
Abstract
Background:
Lung ultrasonography is a new method for diagnosing community-acquired pneumonia. Lung ultrasonography has some advantages over chest X-ray, such as lack of ionizing radiation risk, bedside performance, and cost-effectiveness.
Objectives:
In this study, we aimed to determine the feasibility of lung ultrasonography in emergency settings in children with community-acquired pneumonia.
Methods:
The study included patients younger than 18 years of age with suspicion of community-acquired pneumonia. On the first evaluation, patients with positive clinical and/or chest X-ray findings were defined to have community-acquired pneumonia, and this was accepted as the gold standard. The chest X-rays were evaluated by the chief of the pediatric emergency department, who was blinded to the patients and the lung ultrasonography results. Lung ultrasonography was performed by another pediatric emergency physician who was also blinded to the chest X-ray results and clinical findings such as fever, respiratory distress, rales, and wheezing.
Results:
Of the 91 patients enrolled, 71 (78.0%) were diagnosed with community-acquired pneumonia based on clinical and chest X-ray findings. The median (interquartile range) duration of the lung ultrasonography procedure was 4.0 (3.5–6.0) min. Shred sign, air bronchogram, and hepatization were significantly more frequent in the patients with community-acquired pneumonia (p < 0.01, p < 0.01, and p = 0.01, respectively). Sensitivity and specificity of lung ultrasonography were 78.5% (67.1–87.4) and 95.2% (76.1–99.8), respectively.
Conclusion:
Lung ultrasonography is a useful diagnostic method for children with suspicion of community-acquired pneumonia.
Introduction
Community-acquired pneumonia is one of the leading causes of mortality and morbidity, especially in the pediatric population. Every year, nearly 150 million children below 5 years suffer from pneumonia. 1 In children with uncomplicated and mild pneumonia, the clinical findings are adequate to diagnose. Although most patients benefit from outpatient treatment, some complicated cases require hospitalization. Recent studies report that the hospitalization rate in children with pneumonia is 15.7/100.000. 2 Although the British Thoracic Society and the Infectious Diseases Society of America (IDSA) suggest that routine chest X-ray (CXR) should be performed in all hospitalized cases3,4, previous studies report that CXR has low sensitivity and specificity to determine complicated cases. 5 Moreover, the radiation risk of CXR is another disadvantage for children. 6 Thus, an alternative diagnostic modality is required to diagnose community-acquired pneumonia (CAP).
The use of point-of-care ultrasound has become widespread in pediatric emergency departments (EDs). The ability of bedside performance, lack of ionizing radiation risk, time-saving, and cost-effectiveness are the most advantageous features of point-of-care ultrasonography. 7 Various pathologies such as pneumothorax, pleural effusions, pulmonary contusion, pulmonary emboli, and pneumonia can be identified with lung ultrasound (LUS) in emergency settings. 7 Although recent adult studies report that LUS has higher sensitivity and specificity than CXR for identifying CAP,8,9 there are various data in the literature for the pediatric population.10–13 Hence, we aimed to determine the sensitivity and specificity of LUS for diagnosing CAP in a pediatric ED.
Methods
Setting and design
This study was approved by the Dokuz Eylul University Medicine Clinical Research Ethics Committee (Report number: 2274—GOA; 2015/21-07). Informed consent was obtained from parents or legal guardians of the patients before enrollment in the study. Financial assistance has not been received for this study. Between September 2015 and April 2016, all patients below 18 years with suspicion of CAP were enrolled in this study. Patients with chronic pulmonary disease were excluded based on the probability of scar tissue in lungs. Also, patients with external thoracic wall malformations and thoracic trauma that can preclude optimal evaluation, or congenital lung malformations and patients who did not undergo both CXR and LUS on admission were not included.
If patients had fever (>38°C), signs of respiratory distress, or symptoms of pneumonia (cough, tachypnea, dyspnea, retractions, nasal flaring, grunting, wheezing, and pulse oximetry measurement <90%), 3 CXR was performed for suspicion of CAP. Lung US was performed in all patients. The CXRs were evaluated by the chief of the pediatric ED who was blinded to the patients and the LUS results. The findings of CXR were classified as alveolar, interstitial, mixed pneumonia, or normal and the presence of pleural effusion was also noted (Figure 1).
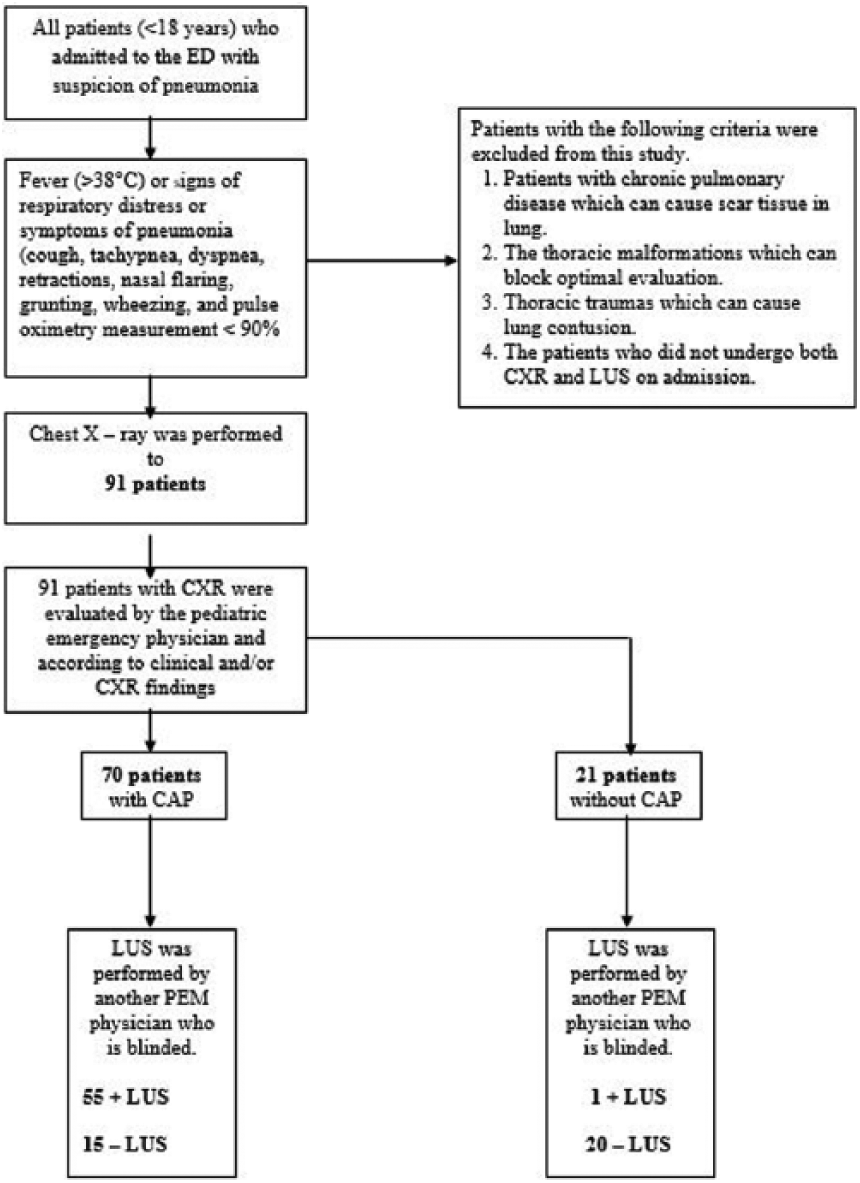
Flow patient diagram of the study.
LUS procedure
LUS was performed by another pediatric emergency physician who had taken course on LUS theory and had at least 150 LUS practice on patients before the study. The LUS operator was blinded to the CXR results and clinical findings. All LUS examinations were performed with a Philips ClearVue 350 (Philips, Andover, MA, USA) ultrasound machine with linear (L12-4 MHz) and curved (C5-1 MHz) probes. The probes were placed vertically, parallelly, and obliquely. The chest portion was divided into three regions (anterior, lateral, and posterior) as areas 1, 2, and 3. 14 The posterior region of the patients was scanned in a sitting position. Each intercostal region, between the first costa and the diaphragm line, was scanned on all three areas. In normal lung tissue, the pleural line causes horizontal reverberation artifacts called “A lines,” which are seen as a series of echogenic parallel lines equidistant from one another below the pleura.
The sliding movement of the pleural surfaces, which is called “lung sliding,” and the A line are essential signs of normal lung tissue (Figure 2). If the pleural line is shredded with an irregular line, it indicates alveolar consolidation and is called shred sign (Figure 3(a)). In the consolidated lung area, the lung tissue can show similar echogenicity to liver tissue, which is called hepatization; also air bronchograms and irregular, hyperechoic, punctiform or linear images may be seen (Figure 3(b)). Patients with shred sign, air bronchogram, or hepatization were diagnosed with alveolar pneumonia. “B lines” arise from the pleural line and appear as vertical hyperechoic images. Detecting more than three B lines indicates interstitial syndrome (Figure 3(c)). Patients with B lines (>3 in intercostal region) were classified as having interstitial pneumonia. Pleural effusion was diagnosed if the patient had sinusoidal and quad signs (Figure 4). The duration of the LUS procedure was also recorded.
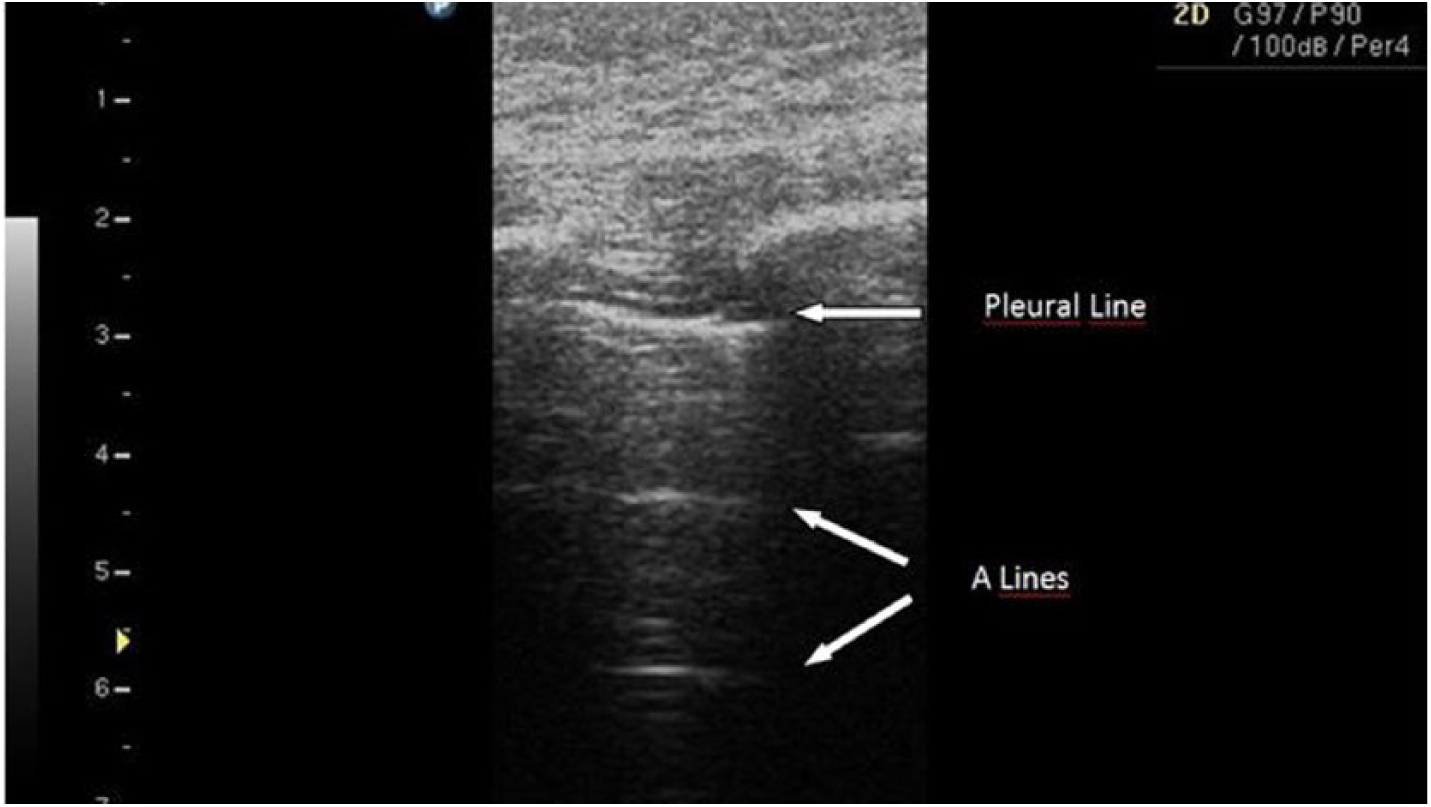
Pleural line and its reverberation artifacts in normal lung tissue.
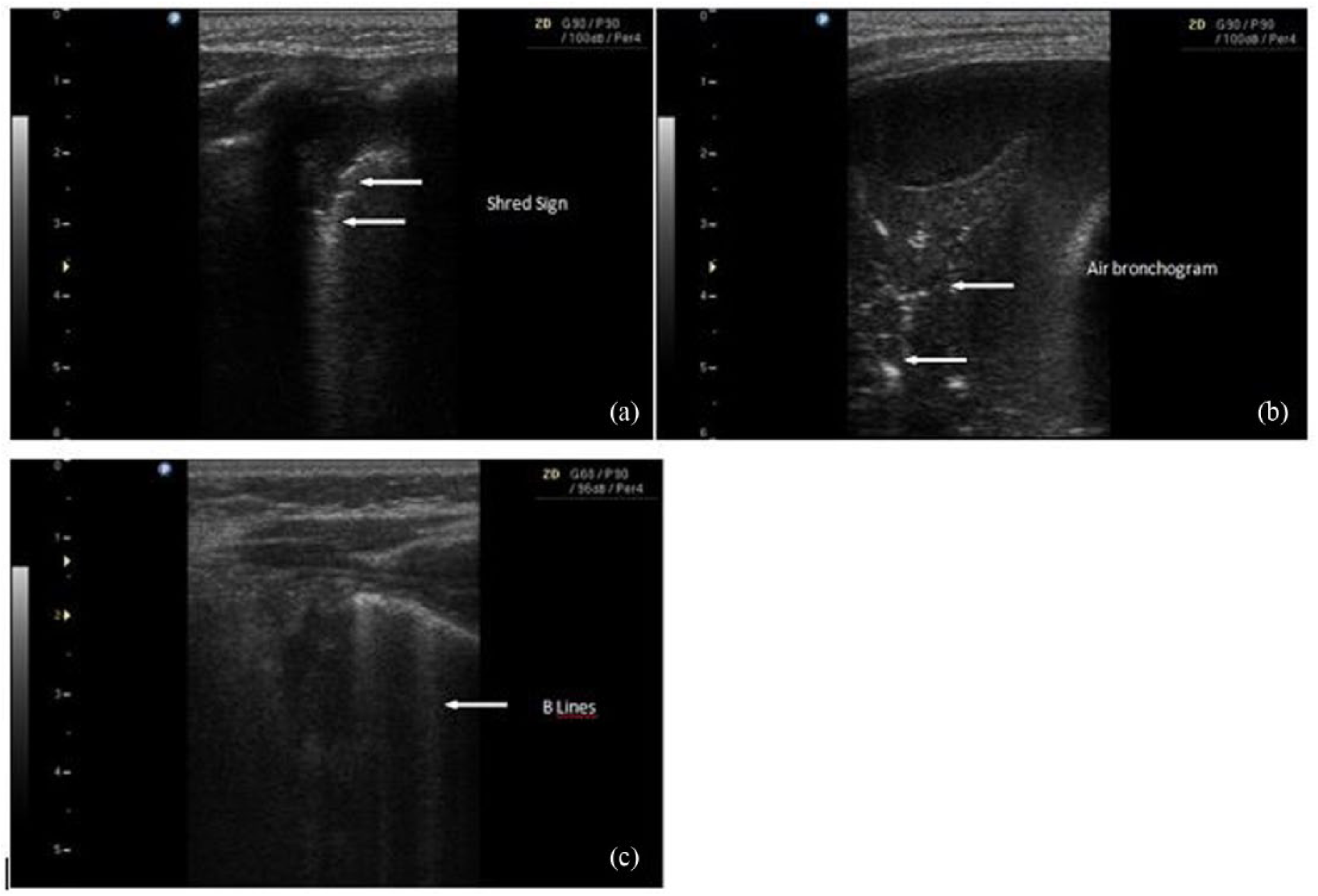
(a) Shred sign illustrates lung consolidation. (b) Lung ultrasound shows hepatization and air bronchograms. (c) B lines are vertical reverberation artifacts which arise from the pleural line and can give the hint of interstitial pneumonia or alveolar edema.
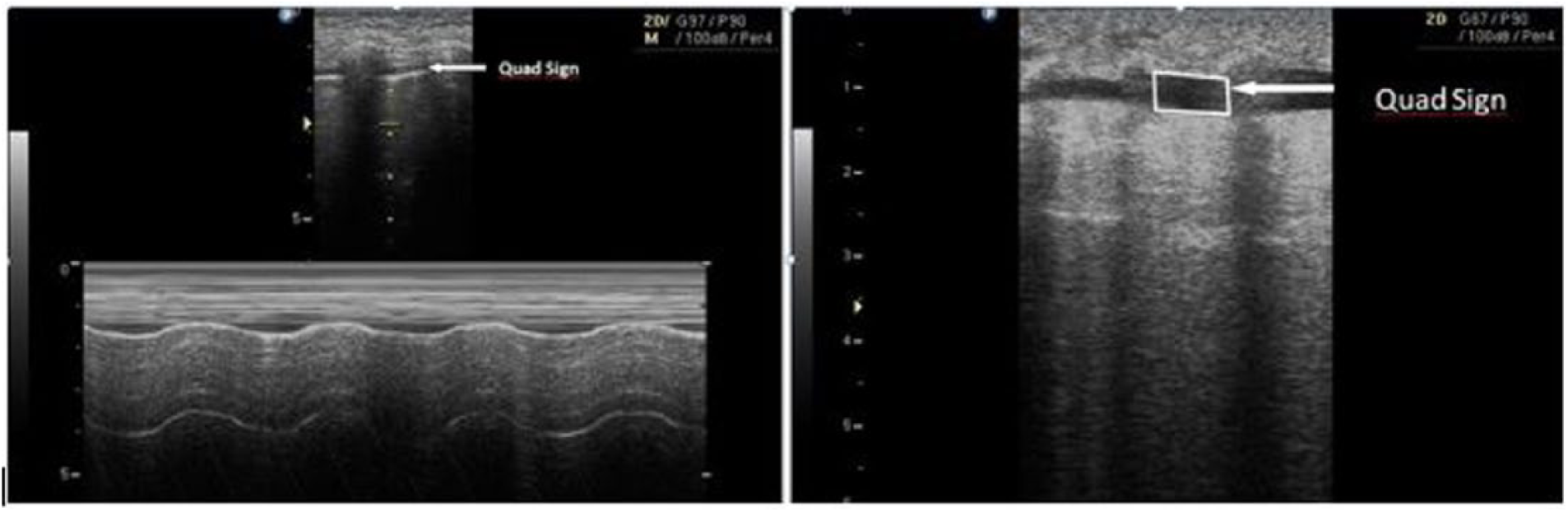
Quad and sinusoidal signs are the findings of pleural effusion.
On first evaluation, patients with positive clinical or CXR findings were defined to have CAP, and this was accepted as the gold standard for this study.
Statistical method
Statistical analysis was performed using SPSS Software 16.0. If the numerical data fit the normal distribution, mean ± standard deviation was calculated, while if the numerical data did not fit a normal distribution, median and the interquartile (IQR) 25th–75th percentile were calculated. Chi-square test was used for the categorical variables. The diagnostic performance of LUS was evaluated for sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). McNemar–Bowker, chi-square, and Cohen’s weighted kappa (κ) tests were used to determine the concordance of LUS and CXR. The strength of the concordance was classified according to k values as poor (<0.0), slight (0.0–0.2), fair (0.2–0.4), moderate (0.4–0.6), substantial (0.6–0.8), or almost perfect (0.8–1.0). Statistical significance was accepted as p < 0.05 for all tests.
Results
This study included 91 patients with suspicion of CAP. The median (IQR) age of the patients was 3.0 (1.0–5.0) years and 59% of the subjects were boys. In all, 70 (78.0%) patients were diagnosed to have CAP according to clinical and CXR findings, 11 (12.0%) patients with fever and respiratory distress were diagnosed to have bronchiolitis, while 10 patients (11.0%) were diagnosed to have asthma. Cough and fever were the most observed symptoms in all patients (84.6% and 73.6%, respectively). There was respiratory distress in 62.6% of patients. The most observed LUS finding was shred sign. The other findings observed in LUS are summarized in Table 1. Shred sign, air bronchogram, and hepatization were significantly more frequent in patients with CAP (p < 0.01, p < 0.01, and p = 0.01, respectively). There was a statistically significant concordance between LUS and CXR in both determination of lesion localization and characterization of the lesion (Tables 2 and 3). Sensitivity and specificity analyses of both imaging modalities in diagnosing CAP are summarized in Table 4. Pleural effusion was determined in nine patients who had both sinusoidal and quad signs. The CXRs of four of these patients were not diagnostic for pleural effusion. The median (IQR) duration of the LUS procedure was 4.0 (3.5–6.0) min.
The findings of LUS that illustrate CAP.
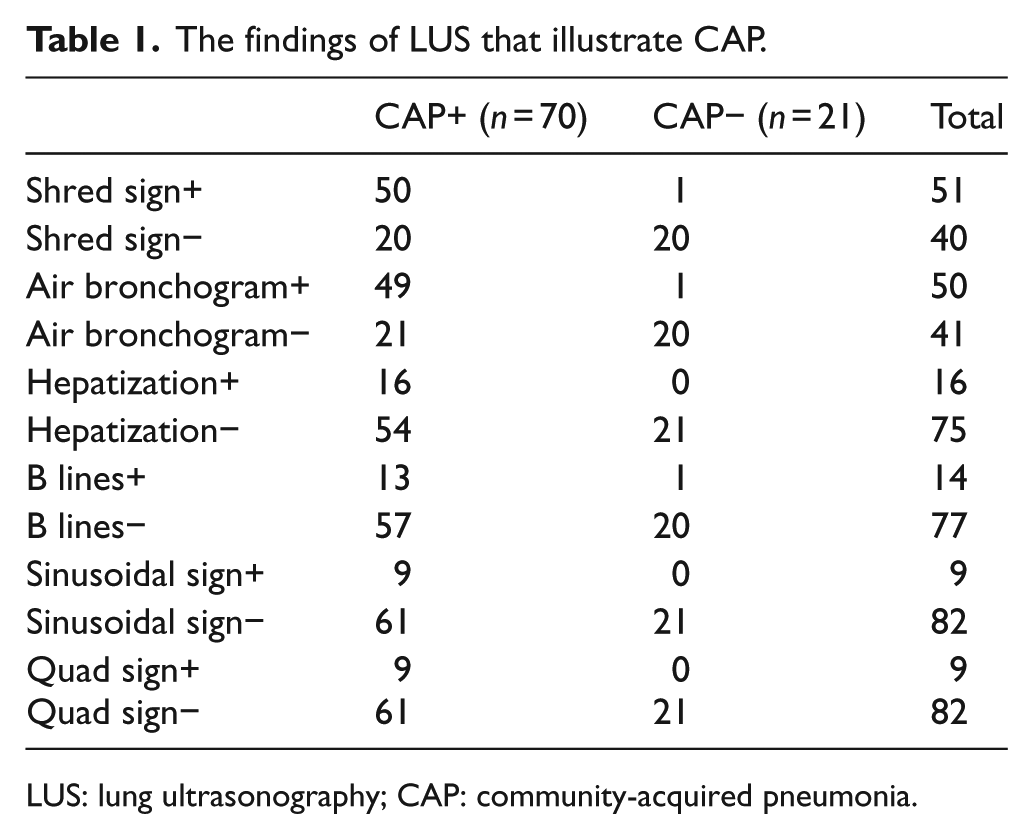
LUS: lung ultrasonography; CAP: community-acquired pneumonia.
The concordance between LUS and CXR in identifying types of pneumonia.
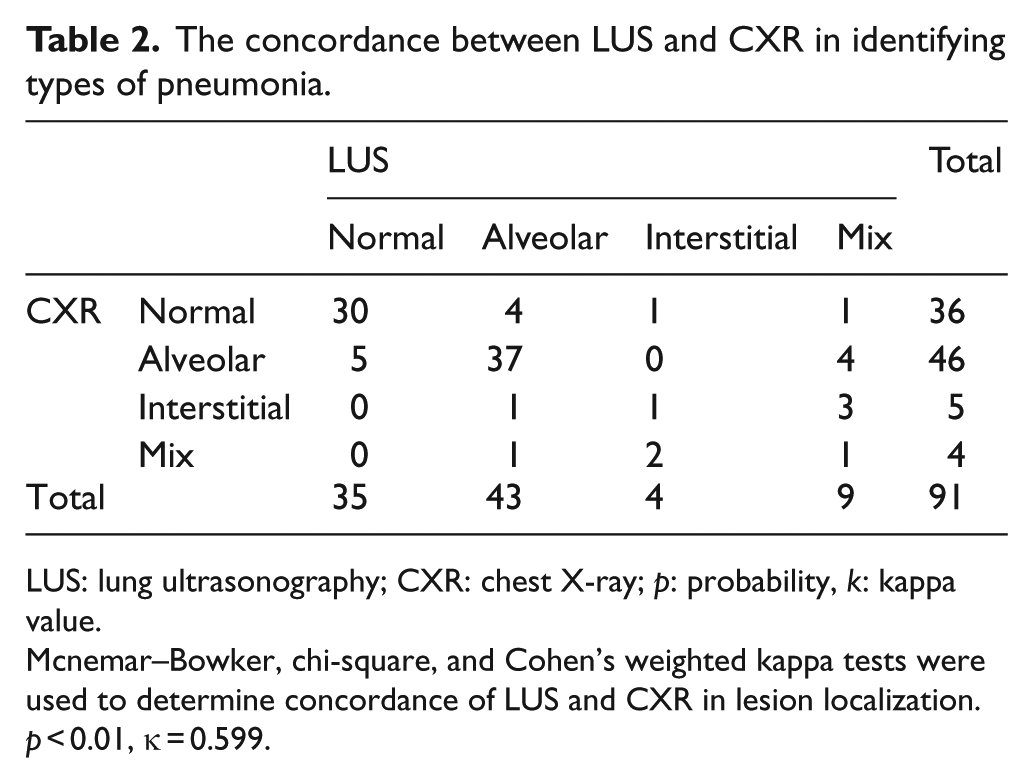
LUS: lung ultrasonography; CXR: chest X-ray; p: probability, k: kappa value.
Mcnemar–Bowker, chi-square, and Cohen’s weighted kappa tests were used to determine concordance of LUS and CXR in lesion localization. p < 0.01, κ = 0.599.
The concordance between LUS and CXR in determination lesion of localization in CAP group.
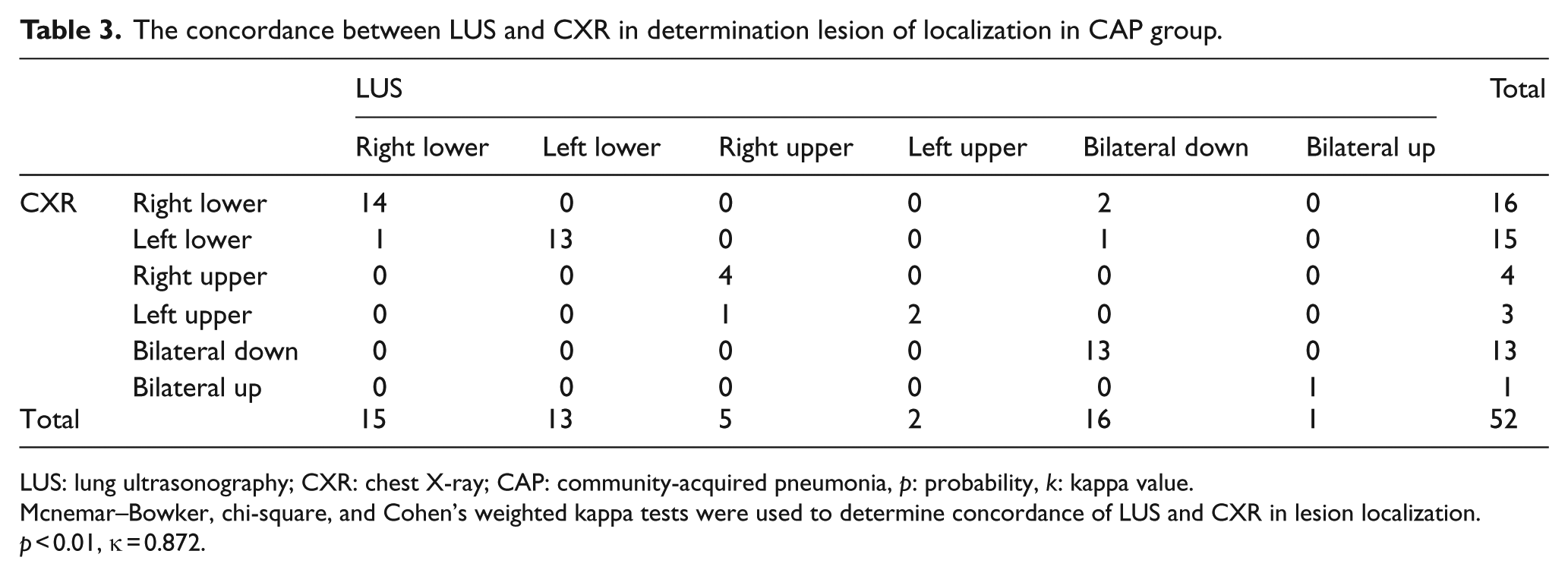
LUS: lung ultrasonography; CXR: chest X-ray; CAP: community-acquired pneumonia, p: probability, k: kappa value.
Mcnemar–Bowker, chi-square, and Cohen’s weighted kappa tests were used to determine concordance of LUS and CXR in lesion localization. p < 0.01, κ = 0.872.
Diagnostic test of LUS in diagnosing CAP.
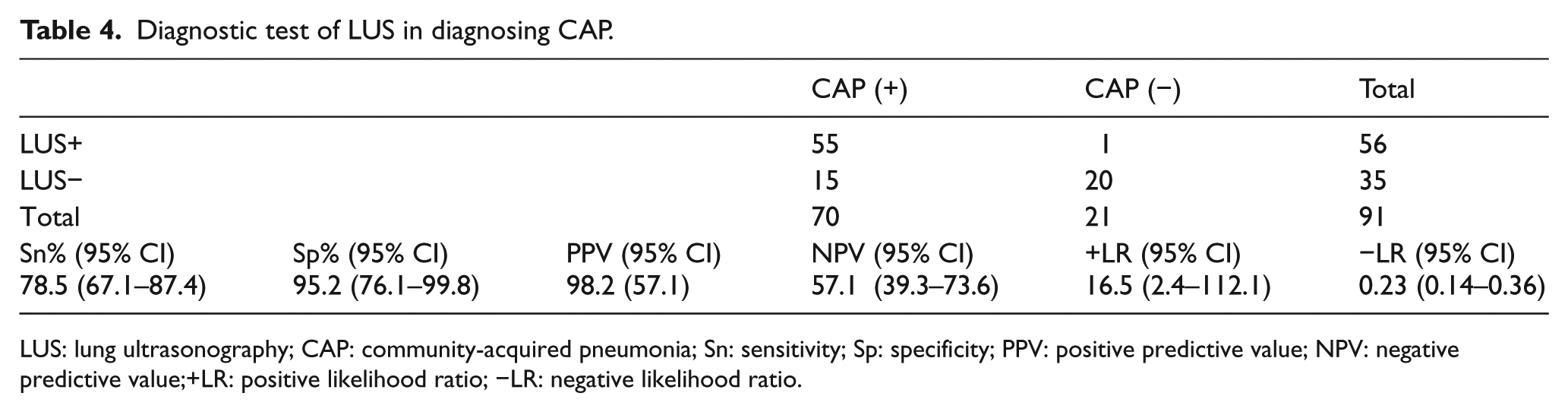
LUS: lung ultrasonography; CAP: community-acquired pneumonia; Sn: sensitivity; Sp: specificity; PPV: positive predictive value; NPV: negative predictive value;+LR: positive likelihood ratio; −LR: negative likelihood ratio.
Discussion
Point-of-care ultrasonography is an imaging technique that has often been used in emergency settings. Current guidelines indicate that CXR or even computed tomography (CT) of thorax could be necessary for diagnosis in patients with CAP who require hospitalization.3,4 Unfortunately, these imaging techniques can cause ionizing radiation and have high cost. The thorax CT in particular is much more disadvantageous than CXR and may often require anxiolysis and sedation additionally. LUS has emerged as an alternative method that is feasible for bedside application and is free of radiation risk. There are many previous studies on adult 8,9,15 and pediatric patients that aimed to determine feasibility or effectivity of the LUS procedure in cases of CAP.10–13,16–18 In adult studies, air bronchogram was defined as the most characteristic LUS finding for pneumonia. 19 Shred signs and air bronchograms were the most frequently observed LUS findings in our study. Hajalioghli et al. 20 reported that there was a perfect concordance between LUS and thorax CT in identifying complicated cases of CAP, but no such concordance was observed for uncomplicated cases if LUS or CXR was performed alone. The other remarkable finding in that study was that LUS plus CXR were in almost perfect concordance in identifying uncomplicated CAP cases. 20 LUS and CXR showed moderate agreement for identifying types of pneumonia when the localization of lesions in both these techniques was almost in perfect agreement and these data were consistent with previous studies.12,20
Although the studies revealed that LUS has higher sensitivity and specificity values for diagnosing CAP than CXR, there are various results (Table 5).11–13,15,17,18,21–24 Among these studies, only Ambroggio et al. 18 accepted thorax CT as the gold standard. In this study, thorax CT was not required in our patients. Hence, we accepted that the last diagnosis based on clinical findings and CXR should be the gold standard. In our study, LUS sensitivity was 78.5% and specificity 95.2%. Although this result is consistent with the study of Ambroggio et al., 18 it is lower compared to other studies that used CXR and clinical diagnosis as the gold standard. In our study, there was a mixed population which consisted of patients having alveolar, interstitial, and mixed pneumonia. Whereas there were consistent clinical findings with pneumonia in patients, some of them did not reveal LUS findings since there was no consolidated lung area yet. This might have affected the sensitivity ratio of our study.
Varied sensitivity and specificity values on previous pediatric studies.
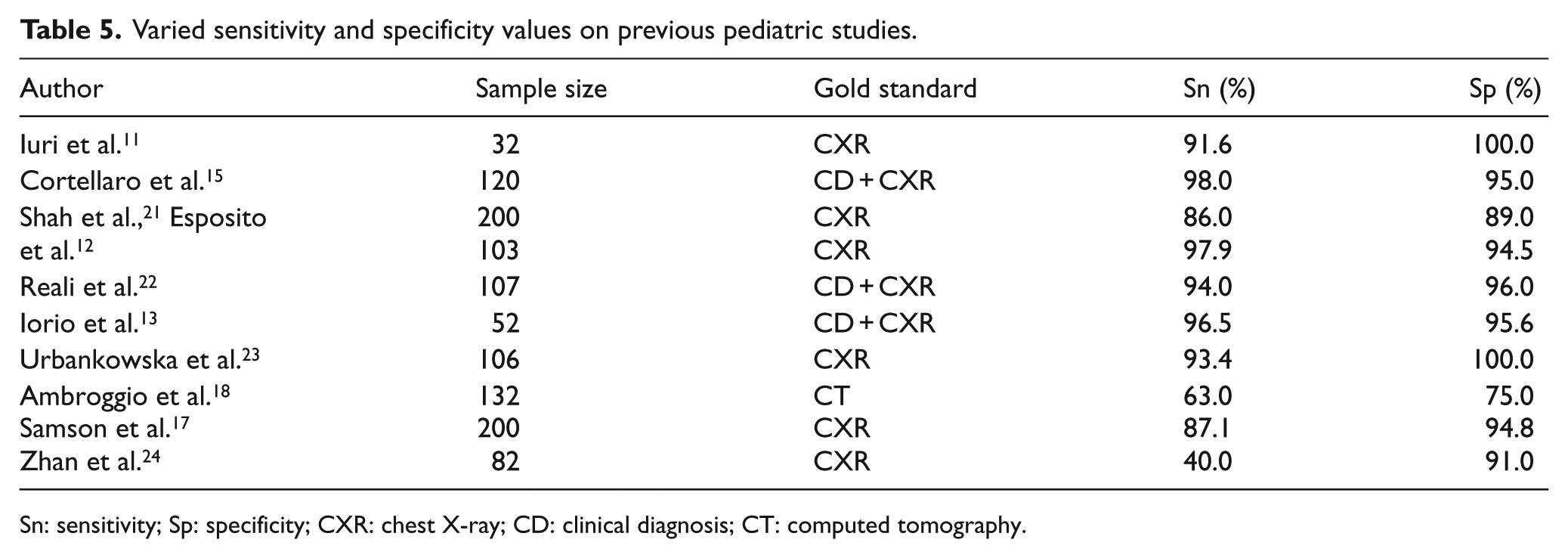
Sn: sensitivity; Sp: specificity; CXR: chest X-ray; CD: clinical diagnosis; CT: computed tomography.
Previous studies have also reported that LUS has high sensitivity and specificity for identifying pleural effusion.11,12,22,23 In our study, LUS detected nine patients with pleural effusions, but CXR could detect only four patients with pleural effusions.
The median duration of the LUS procedure was 4 min, which was shorter than previous reports.21,22 Shah et al. 21 determined that the mean time of the procedure was 7 min, and they could not find statistical differences between two LUS providers according to experience. However, in this study, we could not determine the relationship between the procedure time and the experience of providers.
Like previous studies, this study also has some limitations. First, we could not use thorax CT as a gold standard. Second, we were unable to evaluate the difference between two or more LUS providers. Despite these limitations, this study revealed that LUS has high sensitivity and specificity and is a feasible method for diagnosing CAP. Nevertheless, LUS alone should not be considered diagnostic; it might be more effective when it is used together with physical examination in the diagnosis of CAP. Furthermore, large-scale studies will establish the role of LUS in patients with CAP.
Conclusion
This study indicated that LUS is an effective method to evaluate patients with CAP, and LUS can also be performed within a reasonable time. Therefore, we concluded that LUS is a feasible method for diagnosing patients with CAP in emergency settings.
Footnotes
Acknowledgements
A.Ç., E.U., A.E., D.Y., and M.D. designed and carried out the trial. A.Ç., F.A., H.Ç., and E.U. collected and interpreted data. A.Ç., A.E., D.Y., and M.D. analyzed data. The authors confirm that the paper is original, is not under consideration by another journal, has not been previously published, and has been prepared according to the manuscript guidelines.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from parents or legal guardians of the patients before enrollment in the study.
Ethical approval
This study was approved by the Dokuz Eylul University Medicine Clinical Research Ethics Committee (Report number: 2274 –GOA; 2015/21-07).
Human rights
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee