
Abstract
Background and Objectives:
Patients who overdose on doxylamine, hypnotic agent, usually exhibit good outcomes, but some experience serious complications. Some patients who present with normal creatinine phosphokinase levels in the emergency department later develop rhabdomyolysis during observation. We investigated factors associated with delayed-onset rhabdomyolysis in patients with doxylamine overdoses.
Methods:
Our investigation period was between 1 January 2011 and 29 February 2016. The initial blood samples were obtained for arterial blood gas analysis and measurements of the levels of electrolytes, creatinine phosphokinase, blood urea nitrogen, creatinine, aspartate aminotransferase, alanine aminotransferase, and lactate dehydrogenase. Urine analyses including pH and occult blood analyses were performed. Follow-up samples were obtained at 6 and 12 h after admission. Delayed-onset rhabdomyolysis was defined by a follow-up serum creatinine phosphokinase level greater than fivefold the upper limit of normal (>1000 IU/L). Comparisons of categorical variables between groups were performed using either the χ2 or Fisher exact tests. Continuous variables were compared between groups using the Mann–Whitney U test.
Results:
A total of 337 patients were enrolled. The large amount of ingested doxylamine (odds ratio = 7.002), tachycardia (odds ratio = 2.809), low arterial blood gas analysis pH (odds ratio = 2.267), and presence of occult blood in the urine (odds ratio = 2.048) were significant associated with delayed-onset rhabdomyolysis.
Conclusion:
Laboratory follow-up examinations were required for patients, ingested more than 18 mg/kg doxylamine poisoning, who had pulses exceeding 120 beats/min, had arterial blood gas analysis pH values below 7.3 on blood and urine testing, and/or exhibited the presence of occult blood in the urine, even if the initial creatinine phosphokinase level was normal.
Introduction
Doxylamine is a hypnotic agent and comprises a class of antihistamines with anticholinergic and sleep-inducing effects. The drug is widely used to control symptoms such as insomnia. In Korea, doxylamine can be purchased over the counter, that is, without a prescription.1–6
Patients who overdose on doxylamine usually have good outcomes, although some patients present with anticholinergic symptoms including tachycardia, mental deterioration, nausea, emesis, dizziness, and mydriasis or complications such as rhabdomyolysis, convulsions, acute kidney injury (AKI), and pancreatitis. Rhabdomyolysis after a doxylamine overdose was first reported in 1983, 7 and its incidence ranges from 32% to 77%.3,8,9 If improperly treated, rhabdomyolysis can cause acute renal injury; therefore, it is imperative to determine a method to predict the development of rhabdomyolysis after doxylamine overdose.10–12 Factors known to correlate with the incidence of rhabdomyolysis in patients who have overdosed on doxylamine include the amount of drug ingested, blood-drug concentration, time elapsed from drug ingestion to admittance at the hospital, and the presence or absence of vomiting after drug ingestion, tachycardia, and hematuria at the time of admittance to the emergency department (ED).2,8,9,13–15 We noticed that some patients who presented to the ED with normal creatinine phosphokinase (CPK) levels developed rhabdomyolysis during ED management. These factors are associated with the delayed development of rhabdomyolysis in patients who have overdosed on doxylamine. Therefore, we investigated the factors associated with delayed-onset rhabdomyolysis in doxylamine succinate intoxication patients.
Methods
The investigation was performed prospectively among individuals who visited the EDs of two tertiary teaching hospitals in Seoul, Korea, for the treatment of doxylamine overdoses between 1 January 2011 and 29 February 2016. To define the risk factors for doxylamine-induced rhabdomyolysis, patients who exhibited features that could potentially affect CPK levels (e.g. concurrent ingestion of other drugs and alcohol, seizures before the hospital visit, or any trauma history) and those with renal disease, ischemic heart disease, or muscular disease were excluded. Patients who refused laboratory studies and those with abnormal CPK levels at admission were excluded.
The patient characteristics, time from drug ingestion to arrival at the hospital, amount of doxylamine ingested, and intentionality were noted. The doses of ingestion and intentionality were based on what the patient had stated. Intravenous hydration and urine alkalization were examined, and 50 g of activated charcoal was administered to all patients. The method of conducting urine alkalization was that to administer 1–2 mEq/kg IV sodium bicarbonate bolus, infuse 100 mEq of sodium bicarbonate mixed with 1 L of D5W at 250 mL/h, monitor serum potassium and bicarbonate every 2–4 h to detect hypokalemia or excessive serum alkalinization, and check urine pH regularly (every 15–30 min), aiming for a pH of 7.5–8.5. A further IV bolus of 1 mEq/kg of sodium bicarbonate may be necessary if sufficient alkalinization of the urine is not achieved. The endpoint was set 24 h after reaching urine pH 7.5.
Gastric lavage was performed within 1 h of doxylamine ingestion. The initial blood samples were obtained for arterial blood gas analysis (ABGA) of pH and to measure the levels of electrolytes, CPK, blood urea nitrogen (BUN), creatinine (Cr), aspartate aminotransferase (AST), alanine aminotransferase (ALT), amylase, and lactate dehydrogenase (LDH). Urine was collected, the pH was measured, and occult blood using aution stick was identified.Follow-up samples (for measurements of electrolytes, BUN, Cr, and CPK levels) were obtained 6 h after ED admission. Rhabdomyolysis was defined by a follow-up serum CPK level more than fivefold the upper limit of normal (>1000 IU/L).16–18 We used an electrocardiogram for all patients in order to distinguish themselves from cardiac origin problem, and patients with recent myocardial infarction or stroke were excluded. AKI was defined by an acute increase in serum Cr above the upper limit of normal (>1.23 mg/dL). This study was approved by the Institutional Review Board Committee of our College of Medicine.
The results are described as means ± standard deviations (SDs) or as the frequencies and percentages. Comparisons of categorical variables between groups were performed using either the χ2 or Fisher exact tests. Continuous variables were compared between groups using the Mann–Whitney U test.
To assess delayed-onset rhabdomyolysis risk, multiple logistic regression was used. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using a logistic regression model. For the receiver operating characteristic (ROC) curves, the best cutoff value was defined as the value that optimally predicted the development of rhabdomyolysis; thus, the point yielding the highest sum of the sensitivity and specificity was selected. The p values less than 0.05 were considered to reflect statistical significance.
Results
A total of 355 patients who had overdosed on doxylamine visited the ED during the study period. Of these, 43 patients were excluded based on the exclusion criteria. A total of 312 patients (61 males and 251 females) were ultimately enrolled.
The patients were divided into rhabdomyolysis (n = 87) and non-rhabdomyolysis groups (n = 212) to allow for comparisons of clinical and laboratory characteristics.
In terms of clinical characteristics, no differences were observed regarding age, gender, time from ingestion to arrival at the ED, body temperature, or mental status. The amount of doxylamine ingested was significantly higher (p < 0.001) in rhabdomyolysis group. Significant between-group differences were evident in higher systolic blood pressure (p = 0.022) and more rapid heart rate in rhabdomyolysis group (p = 0.001; Table 1). At admission, the laboratory variables of ABGA pH (p = 0.001) and urinary occult blood presence (p = 0.004) differed significantly between the groups (Table 2).
Clinical variables of patients with doxylamine overdose.
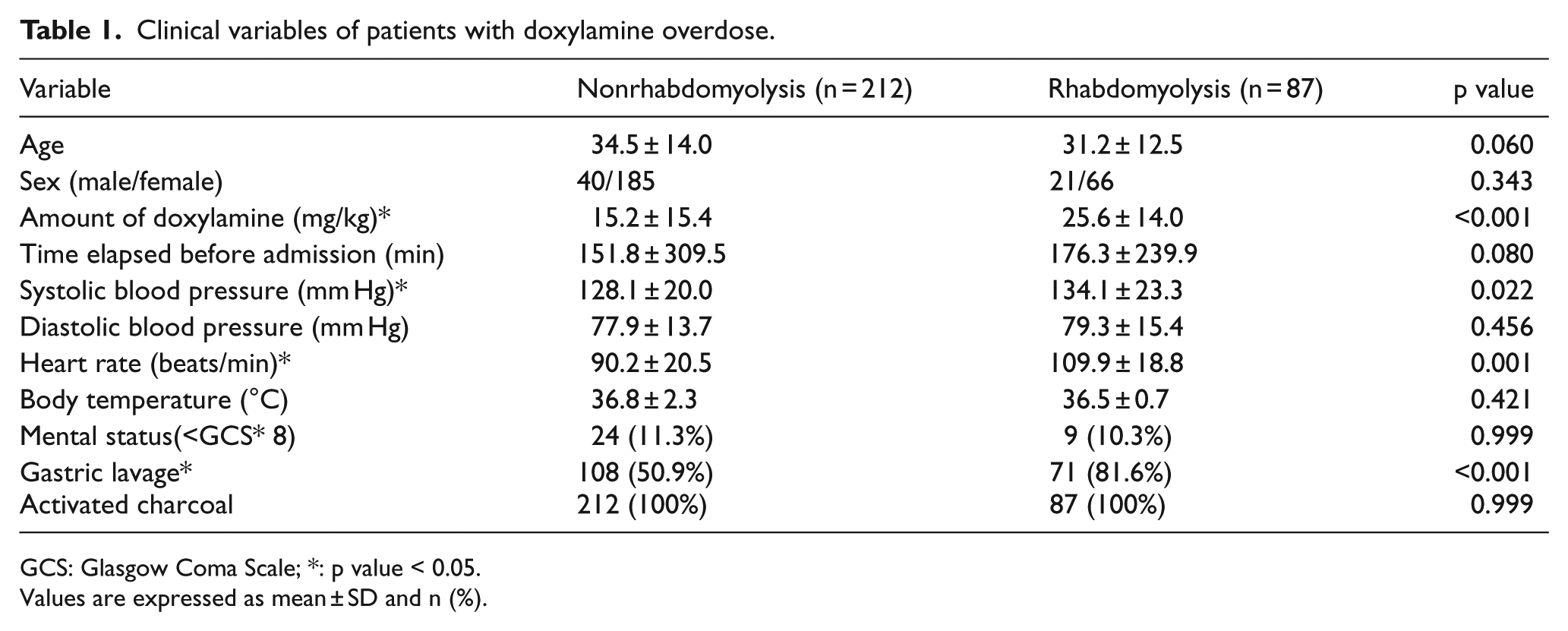
GCS: Glasgow Coma Scale; *: p value < 0.05.
Values are expressed as mean ± SD and n (%).
Laboratory variables of patients with doxylamine overdose.
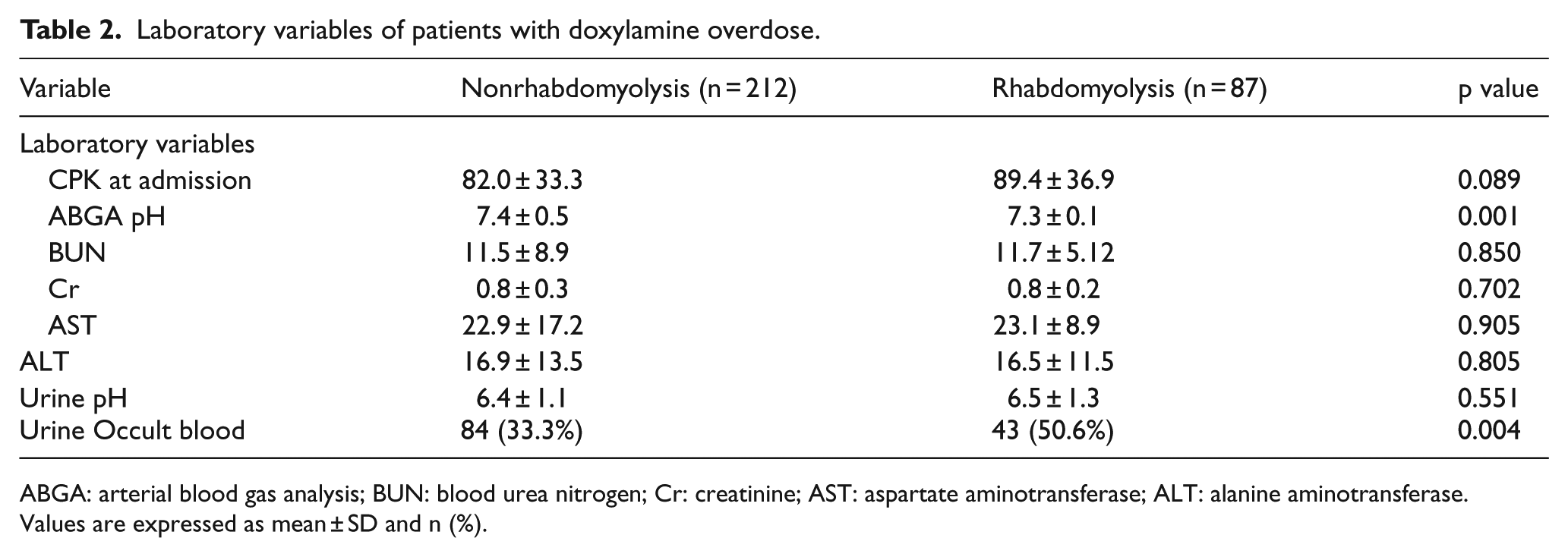
ABGA: arterial blood gas analysis; BUN: blood urea nitrogen; Cr: creatinine; AST: aspartate aminotransferase; ALT: alanine aminotransferase.
Values are expressed as mean ± SD and n (%).
AKI developed in four patients in the rhabdomyolysis group, and one patient required continuous renal replacement therapy (CRRT). The serum Cr levels in the patients with rhabdomyolysis-related AKI were 1.8, 2.1, 2.7, and 2.8 mg/dL, and the peak Cr levels were 2.4, 2.8, 3.0, and 4.1 mg/dL, respectively. The amount of doxylamine ingested was 62.5 mg/kg in the CRRT patients.
To investigate the risk factors of delayed-onset rhabdomyolysis, the amount of doxylamine, systolic blood pressure, heart rate, ABGA pH, and urine occult blood was examined using multivariate logistic regression. The high amount of doxylamine ingested (p < 0.001, OR = 7.002), rapid heart rate (p = 0.003, OR = 2.809), low ABGA pH (p = 0.003, OR = 2.267), and presence of occult blood in the urine (p = 0.005, OR = 2.048) were significantly associated with delayed-onset rhabdomyolysis (Table 3).
Multiple logistic regression predicting delayed-onset rhabdomyolysis in patients with doxylamine poisoning.
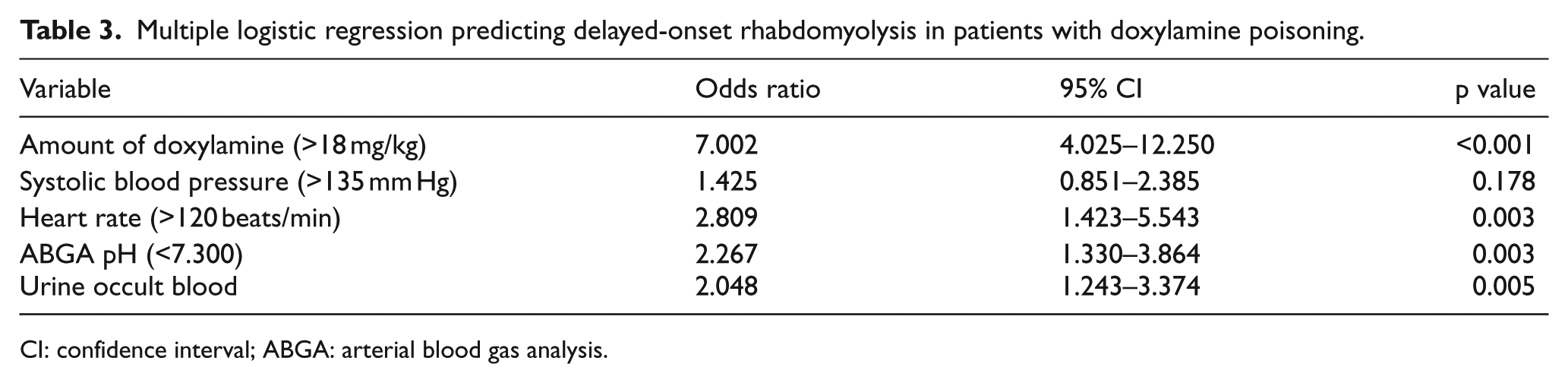
CI: confidence interval; ABGA: arterial blood gas analysis.
Discussion
Doxylamine comprises a class of antihistamines and is commonly used to relieve insomnia. The drug is easily absorbed in the gastrointestinal tract, attains a maximum blood concentration within 2–3 h of ingestion, and has a half-life in the body of approximately 10 h. Approximately 60% of the absorbed drug is directly excreted in the urine, and the remaining 40% is metabolized in the liver followed by urinary excretion. 13
The symptoms of an overdose are principally attributable to the anticholinergic effects of the drug on the autonomic and central nervous systems and the heart. 18 Overdoses are usually asymptomatic (70%–80%), although confusion (12%), mydriasis (10%), tachycardia (4%), coma (3%–4%), and convulsions (2%–3%) have been reported, and rhabdomyolysis is rare (1%–2%). However, in urban EDs in Korea, doxylamine overdoses account for 25% of drug overdose-related visits, 2 and the incidence of overdose-associated rhabdomyolysis ranges from 32% to 77%.3,9,10 Rhabdomyolysis is a complication that develops in patients who have overdosed on doxylamine. This drug exerts a direct toxic effect on myocytes.19–21 An increase in endomysial permeability caused by the activation of phospholipase A induces an outflow of materials from, and sodium flow into, myocytes. The increased sodium ion concentration damages the Na+-K+-adenosine triphosphatase (ATPase) pump, which triggers increased adenosine triphosphate (ATP) consumption and impairment of intercellular calcium ion transport. As calcium ions accumulate within the cells, neutral proteases are activated, triggering cell damage. Rhabdomyolysis refers to a series of syndromes with symptoms of skeletal muscle injury and material outflow from myocytes. The associated complications include hypocalcemia, hyperuricemia, hyperkalemia, hyperphosphatemia, myoglobinuria, disseminated intravascular coagulation, metabolic acidosis, acute cardiomyopathy, respiratory failure, AKI, compartment syndrome, and peripheral neuritis. AKI is a severe complication with a poor prognosis.3,4,10–12,18 The frequencies of AKI as a complication of rhabdomyolysis vary greatly in different reports. For example, Tintinalli et al. 12 reported that complications featuring AKI were observed in 46% of patients with rhabdomyolysis, whereas the incidences of AKI in Korean populations are 16% based on the work of Lee et al. 4 and 58% on the study of Kim et al. 15
In one report, approximately 4% of patients with AKI due to rhabdomyolysis required hemodialysis. 22 AKI caused by rhabdomyolysis is attributable to fact that myoglobin per se is toxic to kidney tubules, that is, myoglobin casts form within the tubules. 22
In our study, the CPK levels were re-checked after 6 h in patients with initially normal CPK levels. Delayed-onset rhabdomyolysis developed in approximately 25% of patients. Most of these patients were discharged when their symptoms improved after fluid therapy alone, and they did not develop severe complications. However, two patients with AKI required CRRT.
We analyzed laboratory and clinical data to identify the associations between these parameters and the development of delayed-onset rhabdomyolysis after a doxylamine overdose. The amount of doxylamine ingested, heart rate, systolic blood pressure, initial ABGA pH, and presence of occult blood in the urine all exhibited significant associations with rhabdomyolysis upon univariate analyses. Upon multivariate regression, the amount of doxylamine ingested, initial ABGA pH, presence of occult blood in the urine, and heart rate (tachycardia) reliably predicted delayed-onset rhabdomyolysis development after a doxylamine overdose.
Jo et al. 9 found that only the amount of doxylamine ingested was a risk factor for the development of rhabdomyolysis at the initial examination, and the cutoff dose was 20 mg/kg. Kim et al. 15 reported that an intake of 13 mg of doxylamine per kilogram caused rhabdomyolysis. We found that when more than 18 mg/kg of the drug was ingested, the incidence of rhabdomyolysis increased by more than sevenfold.
Patients with tachycardia (120 beats/min) exhibited a higher ORs of rhabdomyolysis. Sinus tachycardia is among the earliest and most reliable signs of doxylamine-mediated muscarinic receptor blockade. 23 In addition, patients with an ABGA pH below 7.3 at the time of the ED visit were significant associated with delayed-onset rhabdomyolysis, and those with occult blood in the urine were at an over higher risk. Park et al. reported that hematuria developed after 18 h in patients who had ingested doxylamine was correlated with the amount of drug ingested per kilogram of body weight and occurred at approximately the time when the CPK level reached a maximum.
We recognize the limitations of the interpretation of our findings. Data were collected via self-reporting, and we calculated the drug amount as mg/kg; therefore, differences were present between the drug amounts and the actual drug blood levels.
Conclusion
Rhabdomyolysis is a common complication in patients who visit EDs after overdosing with doxylamine. However, if no troublesome symptoms are apparent and examination results are normal, most patients reject further treatment or hospitalization for symptom monitoring and discharge themselves. However, even if the CPK level is normal at the time of the ED visit, it is necessary to determine whether more than 18 mg/kg doxylamine has been ingested. If the pulse exceeds 120 beats/min, the ABGA pH is less than 7.3 on blood and urine testing, and if occult blood is present in the urine, the patient is at risk of delayed-onset rhabdomyolysis, and further observation and laboratory follow-up should be considered.
Footnotes
Acknowledgements
All authors have made substantive contributions to the study, and all authors endorse the data and conclusions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The authors confirm that guidelines on patient consent have been met and any details of informed consent obtained.