
Abstract
Neurofibromatosis 1 is an autosomal dominant disorder characterized by cafe-au-lait spots, cutaneous neurofibroma, and bony deformities. Vascular abnormality such as stenosis, aneurysm, or rupture associated with neurofibromatosis 1 is rare. Rupture of vertebral artery aneurysm into the thoracic cavity is extremely rare. The outcomes of patients with aneurysmal ruptures are very poor when spontaneous hemothorax occur. A 31-year-old woman presented to the emergency department with left shoulder pain and with both lower chest wall pain and left supraclavicular area swelling. The chest computed tomography scan revealed about 4-cm pseudo-aneurysm probable arising from the left vertebral artery with large hematoma at left supraclavicular area. Neurofibromatosis 1 is generally being regarded as a benign disease but has the potential for serious vascular complications. When aneurysms were ruptured, cervical hematoma, hemothorax, or hypotension was developed. It is potentially a life-threatening condition, so it must require emergent management. Emergency physicians must remember the relation of neurofibromatosis 1 and serious vascular complications and ensure rapid access to rule out vascular lesions, so as to prevent the life-threatening condition.
Case history
A 31-year-old woman presented to the emergency department (ED) with left shoulder pain and with both lower chest wall pain and left supraclavicular area swelling for 2 days. Two days prior to admission, she had slipped on her right side on an icy road. She took analgesics for pain control but the symptom did not improve and the supraclavicular area swelling worsened. According to her medical history, she had been diagnosed with neurofibromatosis 13 years ago and had undergone a neck mass excision operation due to neurofibroma. The initial examination revealed tenderness over the left shoulder and anterior neck, with 4 × 4 cm neck mass. A plain cervical spine and radiograph of both shoulders showed soft tissue swelling, left cervical area (Figure 1). 30 min after ED admission, she complained with swelling of her left-side neck, mild dyspnea and left lower chest wall pain. We obtained computed tomography (CT) scan of the chest to evaluate cause of dyspnea and lower chest wall pain (Figure 2).

A plain radiograph of both shoulders showed soft tissue swelling, left cervical area.
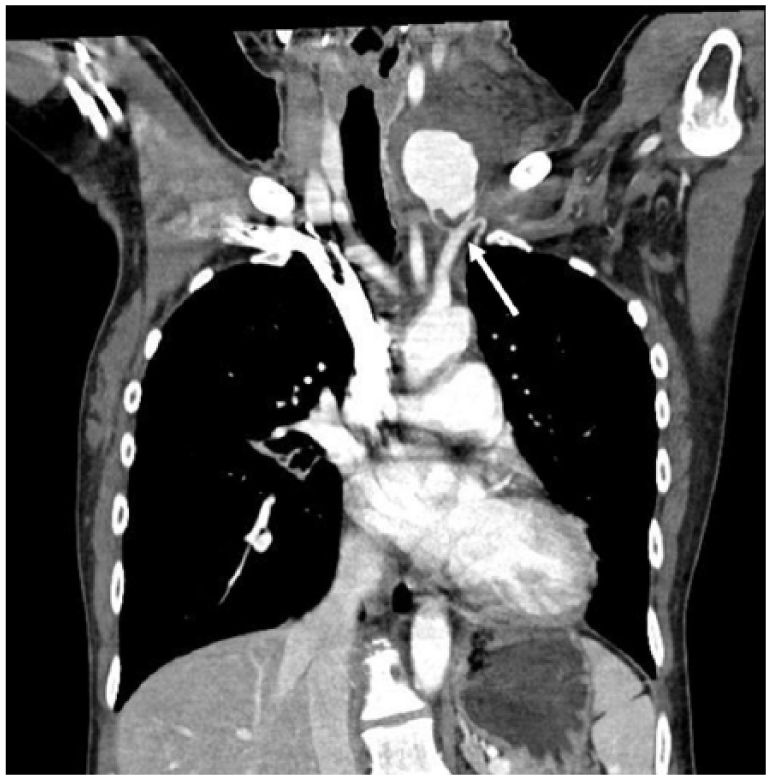
The chest computed tomography.
Questions
What were the CT findings?
What was the diagnosis?
Why emergency physician should be aware of this finding?
Answers
The chest CT scan revealed about 4-cm pseudo-aneurysm probable arising from the left vertebral artery with large hematoma at left supraclavicular area (indicated by an arrow in Figure 2).
The diagnosis was ruptured aneurysm of left vertebral artery in neurofibromatosis.
Neurofibromatosis 1 (NF 1) is generally being regarded as a benign disease but has the potential for serious vascular complications. When aneurysms were ruptured, cervical hematoma, hemothorax, or hypotension was developed. It is potentially a life-threatening condition, so it must require emergent management.
Discussion
NF 1 is an autosomal dominant disorder characterized by café-au-lait spots, cutaneous neurofibroma, and bony deformities. Vascular abnormality (arterial lesions) such as stenosis, aneurysm, arteriovenous fistula, or rupture associated with NF 1 is rare. 1 Most cases of extracranial vertebral artery aneurysm occur in trauma involving the craniocervical region. 2 The 1% of extracranial vertebral artery aneurysms are pseudoaneurysms, which develop as a result of complete or incomplete disruption of the arterial wall due to trauma-induced necrosis of the arterial wall (especially intima). 3 The majority of aneurysm occurred on the left and in females. Patients typically presented with radiculopathy, neck pain, or neck mass. When aneurysms were ruptured, cervical hematoma, hemothorax, or hypotension was developed. 4 The outcomes of patients with aneurysmal ruptures are very poor if bleeding extends into the thoracic cavity. 5
Emergency physicians must remember the relation of NF 1 and serious vascular complications and ensure rapid access to rule out vascular lesions, so as to prevent the life-threatening condition.
Footnotes
Acknowledgements
The manuscript, as submitted or its essence in another version, is not under consideration for publication elsewhere and will not be published elsewhere while under consideration by the Hong Kong Journal of Emergency Medicine. The authors have no commercial associations or sources of support that might pose a conflict of interest. All authors have made substantive contributions to the study, and all authors endorse the data and conclusions. D.H.L. and Y.H.C. participated in the design of the study and conceived the study. D.H.L. and Y.H.C. were major contributors in writing the manuscript. J.H.L., K.K., and J.Y.L. helped to draft and revise the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Informed consent
Written informed consent was obtained from the patient for anonymized information to be published in this article.
Ethical approval
Ethical approval was not required as no patient’s identifiable data were disclosed.
Human rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.