
Abstract
Background:
Acute epiglottitis is a potentially life-threatening condition, but its clinical manifestations are usually nonspecific.
Objectives:
We investigated the clinical differences between patients with and those without acute epiglottitis and identified the risk factors of patients with acute epiglottitis who may develop airway compromise.
Methods:
We studied patients suspected of having acute epiglottitis in the emergency department. All patients received fibre-optic laryngoscopy performed by an otorhinolaryngologist and were subsequently divided into two groups: patients with acute epiglottitis and those without.
Results:
Of the 311 adult patients, 108 were diagnosed with acute epiglottitis. In the nonepiglottitis group, more complaints of fever (p < 0.001), cough (p < 0.001), and rhinorrhoea (p = 0.048) and more systemic comorbidities were reported. People with acute epiglottitis generally had a higher prevalence of head and neck tumours (p = 0.015), odynophagia (p = 0.037) and an elevated white blood cell level (p < 0.001). The proportion of patients with cardiovascular disease (p = 0.014) or diabetes mellitus (p = 0.019), drooling (p = 0.026) or sore throat (p = 0.042), a high respiratory rate (p = 0.009), an elevated white blood cell level (p = 0.002) and a higher C-reactive protein level (p = 0.005) was higher among those who required airway intervention.
Conclusion:
Clinical manifestations alone were insufficiently reliable for diagnosing acute epiglottitis but could predict disease severity. Laryngoscopy should be performed as soon as possible once a patient is suspected of having acute epiglottitis.
Introduction
Acute epiglottitis (AE) is an inflammation of the epiglottis and adjacent supraglottic structures. Historically, AE was described as a disease of adults; however, it was subsequently reported more frequently in children and considered primarily a paediatric disease from the 1960s onwards. 1 However, the recent widespread use of the haemophilus vaccination has produced a drastic decline in the number of children with epiglottitis, and the disease is once again more common in adults.2,3
AE in adults seems to differ from that observed in children. Most adult patients with AE have a concomitant underlying medical condition at diagnosis. In contrast to the swelling observed in AE in children, the swelling in adults with AE often occurs not only in the epiglottis but also in the surrounding supraglottic area. 4
Prompt diagnosis of AE is vital to prevent a subsequent life-threatening airway obstruction. Currently, AE is diagnosed through direct visualisation of an inflamed epiglottis. Therefore, early diagnosis of AE is challenging for physicians when an otolaryngology consultation or flexible laryngoscopy is unavailable.
Previous studies have investigated patients with a confirmed AE diagnosis to identify the risk factors and clinical features. However, the diagnostic validity of the clinical parameters for identifying patients with definite AE is rarely discussed. Therefore, we investigated patients suspected of having AE in the emergency department (ED) to assess the clinical differences between patients with AE and those without.
Methods
Patient selection and data collection
In the ED of Chi-Mei Medical Center, all patients suspected of having epiglottitis are referred to otolaryngologists for flexible laryngoscopies. Between February 2010 and July 2012, we reviewed all ED requests for otolaryngologist consultations and collected data on patients who were reported to potentially have epiglottitis after clinical assessment. Patients referred from the otorhinolaryngology outpatient department with a confirmed AE diagnosis were also included. All patients included in our study underwent flexible laryngoscopies performed by otolaryngologists, and the results of the flexible laryngoscopies were considered the diagnostic standard for epiglottitis. AE was diagnosed on the basis of inflammation involving the epiglottis, vallecula, arytenoids and aryepiglottic fold.
For each patient, we collected the following information: patient characteristics, comorbidities, initial vital signs at ED arrival, presenting symptoms, laboratory tests, image studies with formal radiology reports, the requirements for airway management, ward or intensive care unit (ICU) admission, and mortality. We defined medical conditions on the basis of abnormal vital signs, laboratory results and image studies as follows: tachycardia, a heart rate greater than 100 bpm; fever, a temperature greater than 38°C; tachypnoea, a respiratory rate greater than 20 breaths/min; desaturation, an oxygen saturation determined using a pulse oximeter less than 90%; leucocytosis, a white blood cell (WBC) count greater than 10,000/μL; elevated C-reactive protein (CRP), a level greater than 3 mg/dL; and positive results for neck radiographs (official radiographic reports that indicated suspicion of epiglottitis). All patients were assessed by emergency physicians for the appearance of respiratory distress. The decision to establish an artificial airway was made on the basis of the patients’ clinical presentations and the patency of the airway ascertained through flexible laryngoscopy. This study was reviewed and approved by the Institutional Review Board of Human Research, Chi-Mei Medical Center.
Statistical analysis
Statistical analysis was performed using SPSS 12.0 (SPSS Inc., Chicago, IL, USA). We applied chi-square and Fisher’s exact tests to ascertain the differences in categorical variables and used Student’s t test to ascertain the differences in continuous variables between the groups of patients.
Results
We collected data on 291 consecutive patients suspected of having AE during the study period. Of the patients, 108 were confirmed as having AE after flexible laryngoscopy. Among the patients with AE, 67 were men and 41 were women, representing a male-to-female ratio of 1.6:1. The median age was 44 years.
A total of 34 patients with AE had concomitant medical conditions at diagnosis, among which diabetes mellitus, cardiovascular diseases (including hypertension, coronary artery disease, congestive heart failure and peripheral arterial occlusive disease) and head and neck tumours were the three commonest. By contrast, 77 patients without AE had concomitant diseases. We compared the systemic comorbidities between the patients with and those without AE (Figure 1) and determined that patients with AE had a higher prevalence of head and neck tumours (AE vs non-AE: 10% vs 3%, p = 0.015). By contrast, more patients without AE had concomitant cardiovascular disease (AE vs non-AE: 11% vs 21%, p = 0.035), dementia or stroke (AE vs non-AE: 3% vs 9%, p = 0.034), or asthma or chronic pulmonary obstructive disease (AE vs non-AE: 0% vs 7%, p = 0.007).
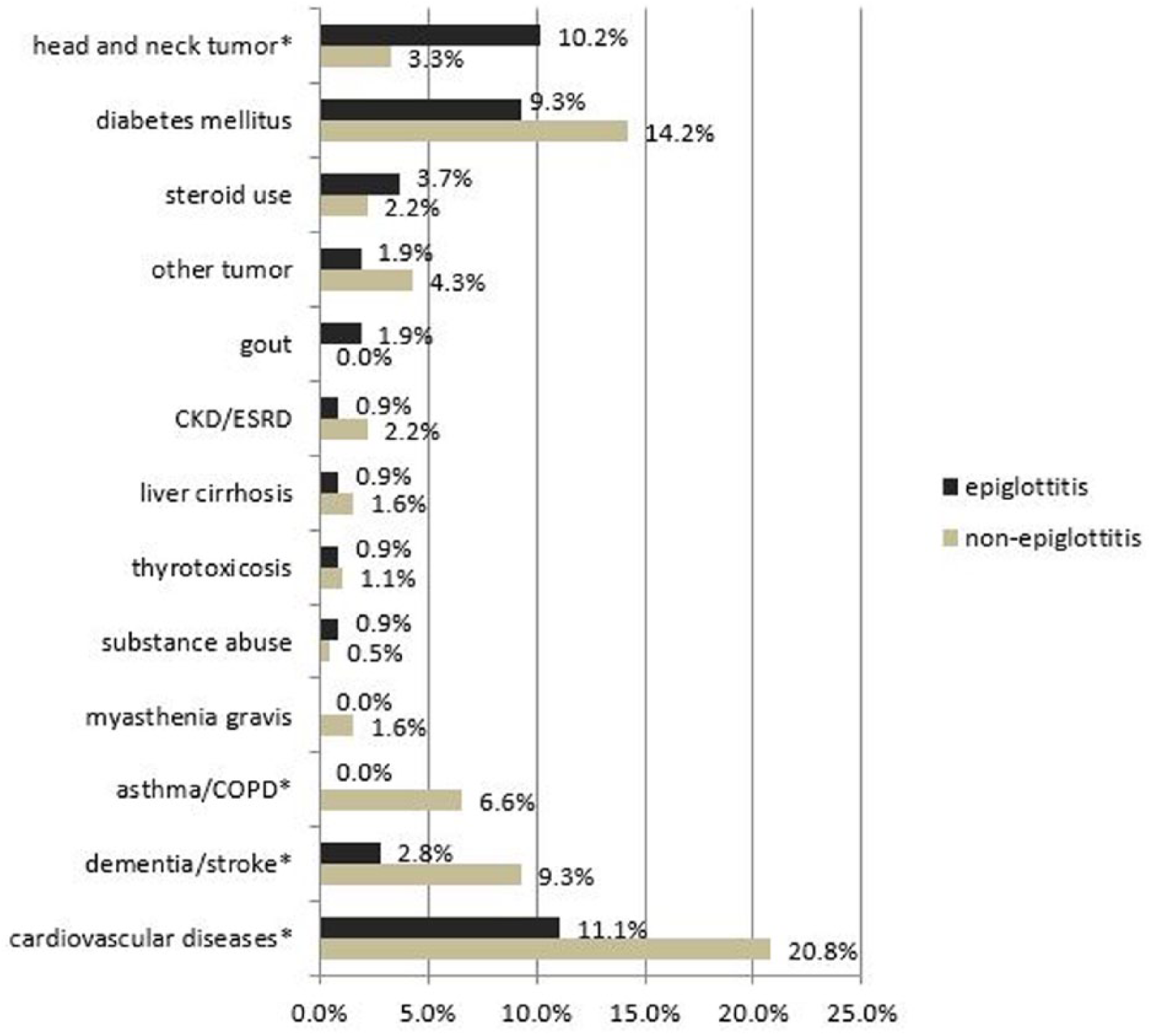
Systemic comorbidities in patients with and without AE.
The mean duration of symptoms before arrival at the ED was 2 days. Sore throat was the commonest symptom (81.5%), followed by odynophagia (49.1%). However, compared with the non-AE group, only odynophagia was statistically significantly more common in patients with AE (AE vs non-AE: 49% vs 37%, p = 0.037). Conversely, patients without AE had higher rates of fever (23% vs 37%, p < 0.001), cough (15% vs 36%, p < 0.001) and rhinorrhoea (5% vs 12%, p = 0.048).
The neck radiographs were positive for epiglottitis in 61 of the 103 patients with AE and 46 of the 177 patients without AE, yielding a sensitivity of 59%, specificity of 74%, positive predictive value of 57% and negative predictive value of 76%.
The patients with AE had a higher prevalence of leucocytosis (AE vs non-AE: 72% vs 43%, p < 0.001) and a higher WBC count (12,200 vs 9500/μL, p < 0.001) than did the patients without AE, but the prevalence of elevated CRP levels was similar between the two groups (Table 1).
Comparison of clinical manifestations in patients with and without AE.
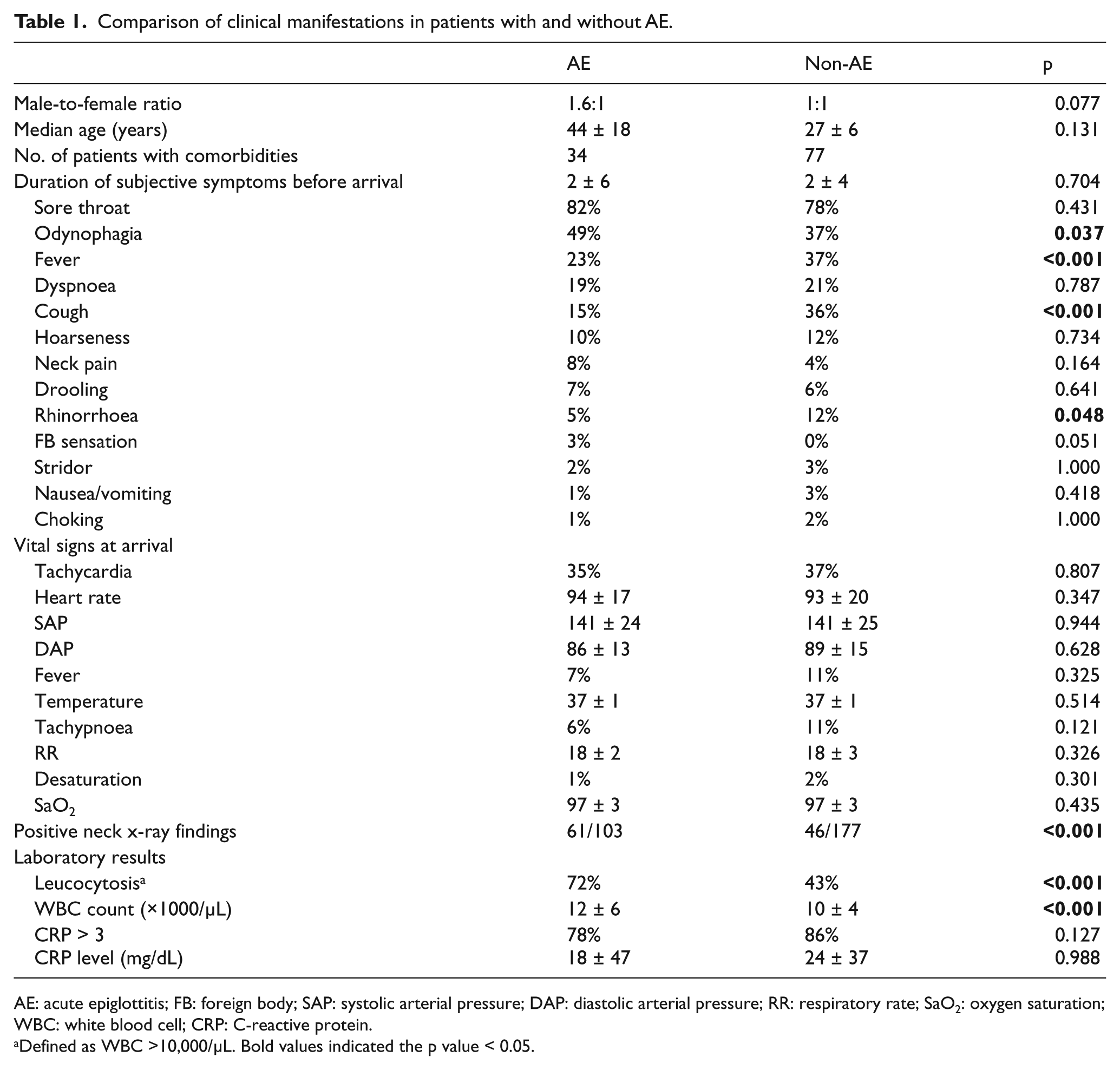
AE: acute epiglottitis; FB: foreign body; SAP: systolic arterial pressure; DAP: diastolic arterial pressure; RR: respiratory rate; SaO2: oxygen saturation; WBC: white blood cell; CRP: C-reactive protein.
Defined as WBC >10,000/μL. Bold values indicated the p value < 0.05.
Of the patients diagnosed with AE, 99% were administered antibiotics. Amoxicillin with clavulanic acid was the commonest empiric regimen, prescribed for 83.3% of the patients; 93% of them underwent corticosteroid therapy. Two patients had already undergone tracheostomies at diagnosis, and 30 of the remaining 106 patients required urgent airway interventions, including 9 orotracheal intubations, 20 nasotracheal intubations and 1 emergent tracheostomy. The median intubation period was 5 days. The outcome and dispositions of the patients with AE are shown in Figure 2.
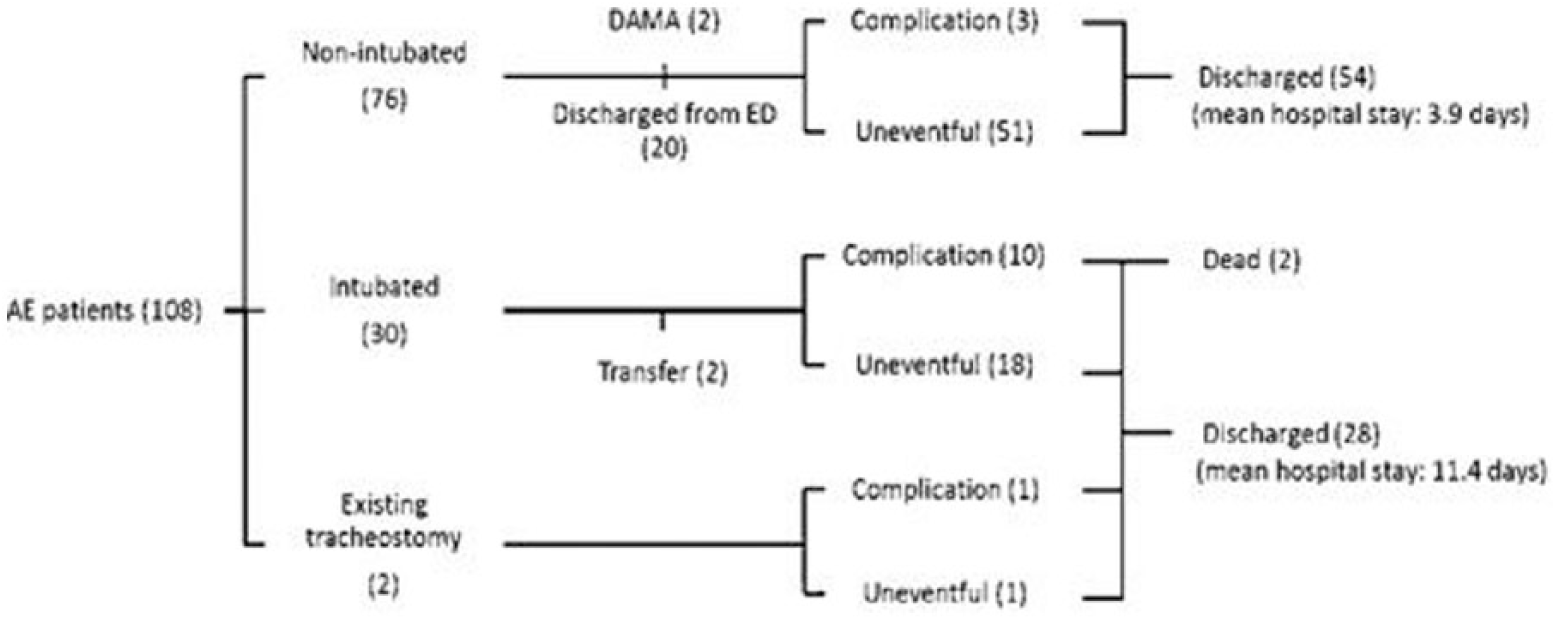
The outcome and dispositions of the AE patients.
Two patients were discharged against medical advice, and two patients were transferred to another hospital. Of the remaining 104 patients, 20 were discharged from the ED with uneventful outcomes, 50 were admitted to the ward and 34 required ICU admission. Complications were documented in 14 patients, including 6 deep neck infections, 3 pulmonary abnormalities (pneumonia, pneumothorax and pulmonary embolism), 2 epiglottic abscesses, 1 bleeding tumour, 1 oesophageal laceration and 1 cerebral infarction. Two patients expired: one with concomitant buccal cancer developed tumour bleeding and a deep neck infection and the other patient had a history of thyroid cancer and developed pneumothorax and a deep neck infection. Of those who had complications but could be discharged, the mean hospital stay was 13.6 (standard deviation (SD) = 6.92) days. Patients without complications had a mean hospital stay of 6.3 (SD = 2.66) days.
Because two of the patients with AE had pre-existing tracheostomies, we divided the remaining 106 patients with AE into two groups: those who received airway intervention and those who did not. Comparing the clinical characteristics of the two groups revealed that patients with AE who required artificial airways had a higher prevalence of cardiovascular diseases and diabetes mellitus (Figure 3). In addition, patients who required artificial airways had a higher prevalence of sore throat, drooling, tachypnoea and leucocytosis as well as higher WBC counts and higher CRP levels (Table 2).
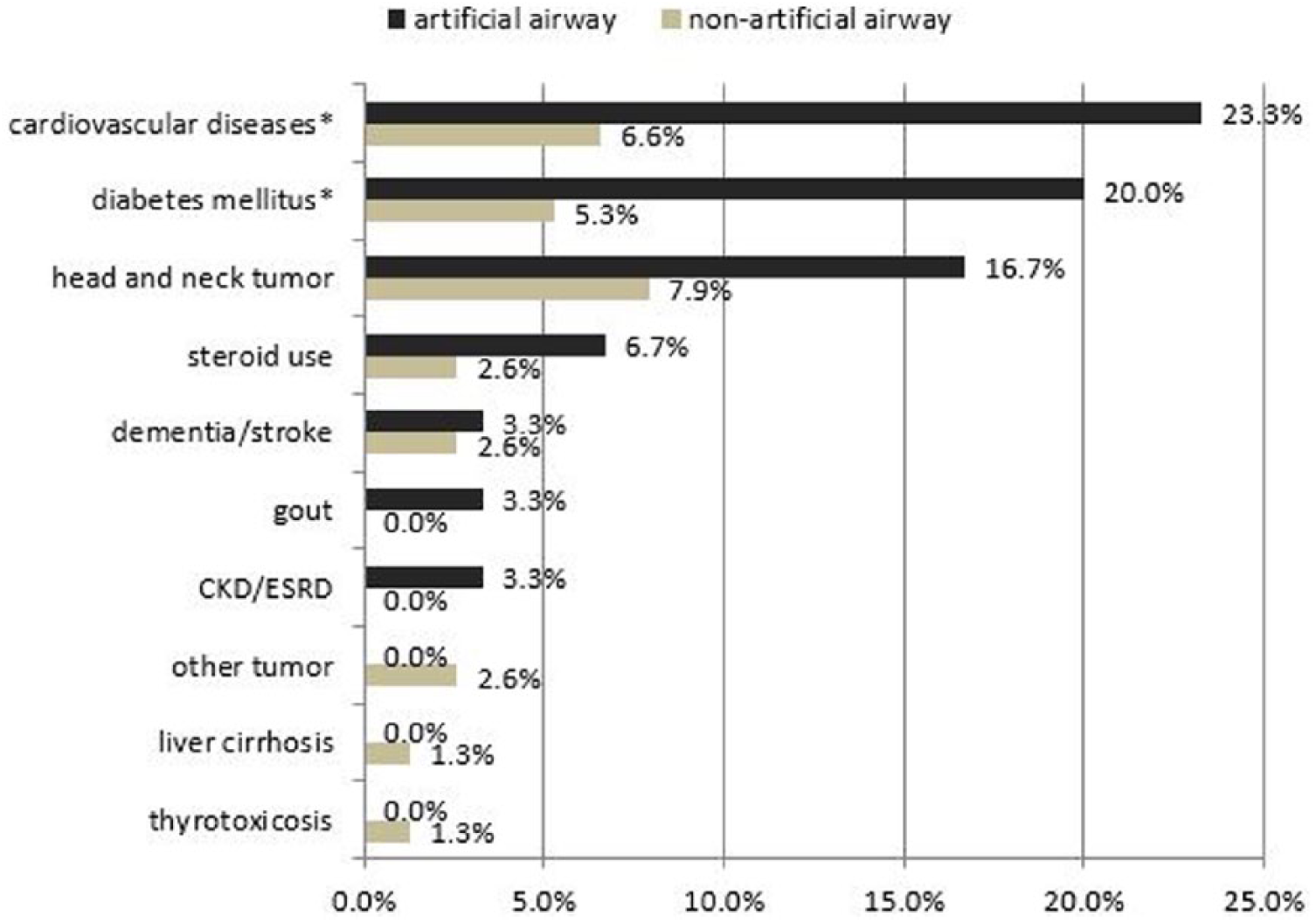
Comorbidity prevalence by artificial airway creation.
Comparisons between patients with AE who received an artificial airway and those who did not.
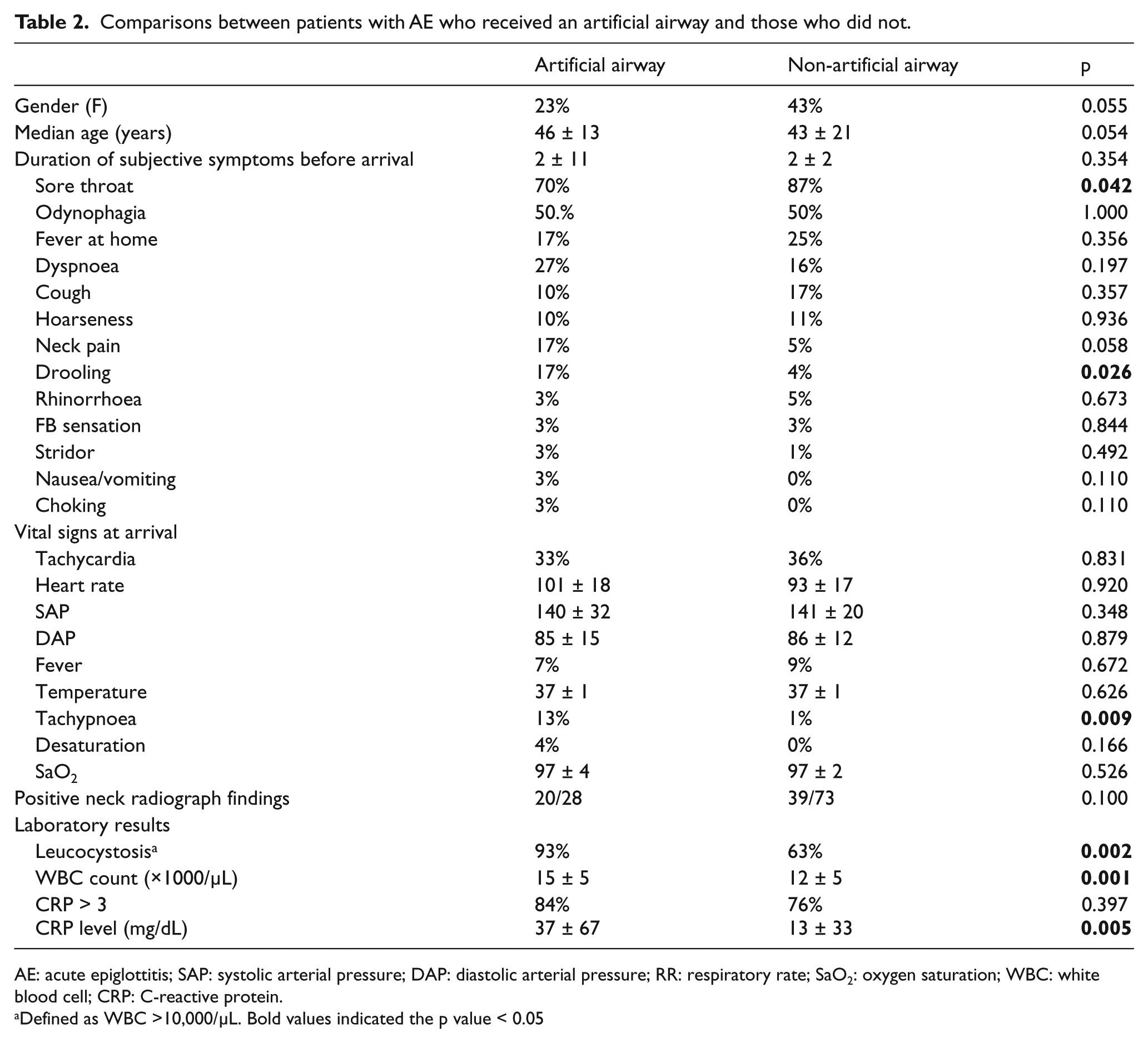
AE: acute epiglottitis; SAP: systolic arterial pressure; DAP: diastolic arterial pressure; RR: respiratory rate; SaO2: oxygen saturation; WBC: white blood cell; CRP: C-reactive protein.
Defined as WBC >10,000/μL. Bold values indicated the p value < 0.05
Discussion
The patient characteristics of our patients with AE were similar to those reported in other studies, that is, middle-aged and slightly predominantly male.4–7
Hypertension, diabetes mellitus, malignancy and asthma have been considered possible predisposing concomitant diagnoses for AE. 4 However, our study revealed that although cardiovascular diseases, diabetes mellitus and head and neck tumours were the three commonest comorbidities in patients with AE, only head and neck tumours were significantly more prevalent in the AE group than in the patients without AE, probably because the patients with head and neck tumours had typically undergone surgery or radiotherapy for their tumours, rendering the involved regions vulnerable and susceptible to infection or inflammation. In addition, cardiovascular diseases, diabetes mellitus, asthma or chronic obstructive pulmonary disease, and dementia or old stroke were even more common in patients with conditions mimicking AE.
A history of dementia and stroke impaired patients’ ability to express their symptoms and resulted in more patients being inaccurately diagnosed with AE. Patients with cardiovascular diseases, asthma or chronic obstructive pulmonary disease typically presented to the ED with dyspnoea, cough or tachypnoea. When combined with sore throat or odynophagia, these clinical presentations may indicate AE.
Several studies have revealed that sore throat was the commonest presenting complaint.4,6–11 However, this complaint was nonspecific and commonly expressed by patients with other disease entities. By contrast, odynophagia was more specific to patients with AE and was less often reported in the non-AE group. Rhinorrhoea and cough were typically caused by inflammation involving the extra laryngopharyngeal region and therefore usually resulted from conditions other than AE.
Previous studies have reported a sensitivity of 38%–77% and a specificity of 76% for diagnosing epiglottitis through radiography of the lateral soft tissues of the neck.7,10 Although lateral neck radiography is not a sensitive diagnostic tool, clinical physicians should clinically suspect AE when radiologic features indicative of a swollen epiglottis are present.
We determined that more patients with AE exhibited leucocytosis with a higher WBC count compared with patients without AE. However, neither elevated CRP prevalence nor the CRP level differed between the two groups. Therefore, WBC count may serve as a more effective screening parameter for diagnosing epiglottitis than CRP.
Airway management is essential in managing epiglottitis. No consensus has emerged on the optimal timing for establishing an artificial airway, whereas clinicians agree that patients presenting with an acute airway obstruction should undergo immediate airway management. Although concomitant underlying diseases interfered with AE diagnosis, their presence may decrease the immunity and physiologic reserve of patients with AE, thereby increasing the risk of airway obstruction. Our study found that patients with AE who required airway management had a higher prevalence of cardiovascular disease and diabetes mellitus, drooling, tachypnoea and leucocytosis. In addition, they had higher WBC counts and CRP levels, which served as surrogate markers of their greater disease severity. All patients with AE received similar medical treatment, but more patients with emergent airway management developed subsequent complications and had longer hospital stays.
Conclusion
We found that of the patients presenting with AE, those with definite AE were associated with head and neck tumours, odynophagia, positive neck radiography findings, leucocytosis and a high WBC count, but the aforementioned parameters were insufficient for formulating a clinical diagnostic tool. Therefore, for patients suspected of having AE, early referral for flexible laryngoscopy remains necessary. Furthermore, once a patient is confirmed as having AE, coexisting diabetes mellitus, cardiovascular diseases, drooling, tachypnoea, leucocytosis, a high WBC count and a high CRP level may indicate a higher risk of developing airway compromise.
Footnotes
Acknowledgements
I.-Y.W. contributed to the concept or design of the work and drafted the article. P.-C.L. acquired and interpreted data. C.-C.H. analysed the data and drafted the article. K.-T.C. contributed to the concept or design of the work and revised and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Availability of data and materials
Materials described in the manuscript, including all relevant raw data, will be freely available to any scientist wishing to use them for non-commercial purposes, without breaching participant confidentiality.
Informed consent
Waive of informed consent was approved by the Institutional Review Board of Chi-Mei Medical Centre.
Ethical approval
This study was reviewed and approved by the Institutional Review Board of Chi-Mei Medical Centre.
Human rights
This study was conducted according to the World Medical Association Declaration of Helsinki.