
Abstract
Background:
Heat illness in elderly patients has frequently occurred. Because of the difficulties in diagnosis and treatment, it is necessary for us to understand the clinical characteristics of elderly patients with heat illness.
Objective:
This study presents the demographic, clinical, and laboratory data for elderly patients who presented to our emergency department with heat illness and compares elderly group and non-elderly group to find out characteristics of elderly patient.
Methods:
We retrospectively analyzed the data of the elderly heat illness patients who had been presented to the emergency department of Jinshan Hospital, Fudan University, between 1 July 2014 and 1 October 2016.
Results:
There were 64 patients in the study in total and 25 elderly patients (39.1%). The mean age of the elderly patients was 72.8 ± 6.7 years; 18 cases (72%) were male and 7 cases (28%) were female. There were 5 mild cases (20%) and 20 severe cases (80%) in the elderly, which included 1 with heat cramps (5%), 4 with heat exhaustion (20%), and 15 with heat stroke (75%). Lactate dehydrogenase and creatine kinase were significantly higher in the elderly than in the non-elderly (p < 0.0001; t-value = −3.915 and −5.134, respectively). The Acute Physiologic Assessment and Chronic Health Evaluation II score and Modified Early Warning System score were significantly higher in the elderly than in the non-elderly (p < 0.0001; t-value = −6.411 and −4.705, respectively). Age was positively correlated with the Acute Physiologic Assessment and Chronic Health Evaluation II score and Modified Early Warning System score (r2 = 0.4939 and 0.3317, respectively; p value all <0.0001). The Acute Physiologic Assessment and Chronic Health Evaluation II score was positively correlated with lactate dehydrogenase and creatine kinase (r2 = 0.4103 and 0.4520, respectively; p value all <0.0001). The Modified Early Warning System score was positively correlated with lactate dehydrogenase and creatine kinase (r2 = 0.4759 and 0.5850, respectively; p value all <0.0001). There were 19 patients (76%) who improved and 6 patients (24%) who died in the elderly group.
Conclusion:
Chronic diseases and complications have increased rates in the elderly, who are also more likely to acquire severe heat illness, especially heat stroke. Lactate dehydrogenase and creatine kinase are positively correlated with Acute Physiologic Assessment and Chronic Health Evaluation II scores and Modified Early Warning System scores, which indicates that lactate dehydrogenase and creatine kinase could be good predictors of the severity of heat illness.
Introduction
Heat illness is a frequently occurring disease in the summer.1,2 Shanghai has always been very hot during the summer, with both high humidity and temperatures. Non-exertional heat illness has frequently occurred. Elderly patients make up the majority of non-exertional heat illness cases.3,4 It is difficult to diagnose and treat heat-related illness in elderly patient owing to slow metabolism, poor internal organ functioning, slow reaction time, and slow movement.5 –7 All of these increase complications in the disease. Shanghai has been an aging society since 1979. The elderly population in Shanghai will exceed 5.7 million by 2020. In this society, disease prevention and treatment for elderly patients are extremely important. Many people enter this older age category every day. The objective of this article is to retrospectively analyze the 25 elderly heat illness patients in the emergency room of Jinshan Hospital from 2014 to 2016. We hope to understand the clinical characteristics of elderly patients with heat illness in order to guide future clinical prevention and treatment.
Methods
We retrospectively analyzed 64 heat illness patients who presented to the emergency department of Jinshan Hospital, Fudan University from 1 July 2014 to 1 October 2016. We analyzed the general presentation, laboratory results on admission, Acute Physiologic Assessment and Chronic Health Evaluation II (APACHE II) scores and Modified Early Warning System (MEWS) scores 24 h after admission, morbidities, complications, and prognoses of all heat illness patients. The laboratory results included routine blood panels (liver and kidney function, electrolytes, blood sugar, blood gas analysis, and coagulation function). All heat illness patients received comprehensive treatment, 8 including temperature reduction by Ice carpet machine, protection of viscera function, maintenance of electrolyte balance, prevention of circulatory failure, shock, and infection. SPSS 16.0 software was used for statistical analysis (SPSS, Chicago, IL, USA). Continuous data were presented as the mean ± standard deviation (SD), and t-tests were used to compare the differences between groups. Nonparametric U tests were used to compare the differences in skewness between groups. Count data were analyzed using frequency and constituent ratio, and Pearson chi-square and Fisher’s exact tests were used. The correlation between the two parameters was assessed with a linear correlation analysis. All p values of <0.05 were considered statistically significant.
Results
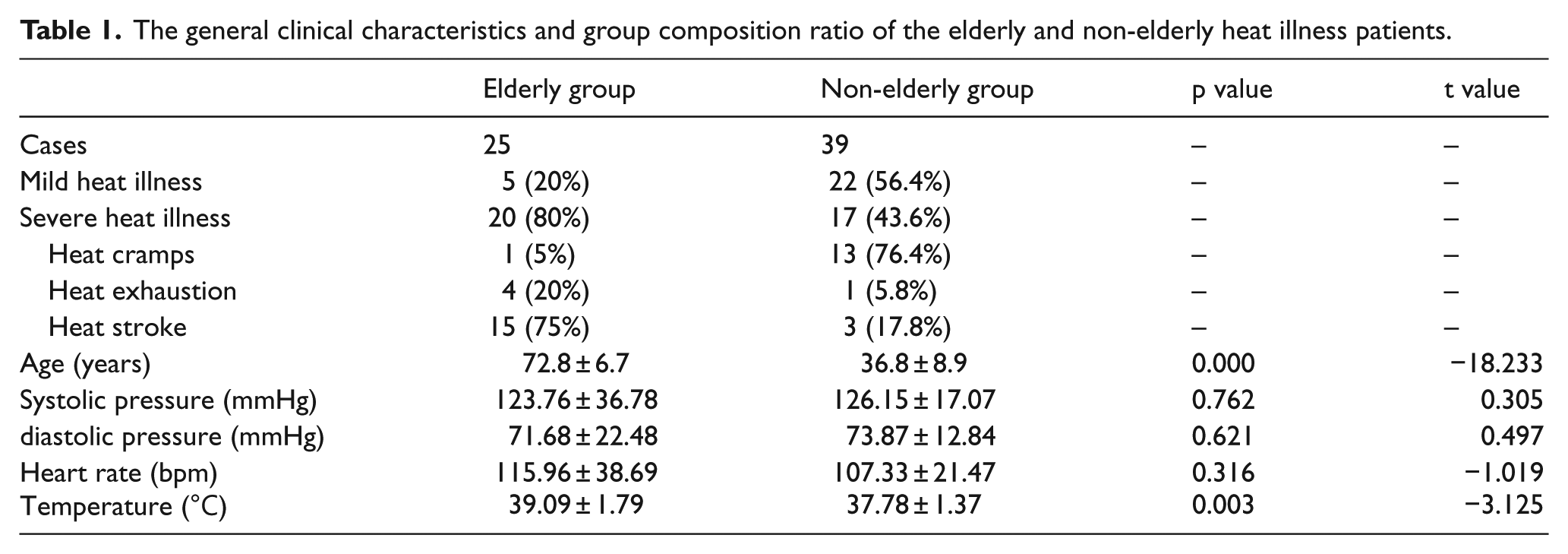
A total of 64 patients were enrolled in the study. Elderly patients (age ≥ 65 years) made up 25 of the cases (39.1%), with an age range from 65 to 92 years and mean age of 72.8 ± 6.7 years, 18 male cases (72%) and 7 female cases (28%). The non-elderly patients (age <65 years) made up 39 of the cases (60.9%), with an age range of 17–64 years and mean age of 36.8 ± 8.9 years, 30 male cases (76.9%) and 9 female cases (23.1%). There were 5 mild heat illness patients (20%) and 20 severe heat illness patients (80%) among the elderly patients. There was 1 heat cramp case (5%), 4 heat exhaustion cases (20%), and 15 heat stroke cases (75%) in the elderly severe heat illness patients. There were 22 mild heat illness patients (56.4%) and 17 severe heat illness patients (43.6%) in non-elderly patients. There were 13 heat cramps cases (76.4%), 1 heat exhaustion case (5.8%), and 3 heat stroke cases (17.8%) in the non-elderly severe heat illness patients. The heat stroke patients made up the majority of the elderly severe patients group. Meanwhile, the heat cramp patients made up the majority of the non-elderly severe patient group; 19 cases received support from the intensive care unit in elderly patients (4 heat exhaustion cases and 15 heat stroke cases), and 4 cases received support from the intensive care unit in non-elderly patients. There were no differences in systolic blood pressure, diastolic blood pressure, and heart rate between the elderly group and the non-elderly group. The temperatures reported in the elderly group were significantly higher than in the non-elderly group (p = 0.003, t = −3.125; Table 1).
The general clinical characteristics and group composition ratio of the elderly and non-elderly heat illness patients.
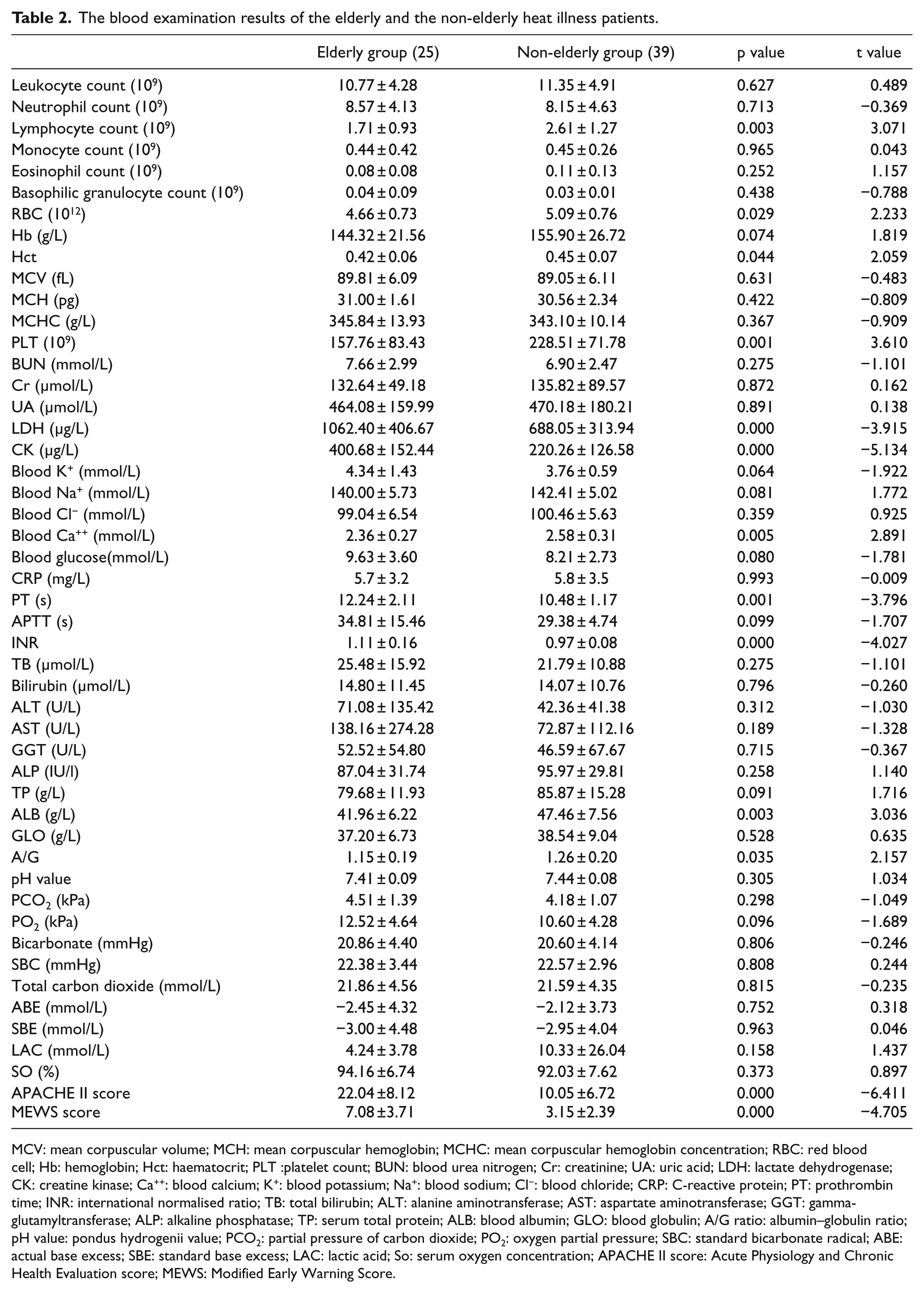
There were no differences in leukocyte count and neutrophil count between the elderly heat illness group and non-elderly heat illness group. The lymphocyte count, red blood cell (RBC) count, haematocrit, and platelet count in the elderly heat illness patients were lower than those in non-elderly heat illness patients (p values = 0.003, 0.029, 0.044, 0.001, respectively; t value = 3.071, 2.233, 2.059, 3.610, respectively). There were no differences in renal function of the two groups (including urea nitrogen, creatinine, and uric acid). Lactate dehydrogenase (LDH) and creatine kinase (CK) in elderly patients were significantly higher than those in non-elderly patients (p = 0.000 and 0.000, respectively; t value = −3.915 and −5.134, respectively). The blood calcium in the elderly group was lower than that in the non-elderly group (p = 0.005, t value = 2.891). Other electrolyte indicators (including blood potassium, blood sodium, and blood chloride) had no differences between the two groups. The prothrombin time (PT) and international normalized ratio (INR) in the elderly group were higher than those in the non-elderly group (p = 0.001 and 0.000, respectively; t = −3.796 and −4.027, respectively). There were no obvious differences in C-reactive protein (CRP) and liver function indicators (including total bilirubin, bilirubin, alanine aminotransferase, and aspartate aminotransferase). However, the blood albumin (ALB) and albumin–globulin ratio (A/G ratio) were lower in the elderly group than those in the non-elderly group (p = 0.003 and 0.035, respectively; t = 3.036 and 2.157, respectively). There were no obvious differences in blood gas analysis between the two groups. The APACHE II scores and MEWS scores were significantly higher in the elderly group than those in the non-elderly group (p = 0.000 and 0.000, respectively; t = −6.411 and −4.705, respectively; Table 2)
The blood examination results of the elderly and the non-elderly heat illness patients.
MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; MCHC: mean corpuscular hemoglobin concentration; RBC: red blood cell; Hb: hemoglobin; Hct: haematocrit; PLT :platelet count; BUN: blood urea nitrogen; Cr: creatinine; UA: uric acid; LDH: lactate dehydrogenase; CK: creatine kinase; Ca++: blood calcium; K+: blood potassium; Na+: blood sodium; Cl−: blood chloride; CRP: C-reactive protein; PT: prothrombin time; INR: international normalised ratio; TB: total bilirubin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyltransferase; ALP: alkaline phosphatase; TP: serum total protein; ALB: blood albumin; GLO: blood globulin; A/G ratio: albumin–globulin ratio; pH value: pondus hydrogenii value; PCO2: partial pressure of carbon dioxide; PO2: oxygen partial pressure; SBC: standard bicarbonate radical; ABE: actual base excess; SBE: standard base excess; LAC: lactic acid; So: serum oxygen concentration; APACHE II score: Acute Physiology and Chronic Health Evaluation score; MEWS: Modified Early Warning Score.
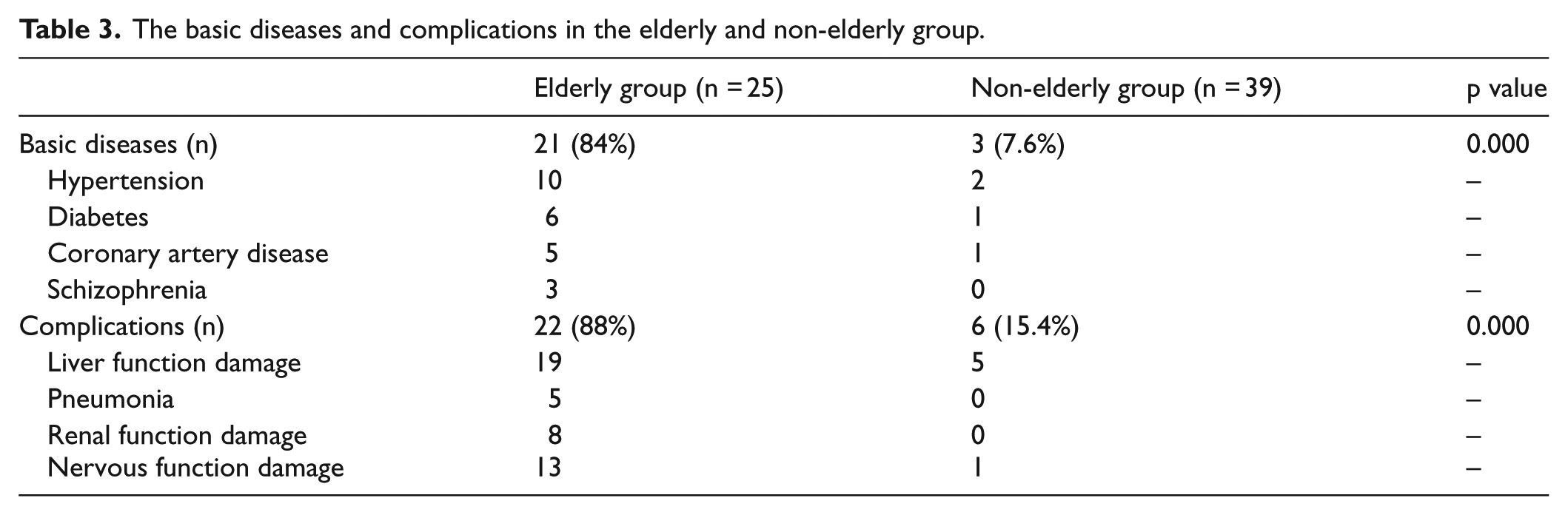
There were 21 patients with chronic diseases in the elderly group, including 10 cases of high blood pressure, 6 cases of diabetes, 5 cases of coronary artery disease, and 3 cases of schizophrenia (ruled out with neuroleptic malignant syndrome). There were 3 patients with chronic diseases in the non-elderly group, including 2 cases of high blood pressure, a case of diabetes, and a case of coronary artery disease. There were 22 patients with complications in the elderly group, including 19 cases of liver function damage, 5 cases of pneumonia (whose primary disease had been ruled out with pneumonia at admission), 8 cases of renal function damage, and 13 cases of nervous function damage. There were 6 patients with complications in the non-elderly group, including 5 cases of liver function damage and a case of nervous function damage (Table 3).
The basic diseases and complications in the elderly and non-elderly group.
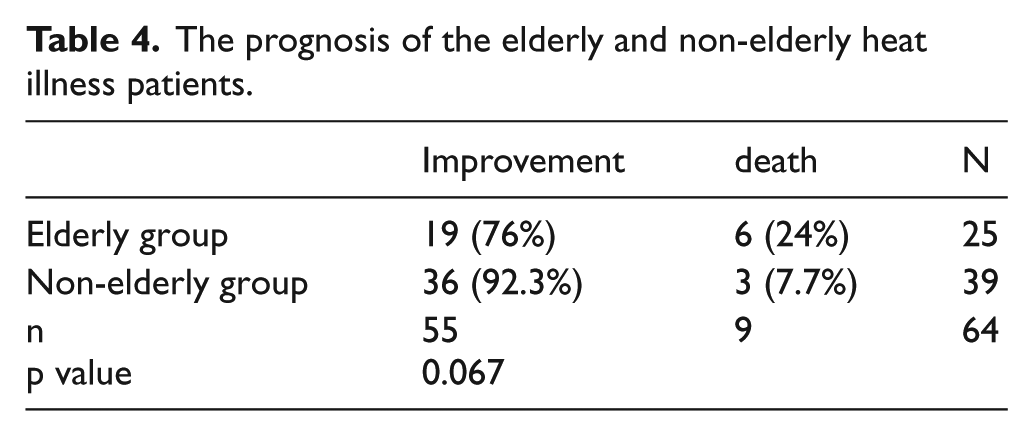
There were 19 patients who improved (76%) and 6 patients who died (24%) in the elderly group, while in the non-elderly group 36 patients improved (92.3%) and 3 patients died (7.7%). There were no significance differences between the two groups (p = 0.067; Table 4). The correlation coefficient between LDH and the prognosis is 0.445 (p value = 0.000), and the correlation coefficient between CK and the prognosis is 0.405 (p value = 0.001).
The prognosis of the elderly and non-elderly heat illness patients.
The APACHE II scores and MEWS scores in the elderly group were significantly higher than those in the non-elderly group (p = 0.000 and 0.000, respectively; t = −6.411 and −4.705, respectively). The LDH and CK in the elderly group were also significantly higher than those in the non-elderly group (p = 0.000 and 0.000, respectively; t = −3.915 and −5.134, respectively; Figure 1).
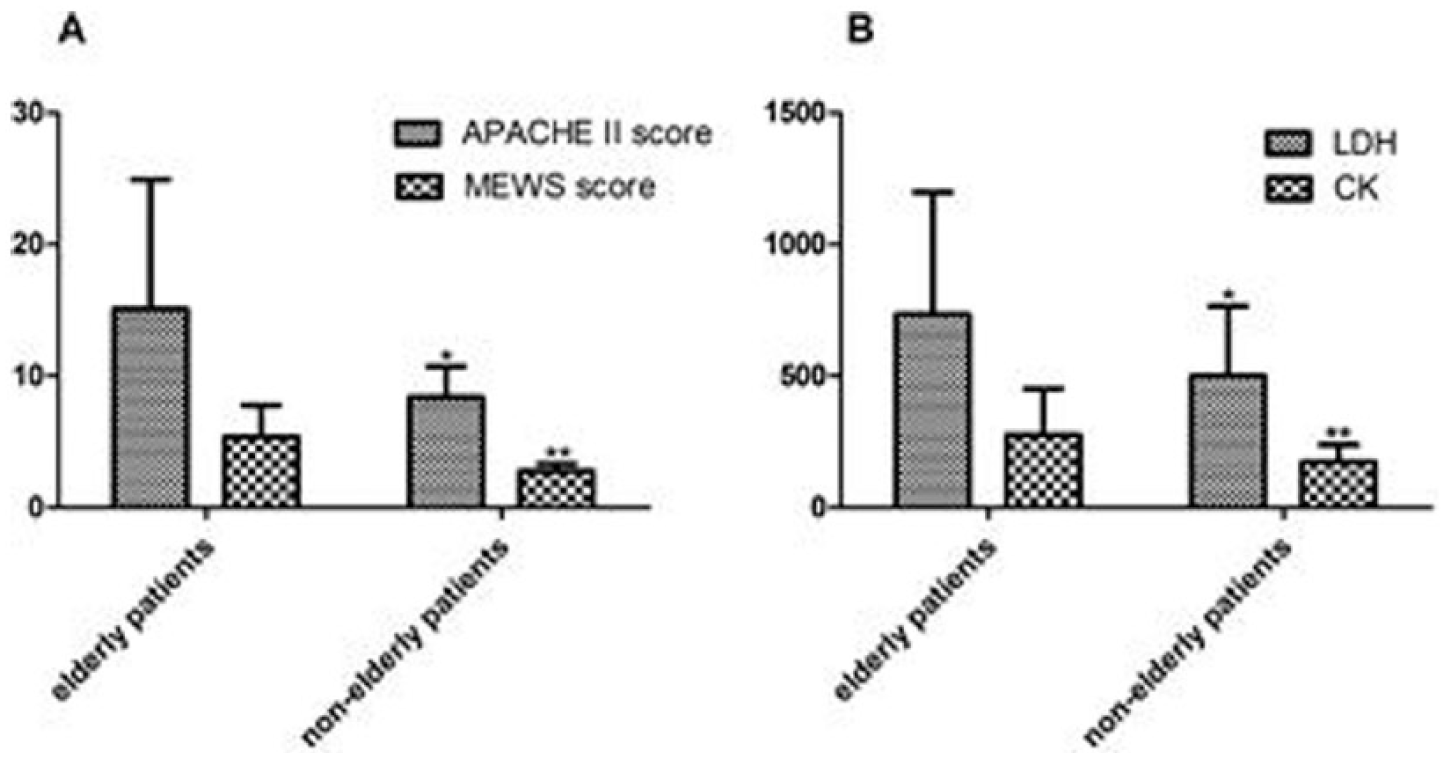
A: The APACHE II score and MEWS score in elderly patients and non-elderly patients. B: The LDH and CK in elderly patients and non-elderly patients
Age was positively correlated with APACHE II scores and MEWS scores (r2 = 0.4939 and 0.3317, respectively; p value all <0.0001). APACHE II score was positively correlated with LDH and CK (r2 = 0.4103 and 0.4520, respectively; p value all <0.0001). MEWS scores were positively correlated with LDH and CK (r2 = 0.4759 and 0.5850, respectively; p value all <0.0001). APACHE II scores were significantly positively correlated with MEWS scores (r2 = 0.6816; p value < 0.0001; Figure 2).
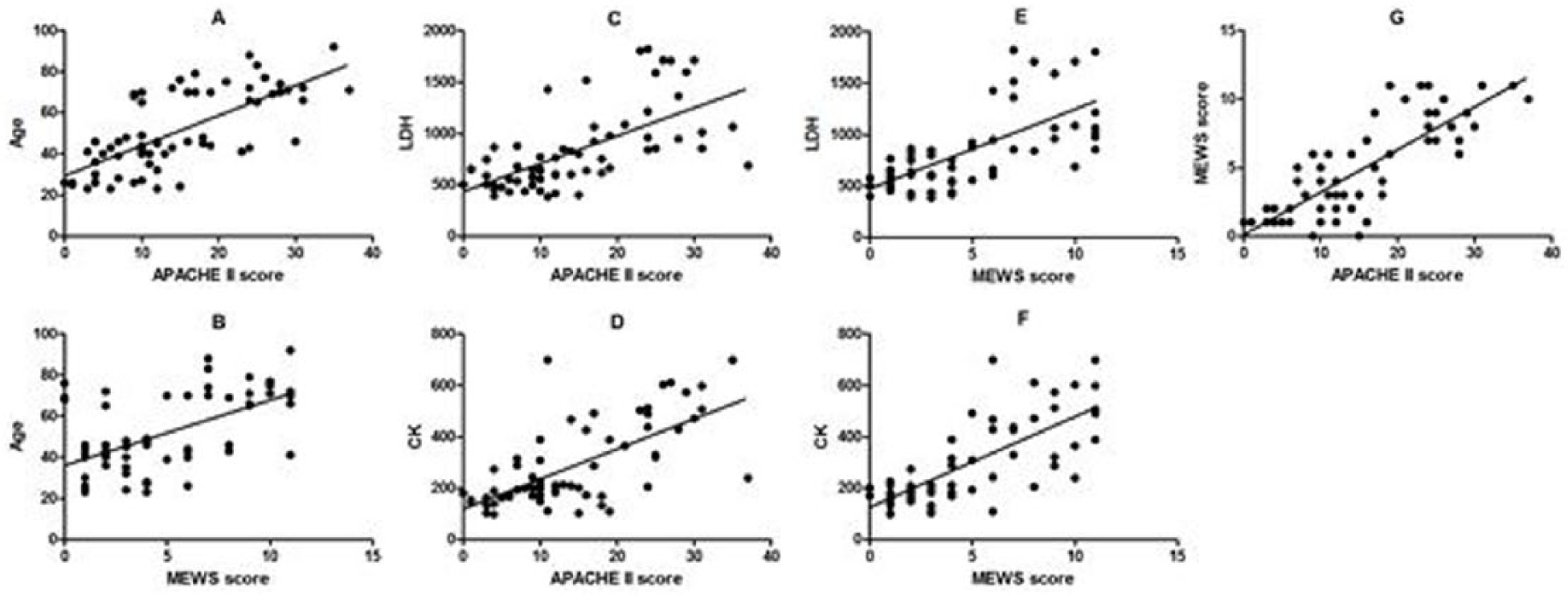
A and B: Age was positively correlated with APACHE II score and MEWS score. C and D: APACHE II score was positively correlated with LDH and CK. E and F: MEWS score were positively correlated with LDH and CK. G: APACHE II score was significantly positively correlated with MEWS score.
Discussion
The Jinshan district of Shanghai is located in the northern subtropical and monsoon climate zone and is influenced by alternating winter/summer wind and has four distinct seasons, abundant precipitation, more sun, and a long frost-free period. The summer begins in June and continues for approximately 3 months. This season has elevated temperatures and heat. Mid-July to mid-August is the hottest period in the year. 9
Heat illness is an acute disease that results in central nervous system and circulatory system dysfunction due to the discontinuation of human body temperature regulation in a high-temperature environment. Heat illness is divided into mild heat illness and severe heat illness, and severe heat illness includes heat cramp, heat exhaustion, and heat stroke. Heat cramp is exercise-associated painful involuntary muscle contractions during or immediately after exercise. 8 Heat exhaustion is caused by exposure to high environmental heat or strenuous physical exercise; signs and symptoms include intense thirst, weakness, discomfort, anxiety, dizziness, and syncope; core temperature may be normal or slightly elevated to >37°C (98.6°F) but <40°C (104°F). 8 Heat stroke is characterized by a core temperature >40°C (104°F) and central nervous system abnormalities such as altered mental status (encephalopathy), seizure, or coma resulting from passive exposure to environmental heat or strenuous exercise. 8 Heat cramps are a result of excessive sweating in the high-temperature environment, where loss of a lot of sodium chloride in the body leads to cramping in the muscles of limbs and abdominals. For heat exhaustion, the body temperature of a patient does not rise; heat exhaustion is the failure of blood circulation to continue in a high-temperature environment, which leads to hypotension, tachycardia and tachypnoea, a large amount of sweat, cool skin, decrease in plasma and intercellular fluid volume, dizziness, and eventually collapse of the patient. However, the patient’s temperature remains normal. 10 Heat stroke refers to the disorders of the body temperature adjustment function caused by a high temperature in the environment. The body temperature rises excessively and leads to damage of the central nervous system. 10 Heat stroke is the most serious heat illness. It is a fatal disease and has a high fatality rate. 11 In the early stage of this illness, the functions of many important organs such as the brain, liver, kidney, and heart have been influenced.12,13
As the economy of Shanghai has grown, it has also become an aging society. Organ function gradually reduces in the elderly, including thermoregulation ability and stress reaction ability. In addition, the elderly have a variety of chronic diseases, such as high blood pressure, diabetes, coronary heart disease, and schizophrenia. In an instance of heat illness, the elderly easily acquire many complications, which can lead to a poor outcome. Therefore, the elderly can easily develop severe heat illness.14,15 The occurrence of heat illness in the elderly is also related to living conditions. 16 The elderly group is less likely to tolerate the high temperature and use effective precautions to protect them. 17 Through the study we found that the elderly people easily develop severe heat illness, heat stroke in particular. Heat stroke occurs when there is an excess saving of heat in the body and the body temperature significantly increases. The circumstance where the majority of heat stroke patients are in the elderly group is likely closely related to the physiological condition of the elderly group. Because in the early stages of heat illness, elderly patients may only show altered mental state, a change of consciousness, a decline in activity, and the lack of typical symptoms; the patients may rapidly develop heat stroke if the initial heat illness is not caught early. Alternatively, severe heat illness patients in the non-elderly group easily develop heat cramps. This is associated with the patient’s age, physiological characteristics, and work environment or amount of motion. These patients have excessive sweating as a typical symptom. Furthermore, they can accurately express their discomfort, which can result in their heat illness being found in a timely manner.
Although some elderly patients have hypertension, some other elderly patients also have shock, namely, heat exhaustion. Furthermore, because of the acute stress reaction, blood pressure will rise correspondingly in the non-elderly group. Therefore, there are no differences in systolic blood pressure and diastolic blood pressure between the two groups. There were no differences in heart rate between the two groups. The temperature in the elderly group is obviously higher than that in the non-elderly group because heat stroke is the most common type of severe heat illness in the elderly group. The temperature in heat stroke patients increases significantly due to the excess heat retention and the challenges with temperature adjustment.
The lymphocyte count in the elderly group is lower than that in the non-elderly group. There were no differences in leukocyte count, neutrophil count, mononuclear cell count, eosinophil count, and basophilic granulocyte count between the two groups. Lymphocytopenia is mainly due to adrenal cortical hormone therapy, radiation damage, immune deficiency disease, and agammaglobulinemia. The lymphocyte count was lower in the elderly group, which may indicate that the elderly patients perhaps have immune deficiency and are more likely to develop various complications. This may need further research. The RBC count and erythrocyte pressure in the elderly group were lower than those in the non-elderly group. This is primarily because blood concentration in the non-elderly group is more obvious and the elderly patients have more basic diseases.
The number of blood platelets normally remains at a certain level. Platelets not only play important roles in blood clotting but also are very active cytokines. Platelets have many biological activities and participate in all types of stress reaction. The platelet count in the elderly group was lower than that in the non-elderly group. The elderly group had more severe patients. Once the platelets are activated, the shape of the platelets changes, and they adhere to the vascular endothelial cells and other cells; they further attract neutrophils and lymphocytes in the blood vessels to finally form the microthrombosis. Meanwhile, the breakdown products after platelet activation such as the platelet activation factor and the inflammation factor further aggravate systemic inflammatory response and affect the prognosis of patients.
There was no obvious difference in kidney function, blood glucose, and CRP between the two groups. There was no obvious difference in liver function in terms of ALT and ALP, but there was difference in PT and ALB between the two groups. The damage to the liver is obvious. The damage likely occurs in the early stage or the late stage of the heat illness. PT and international standardization ratio (INR) in the elderly group are higher than those in the non-elderly group. PT not only can reflect liver synthesis function and liver reserve function but can also reflect the disease severity and the prognosis of the disease. Serum ALB is also synthesized by the liver and can also reflect the liver function. The rise of PT and the reduction of ALB in heat illness patients reflect the abnormality of liver function, especially in the elderly group. The blood calcium (Ca++) in the elderly group is lower than that in the non-elderly group. The reduction of blood calcium is likely associated with hypocalcemia in elderly patients. There was no difference in blood potassium (K+), blood sodium (Na+), and blood chloride (Cl−) between the two groups. 18
The rise of LDH and CK in the elderly group is helpful in the estimation of the severity of heat illness. LDH and CK in the elderly group are significantly higher than those in the non-elderly group and are positively correlated with APACHE II scores and MEWS scores. APACHE II scores are positively correlated with LDH and CK (r2 = 0.4103 and 0.4520, respectively; p values all <0.0001). MEWS scores are positively correlated with LDH and CK (r2 = 0.4759 and 0.5850, respectively; p values all <0.0001). APACHE II scores are composed of the acute physiology score (APS), age, and chronic health evaluation. The acute physiology score (APS) includes rectal temperature, mean arterial pressure, heart rate, breath rate, oxygen cooperation, arterial blood PH value, blood potassium (K+), blood sodium (Na+), haematocrit (Hct), creatinine (Cr), leukocyte count, and Glasgow coma score. The MEWS score is an early forewarning score and can dynamically monitor the progression of disease and detect potential dangers in the early stage. We found that APACHE II scores were positively correlated with MEWS scores (r2 = 0.6816; p value <0.0001). APACHE II scores and MEWS scores are closely related to the disease. A higher score indicates greater severity of disease and a greater risk of death.19,20 As the age of heat illness patients rises, the APACHE II score and MEWS score increase. Age is also positively correlated with APACHE II score and MEWS score (r2 = 0.4939 and 0.3317, respectively; p values all <0.0001). This indicates that the greater the age of heat illness patients, the greater severity of the disease. APACHE II scores and MEWS scores have excellent prediction for the severity of the disease. 21 LDH and CK have good positive correlation with APACHE II scores and MEWS scores. This indicates that LDH and CK could be an excellent prediction effect for the severity of heat illness. The correlation coefficient between LDH and the prognosis is 0.445 (p value = 0.000), the correlation coefficient between CK and the prognosis is 0.405 (p value = 0.001). LDH and CK are positively correlated with the prognosis. But they appear to medium correlation. This is mainly because LDH and CK were taken at admission, and the patients with heat illness were taken in for comprehensive treatment and we reduced the mortality for severe heat illness.
The LDH and CK in the elderly group are significantly higher than those in the non-elderly group. CK is the key enzyme of cellular energy metabolism and usually exists in the heart, muscle, and brain tissues. LDH is a glycolytic enzyme and exists in the cytoplasm of all tissues and cells of the body. LDH and CK increase significantly in the elderly group. This is related to muscle damage and rhabdomyolysis.11,21,22 After rhabdomyolysis, tumor necrosis factor (TNF)-α increases in the serum, inducts the skeletal muscle to dissolve, and promotes peroxide to release. 23 With the role of cytokines and endotoxins, temperature regulation and abnormal blood coagulation mechanisms are further aggravated, the function of endothelial has been damaged, and multiple organs develop dysfunction until the occurrence of sepsis and affect the prognosis of heat illness patients. 24
There are more basic diseases and complications in the elderly group, such as in patients with schizophrenia where the illness detection was delayed because of communication barriers after the occurrence of heat illness. The complications in the elderly group include the damage to liver and kidney function and the damage to the nervous system and pneumonia. However, there are no obvious differences in the mortality between two groups. When the patients arrive to the emergency department, they are treated urgently, including rapid temperature reduction, 25 oxygen inhalation, venous transfusion, correction of electrolyte disorders, prevention of infection, and protection of organ function. The patients with heat illness are taken in for comprehensive treatment in rapid time. Furthermore, we establish the immediate forecast system of the blood critical value and transport security system for severe patients. Through this comprehensive treatment, we reduce the mortality for severe heat illness especially in the elderly patients.
Conclusion
The basic diseases and complications are clearly elevated in elderly patients, who are more likely to develop severe heat illness, especially heat stroke. The lymphocyte, RBC, hematocrit (HCT), PLT, blood Ca++, and ALB in elderly patients are lower than those in non-elderly patients. The PT, INR, LDH, CK, APACHE II scores, and MEWS scores in elderly patients are higher than those in non-elderly patients. The age of the patients is positively correlated with APACHE II score and MEWS score. This indicates that the greater the age of heat illness patients, the more severity of the disease. LDH and CK are positively correlated with APACHE II scores and MEWS scores, which indicate that LDH and CK may have excellent prediction effects for the severity of heat illness. But this subject should need more sample size and in-depth study further.
Limitation
The number of patients recruited in this study is only 64 and elderly patients account for 25. So, there is the limitation of the small patient sample size. We need more sample size for further study.
Footnotes
Acknowledgements
The authors gratefully acknowledge the assistance of the medical and nursing staff of the Emergency Department of Jinshan Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
All of the data and materials are available and credible in this article.
Informed consent
Due to the retrospective nature of the study, informed consent was waived.
Ethical approval
The study was approved by the ethical committee of Jinshan Hospital.