
Abstract
Background:
After the main shock of a major earthquake, casualties cluster in a short period and may overwhelm the capacities of health care facilities. An earthquake with a magnitude of 6.4 on the Richter scale struck Tainan City causing 117 fatalities and 513 injuries.
Objectives:
We conducted a retrospective study to review the medical records of emergency department after the attack of earthquake. The aim of this study was delineating the medical resource requirements after the disaster.
Methods:
We reviewed the medical records of patients admitted to the emergency department of Chi Mei Medical Center. Each chart indicating that the emergency department visit was earthquake-related was reviewed. After the earthquake struck, the Chi Mei Medical Center mobilized off-duty staff through a preset 333 code. Subsequently, routine surgeries and nonurgent admissions were postponed to reserve the maximal capacity for wounded patients.
Results:
A total of 150 patients were reviewed during the study period. In all, 25 cases (23.8%) required admission, and 9 of them (8.6%) were admitted to the intensive care unit. Patients with earthquake-related injuries constituted 62.8% of all traumatic patients in the 24-h aftermath. The requirements for wound sutures, blood component transfusion, numbers of radiographic/computed tomographic scans, and invasive procedures increased dramatically (earthquake-related/total: 66.0%, 30.0%, 72.1%/57.4%, and 47.7%, respectively).
Conclusion:
Patients with earthquake-related injuries arrived at the emergency department soon after the earthquake occurred and substantial emergency department resources were utilized in the 24-h aftermath. Each hospital should have a preset mobilization signal to call in off-duty workers to treat casualties resulting from the main shock of an earthquake. Subsequently, hospital-based mobilization should be initiated to provide comprehensive care to severely injured patients.
Introduction
Earthquakes are the most harmful type of natural disaster and cause considerable life and material loss. 1 In addition, casualties resulting from an earthquake usually cluster in a short period after the main shock and overwhelm the capacities of health care facilities. A survey conducted after the Chi-Chi Earthquake in Taiwan demonstrated that there was a considerable increase in medical demand for as long as 3 days. 2 A hospital in Turkey reported that approximately two-thirds of patients with earthquake-related injuries present within the first 48 h. 3 After the 2005 Kashmir earthquake, a small military hospital recorded that 1502 patients were triaged over the first 72 h. 4 These findings demonstrate that emergency departments (EDs) should be appropriately prepared for the initial patient surge after an earthquake.
At 3:57 a.m. local time on 6 February 2016, an earthquake with a magnitude of 6.4 on the Richter scale occurred in Southern Taiwan, 5 causing 117 fatalities and 513 injuries in Tainan City. 6 The highest number of deaths from a single incident (115) occurred in a collapsed 17-story residential building, with another 397 people rescued from the building (Figure 1). At the time of this event, Chi Mei Medical Center was located near the collapsed building; thus, the ED was inundated with wounded patients in the aftermath of this event. The ED mobilized additional human and medical resources from the other departments of Chi Mei Medical Center, and all patients received timely and suitable medical care. Meanwhile, the ED continued to provide regular medical care to other patients with ED visits unrelated to the earthquake until the end of this event.

The collapsed 17-story residential building.
In this study, we conducted a retrospective study to review the medical records of ED after the attack of earthquake. The aim of this study was delineating the profile of patients with earthquake-related injuries and the various medical resource requirements. If the basic infrastructure remains intact after an earthquake, these medical resources are imperative for EDs to manage the initial surge in patient inflow after the main shock of an earthquake.
Methods
Chi Mei Medical Center mainly provides medical care for Tainan City with a total population around 1,850,000. In Chi Mei Medical Center, the annual ED visits and emergent surgeries for trauma patients are about 120,000 and 2700. This study was reviewed and approved by the Institutional Review Board of Chi Mei Medical Center. We reviewed the medical records of patients admitted to the ED of Chi Mei Medical Center from 6 to 13 February 2016 (the end date of all rescue efforts on the collapsed building). Except those who presented to the ED themselves, the communication and dispatch of patients were conducted by Tainan City Government Fire Bureau. There were 13 hospitals in Tainan City available to receive the victims of earthquake. Generally, severely wounded patients are more likely to be transported to Chi Mei Medical Center because of its high capacity in handling severe trauma patients. Each chart indicating that the ED visit was earthquake related was reviewed. The same patient with multiple ED visits was considered a single case to avoid overpresentation of certain cases. For each patient, we collected data on demographic characteristics; diagnosis; numbers of roentgenographic examinations and computed tomographic scans on each body part; requirements for wound sutures, splinting/casting, and invasive procedures; hospital courses; and requirements for emergent surgery and intensive care.
After the earthquake struck, Chi Mei Medical Center issued a preset 333 code to mobilize health care personnel to the ED. The 333 code activated in-hospital staff to the ED and notified executives of related departments. In the night shift, 5 doctors, 20 nurses, and 2 nursing assistants were on duty. After the 333 code was issued, 9 doctors, 25 nurses, and 3 nursing assistants arrived before the commencement of the day shift. In the morning, all medical departments were notified to evacuate wards and intensive care units as much as possible. In addition, surgeons deferred their routine surgeries, and nonurgent admissions, such as those for scheduled examinations, were postponed.
A total of 105 patients with earthquake-related injuries were recorded during the study period, and 88.6% of them presented to the ED within 24 h after the earthquake. The definitions of earthquake-related injuries were based on two criteria: (1) the patients described that they were hurt during the attack of earthquake and their purposes of ED visits were for the care of traumatic injuries and (2) for nontraumatic cases, the ED visits were related to the consequences of earthquake. These statistics show that patient management after the main shock of an earthquake is crucial to EDs. Therefore, we also reviewed the data of each ED patient who was admitted to the ED within 24 h after the earthquake. The increased medical burden may represent the additional medical resource requirements in the aftermath of such events.
Results
General descriptions
We reviewed the medical records of 105 patients (54 female and 51 male patients), with a mean age of 39.1 ± 19.8 years. These patients included 9 (8.6%) geriatric patients (>65 years old) and 11 (10.5%) pediatric patients (<15 years old). Most patients (101) visited the ED because of traumatic events; only 4 patients were nontraumatic cases. Among the nontraumatic cases, two required oxygen supply and regular airway suction for home-based respiratory care, and they were admitted to the ED because of the discontinuation of electricity resulting from the earthquake. One 5-year-old child was entrapped in the collapsed building for more than 24 h and was admitted because of dehydration. One 87-year-old woman underwent surgical treatment for a femoral fracture resulting from the earthquake in another hospital. However, she became comatose and respirator-dependent after the operation and had to be subsequently transferred to our hospital for intensive care. No patient was transferred from Chi Mei Medical Center to other hospitals. Among the traumatic patients, two arrived at the ED in an out-of-hospital cardiac arrest state and were declared dead without resuscitation. 7 The most common injury sites were the extremities (54), head (44), and torso (25). In all, 25 cases (23.8%) required admission, and 9 of them (8.6%) were initially admitted to the intensive care unit. Regarding the required procedures, 36 patients (34.3%) required wound suturing, and 4 patients required splint/casting for bone fractures. In addition, six central venous catheters, four tracheal tubes, and one chest tube were inserted for shock, respiratory failure, and hemothorax, respectively. About 74 patients sustained minor injuries which required only examinations and cares in ED for their injuries The reasons for the hospitalization of traumatic patients were bone fractures in 15 patients, crush syndrome (defined as creatine kinase >1000 U/L) 8 in 8 patients, hemothorax/lung contusions in 5 patients, subarachnoid hemorrhage in 3 patients, spinal injuries in 2 patients, and spleen contusion in 1 patient (Table 1). Because the load of patients did not exceed the capacity of Chi Mei Medical Center, we did not modify the standard of care according to the suggestions of American College of Emergency Physicians. 9 We did not find any cases who were admitted to Chi Mei Medical Center within 1-week period after the earthquake for wound infection.
Profile of patients with earthquake-related injuries.
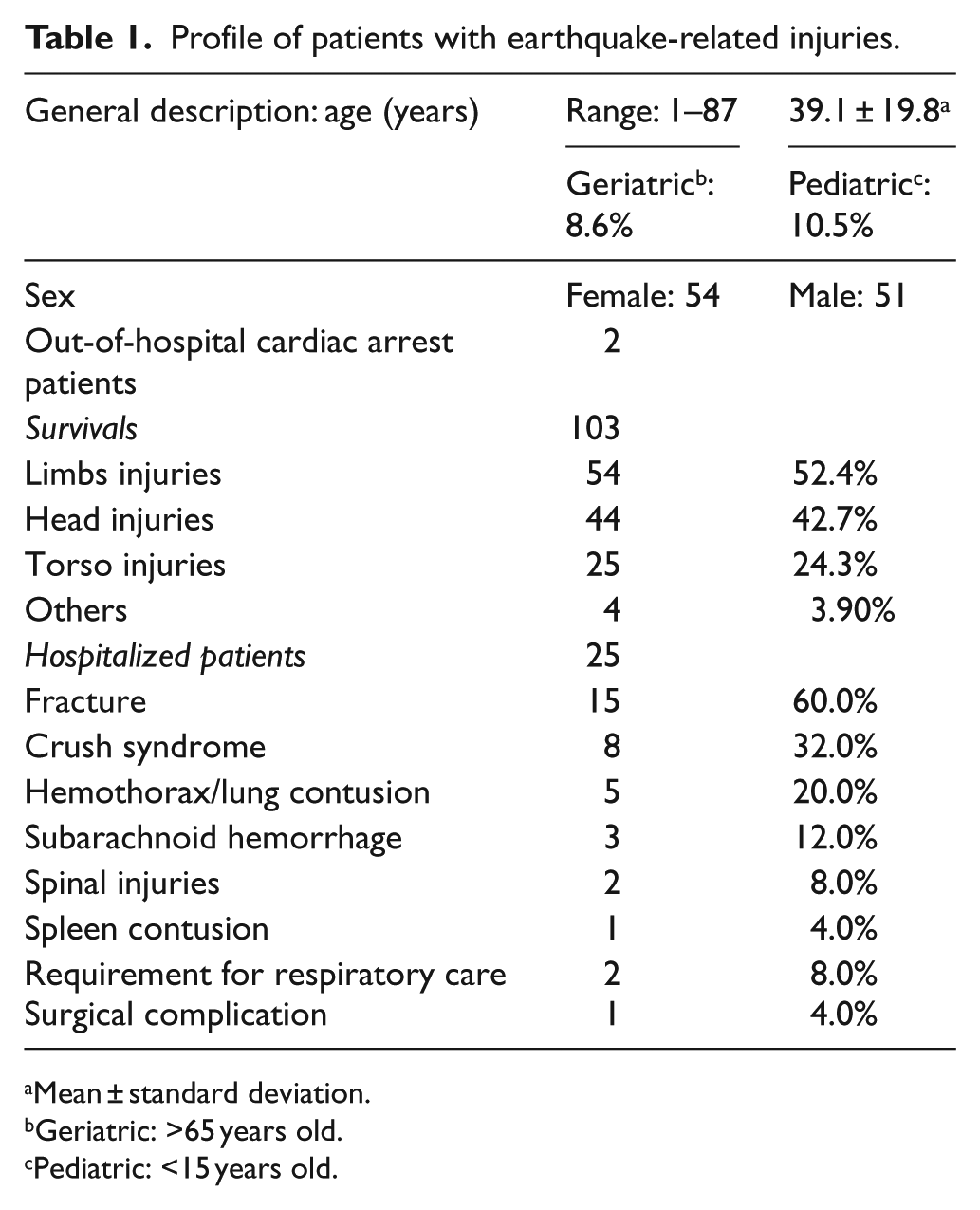
Mean ± standard deviation.
Geriatric: >65 years old.
Pediatric: <15 years old.
Additional medical burden in 24-h aftermath
Immediately after the earthquake struck, wounded patients began arriving at the ED, and patients with earthquake-related injuries exceeded 30% of ED visits per hour in the first 9 h (Figure 2). Patients with earthquake-related injuries constituted 62.8% (91/145) of all traumatic patients and 24.8% (93/375) of all patients in the 24-h aftermath. In the ED, the requirements for wound sutures, blood component transfusion, numbers of radiographic/computed tomographic scans, and various procedures increased dramatically (earthquake-related/total: 66.0%, 30.0%, 72.1%/57.4%, and 47.7%, respectively). In addition, one-fourth of hospitalizations (25.6%) and nearly half of intensive care unit admissions (46.2%), emergent surgeries (50.0%), and mortalities (50.0%) resulted from earthquake-related injuries (Table 2). We did not provide extra psychological care to the victims of this earthquake.
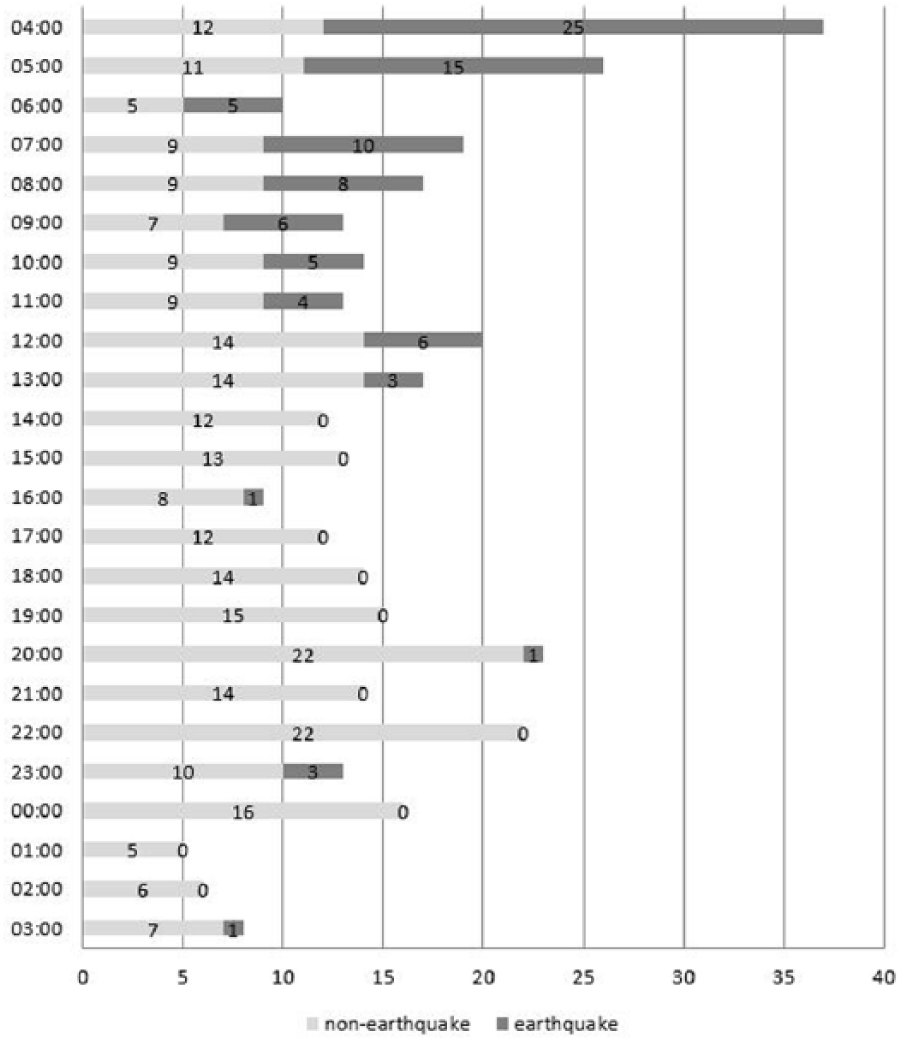
A graph of the number of patients presenting to the emergency department with earthquake-related injuries or non-earthquake-related injuries by hour—from 4:00 a.m. on 6 February to 3:00 a.m. on 7 February.
Additional medical burden within 24 h following the earthquake.
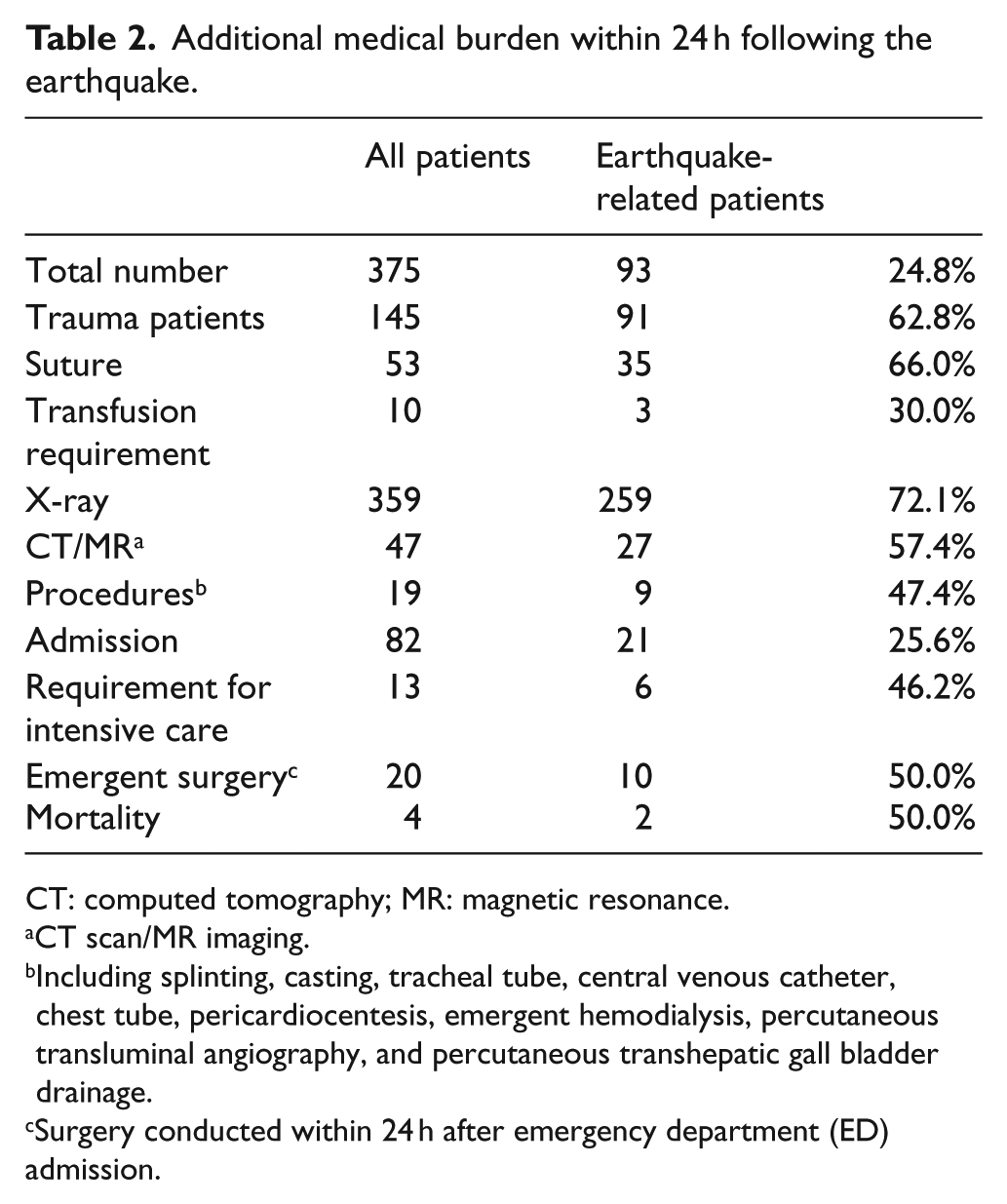
CT: computed tomography; MR: magnetic resonance.
CT scan/MR imaging.
Including splinting, casting, tracheal tube, central venous catheter, chest tube, pericardiocentesis, emergent hemodialysis, percutaneous transluminal angiography, and percutaneous transhepatic gall bladder drainage.
Surgery conducted within 24 h after emergency department (ED) admission.
Discussion
The region severely damaged by the earthquake was located in a metropolitan area; therefore, rescue efforts were initiated soon after the earthquake struck. The first patient with earthquake-related injuries presented to the ED within 20 min, and 80% of patients arrived at the ED in the first 9 h after the earthquake. The most stressful situation occurred early on in the ED; thus, health care facilities should maintain a practical alarm system for managing natural disasters. In our hospital, the 333 code alerted a considerable number of health care workers, even at midnight. Fortunately, the infrastructure of Tainan City remained intact despite after the attack of earthquake; there is no difficulty in recruiting off-duty staff. This emergent mobilization enabled the successful management of the overwhelming number of patients with earthquake-related injuries and facilitated smooth regular ED operation. Both World Health Organization and American College of Emergency Physicians had published their guidelines about how to prepare for disasters; we believed that all hospitals should have a preset plan to cope with the challenge of disasters.10,11
Initially, most patients who arrived at the ED had sustained minor injuries and required simple wound care and examinations for fractures or internal organ injuries. At this stage following a disaster, EDs do not require specially trained personnel such as technicians, physicians, and surgeons who can operate exquisite instruments for extraordinary invasive procedures. Nurses and doctors who are familiar with wound care and have been trained regarding the general concepts for trauma can adequately manage the initial patient surge. Subsequently, more systemic measures, including the evacuation of the ward and intensive care unit and withholding nonurgent medical service, provide greater flexibility for the management of subsequent patients with earthquake-related injuries.
From this experience, we discovered urgent requirements for radiographic and computed tomographic scans. Rapid investigations accelerated the management of wounded patients and effectively relieved the substantial inflow of patients in the ED. Hospitals should therefore consider mobilizing radiologists after an earthquake and providing more equipment for radiographic and computed tomographic scans.
Similar to other studies on casualties after an earthquake, we found that the extremities were the most common injury site,3,4,12 followed by the head and torso. Fractures and crush injuries in the extremities contributed considerably to the emergent surgery and admission requirements. ED admissions for other severe torso and head trauma were distributed across different time points. Therefore, emergent consultations with specialists and surgeons were easily performed, and the management of patients was smooth.
Among patients with earthquake-related injuries, wound infection and acute kidney injury are two critical complications.3,4,8,12 In our series, the rate of wound infection was lower than that reported in other studies, and none of the patients developed acute kidney injury. Because the scale of earthquake-related casualties did not overwhelm the capacity of health care facilities, the basic infrastructure remained intact, and the early effective mobilization of off-duty staff in the ED ensured that patients with earthquake-related injuries received timely and adequate treatment. We believe that these are crucial factors for ensuring excellent patient outcomes.
Our study is limited by the following factor. Every disaster is unique and causes different damage. The experience of the ED in this medical center may not be extrapolated in other hospital. However, for the emergency physicians and trauma surgeons, this disaster still provides a valuable experience about how to manage the disaster. In addition, the recruited staff arrived at different times and we did not record the contributions of these staff, which made it difficult to estimate their roles and responsibilities.
Conclusion
Patients with earthquake-related injuries arrived at the ED soon after the earthquake occurred, and substantial ED resources were utilized in the 24-h aftermath. The requirements for wound sutures, blood component transfusion, numbers of radiographic/computed tomographic scans, various invasive procedures, emergent surgeries, and admission to ward and intensive care unit increased dramatically. All hospitals should have a preset mobilization signal to call in off-duty health care workers, including nurses, doctors, and radiologists, to treat casualties resulting from the main shock of an earthquake. Subsequently, hospital-based mobilization should be initiated to provide comprehensive care to severely injured patients.
Footnotes
Acknowledgements
The authors are grateful to Central News Agency for providing the photograph used in the manuscript. C.Y. contributed to the concept or design of the work and drafted the article; A-C.P. contributed to acquisition and interpretation of data; C-C.H. contributed to analysis of data and drafted the article; and K-T.C. contributed to the concept or design of the work, revised, and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The materials described in the manuscript, including all relevant raw data, will be freely available to any scientist wishing to use them for non-commercial purposes, without breaching participant confidentiality.
Informed consent
Waive of informed consent was approved by the Institutional Review Board of Chi Mei Medical Center.
Ethical approval
This study was reviewed and approved by the Institutional Review Board of Chi Mei Medical Center.
Human rights
This study was conducted according to the World Medical Association Declaration of Helsinki.