
Abstract
Necrotizing fasciitis, officially named by Wilson in 1952, was a rare potentially life-threatening necrotizing soft tissue infections disease. The main lesions showed subcutaneous fat and fascia layer in progressive necrosis, generally not involving muscles. It was characterized by acute onset, rapid progress, and dangerous condition, often accompanied by systemic toxin shock, which was a relatively rare clinical acute critical disease with high mortality rate. Necrotizing fasciitis is a rare but clinical critical disease. The overall incidence of necrotizing fasciitis is approximately 0.04 cases per 1000 persons in the United States, the 30-day mortality is 27%, and necrotizing fasciitis–related mortality in Asian region is about 28%. Streptococcus pyogenes (group A streptococcus) are human-specific pathogens that can cause upper respiratory tract infection such as tonsillitis, associated with post-infection diseases such as rheumatic fever, and also can induce severe invasive diseases such as necrotizing fasciitis and streptococcus toxin shock syndrome. This article reports a case of streptococcus necrotizing fasciitis secondary to suppurative tonsillitis, which was seldom reported before and our successful management with delayed debridement. This study was anonymous and was approved by the local Research Ethics Committee. Informed consent was obtained from the patient.
Case report
A 31-year-old male patient without comorbidities was admitted to intensive care unit (ICU) of Tongji Hospital affiliated to Tongji Medical College, Science and Technology of Huazhong University due to a progressive pain in right thigh for 4 days. There was no documented history of diabetes, alcoholism, and tobacco use. He denied any trauma to his legs, skin breaks, bug bites, inflammatory skin diseases, neuromuscular disorders, or recent travel history. The disease onset was after catching a cold and acute tonsillitis (Figure 1(a)). The syndrome began with fever and chills and the body temperature went up to 39.5°C. A thumb-sized induration appeared on the patient’s right thigh without obvious swelling and pain on day 2. Then the induration expanded in range to half palm size and redness appeared, without pain. After 4 days of intravenous antibiotics, the redness and swelling of right thigh have expanded further, and bruising and large purpura with blister formation have appeared, with severe pain on the lesion site. Soft tissue changes in the right lower limb of the patient are shown in Figure 1(b) to (d). A careful examination clearly showed that it was a much more serious disease since local changes were more prominent compared to erysipelas, which includes epithelial defects and hematoma. Generally, extensively spreading of local changes suggests that the disease develops into a rapidly progressive one. The epithelial defect was more prominent, with worsening hematoma, and the inflammation spreads over the entire leg. On physical examination, the body temperature was 36.2°C, the heart rate was 118 beats/min, the respiratory rate was 20 breaths/min, and the blood pressure was 75/46 mmHg, SPO2 was 100%. The pharynx was hyperemic and the tonsils were red and swollen. There was about 5% size of skin bruising, swelling on the right thigh with unclear boundary, tenderness, and several blisters filled with turbid effusion. Laboratory results were notable for white blood count (WBC) of 8.06 × 109/L, neutrophil granulocyte percentage of 90.9%, and platelet count of 189×109/L. Lactic acid was elevated at 5.17 mmol/L, procalcitonin (PCT) was 35.77 ng/mL, C-reactive protein was elevated at 292 mg/L, creatine phosphokinase (CK) level was elevated at 383 IU/L, and myoglobin was 1203.6 ng/mL. Laboratory parameters of the patient are shown in Table1.

(a) The left tonsil is red and swollen, (b) lesion on right thigh 24 h after admission, (c) skin necrosis on the fourth day, and (d) local lesion was limited on the 10th day.
Laboratory parameters of the patient.
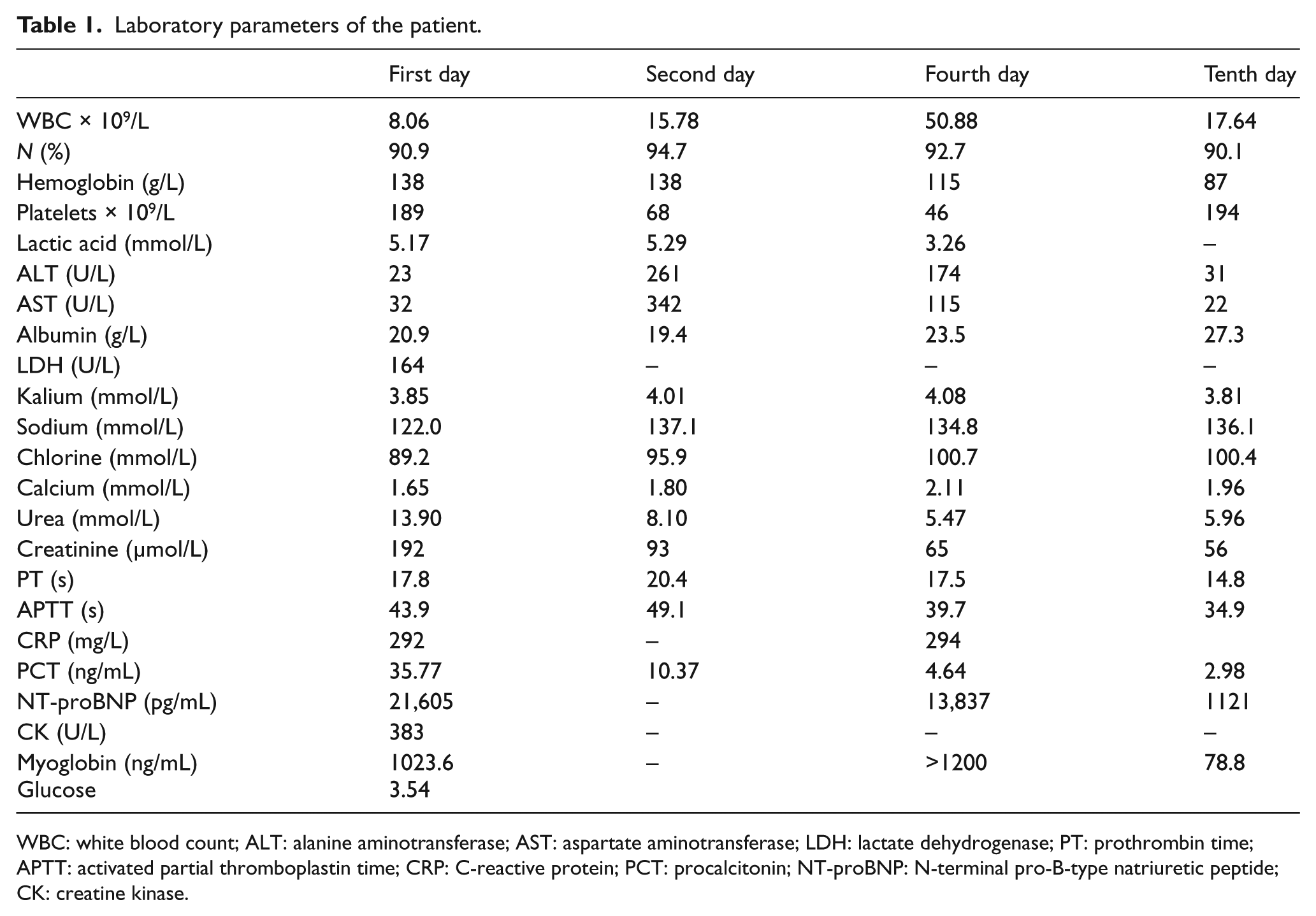
WBC: white blood count; ALT: alanine aminotransferase; AST: aspartate aminotransferase; LDH: lactate dehydrogenase; PT: prothrombin time; APTT: activated partial thromboplastin time; CRP: C-reactive protein; PCT: procalcitonin; NT-proBNP: N-terminal pro-B-type natriuretic peptide; CK: creatine kinase.
Ultrasound check results showed that a left ventricular systolic dysfunction was found (ejection fraction (EF): 35%) and subcutaneous soft tissue was swelling with reductive echo in right-side thigh. Abdominal computed tomographic (CT) scan revealed subcutaneous soft tissue edema in abdomen and right thigh. Lower extremities magnetic resonance imaging (MRI) scan showed widely long T2 signal can be found in the subcutaneous soft tissue and myofascial space of right limb, pelvic, right hip joint, indicating the possibility of infection disease. (Figure 2(a) to (c)). The cultures of throat swab, blood, and secretion swab of the lesion site were both GAS strains. The patient was treated with empiric antibiotic therapy, which combines meropenem, linezolid, and ornidazole. Methylprednisolone and gamma globulin, and continuous renal replacement therapy (CRRT) were applied. Fluid resuscitation and vasopressors were processed to maintain stable hemodynamics. On the third day of admission, intubation was conducted in the situation that the patient developed consciousness disorder and respiration distress. Ventilator and vasopressor were withdrawn on the seventh day after admission. Surgical debridement was performed when the patient was in stable condition and the wound was treated with skin grafting on 30th day. Finally, the patient was fully recovered. Laboratory parameters of the patient are shown in Table 1.
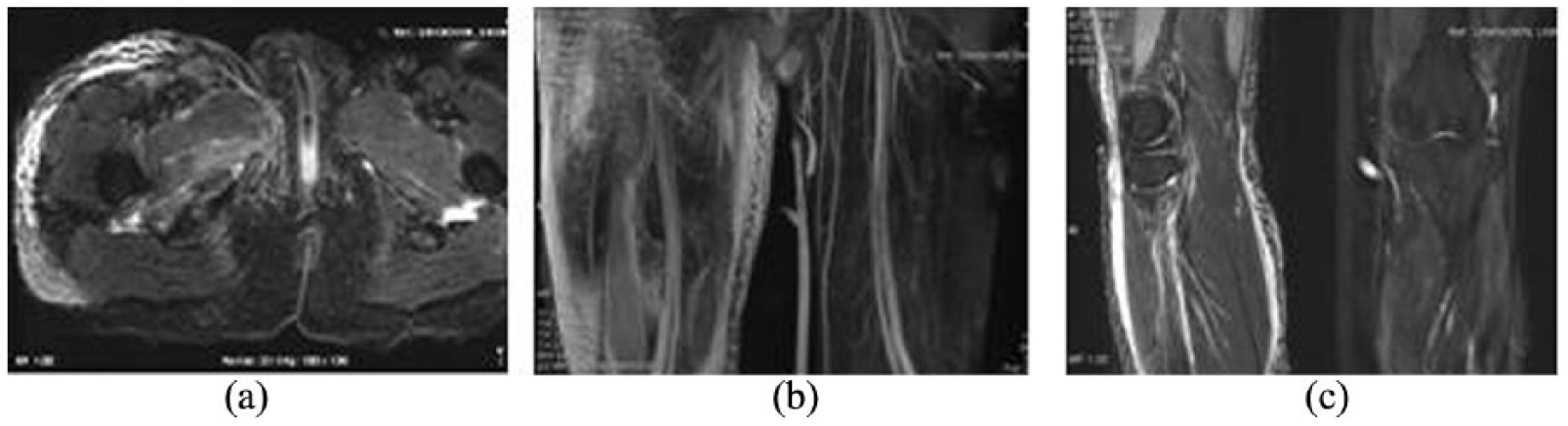
MRI showed diffuse inflammatory lesion in skin and subcutaneous soft tissue without muscle involved.
Discussion
Necrotizing fasciitis (NF) is a rare but clinical critical disease. The overall incidence of NF is approximately 0.04 cases per 1000 persons in the United States, 1 the 30-day mortality is 27%, 2 and NF-related mortality in Asian region is about 28%. 3 NF can occur in any part of the body, while it is more common in limbs, perineum, and abdominal wall. There are no age and gender difference. The process of onset can be fulminant or with an incubation period more than 6 days presenting as a sub-acute process. Based on the causes of the disease, NF can be divided into primary and secondary. Secondary NF is more common in clinical, while primary NF is rare and the cause is more hiding. Secondary NF often attacks systemic or local tissue leading to immune function damage, such as skin damage, and surgery. Patients with systemic immune damage and microvascular lesions are high-risk group, and diabetes mellitus is the most common risk factor of NF. But in recent years, the NF incidence in the group of healthy young people with normal immune function and without disease has increased. As a rare but clinical critical disease, NF can occur in any part of the body, while it is more common in limbs, perineum, and abdominal wall. According to the microbiological culture, 4 NF can be divided into distinct groups. The most severe form of streptococcal NF is the complication of streptococcus toxin shock syndrome (STSS). Type I is infected by polymicrobial flora, synergistic infections that usually are caused by non-group-A streptococci, anaerobic species, and facultatively aerobic bacteria. It usually affects patients with high risk like elderly, patients with chronic diseases such as diabetes, immunocompromised patients, and patients who have recently undergone surgery. Type II infections are usually caused by GAS alone, or in a combination with staphylococci, tending to affect previously healthy young people and frequently presenting as a rapidly progressive disease. The most severe form of streptococcal NF is the complication of STSS. Type III infection, caused by marine vibrios, usually has history of seawater or marine animal exposure. The patient in this case, a young male with healthy physical condition, was infected after a cold. The lesions on the right thigh appeared after acute tonsillitis. There was no obvious local trauma, abrasion and other conditions to destroy the skin barrier. Streptococcus pyogenes was detected in the cultures of throat swab, blood, and secretion of right thigh lesion. Taking these into consideration, we made the diagnosis of streptococcal NF secondary to acute tonsillitis. GAS strains are likely to invade into blood from throat and then spreads through circulation and colonize in optimal anatomical site, finally causing the disease. There are rare reports about streptococcal necrotizing fasciitis secondary to tonsillitis; therefore, the causes of this episode are not clear and whether the lesion site of right thigh is occasional.
Since 1980s, the incidence of GAS-induced severe invasive infectious disease has continued to increase, particularly in NF and STSS. 5 The mechanisms for the emergence of GAS disease are unclear; however, a partial explanation may be the global dissemination of a clonal group of strains of the M1T1 serotype. 6 One of the most severe complications of invasive streptococcal NF is STSS. After invading, pathogen first caused inflammatory response in the subcutaneous deep vein and then formed thrombosis in the blood and lymphatic vessels, which would cause large areas of skin and subcutaneous shallow fascia necrotizing and systemic symptoms such as chills and fever. 7 Histologically, necrosis of the superficial fascia, ploymorphonuclear leukocyte infiltration of the deep dermis and fascia, thrombosis and suppuration of the veins and arteries coursing through the fascia, and microorganism proliferation within the destroyed fascia are seen. The forming of fibrinoid thrombosis in subcutaneous arteriovenous veins is the pathological marker of NF. GAS strains express a variety of virulence factors, including M protein, streptolysins, streptokinase, hyaluronic acid, peptidoglycan, and phosphate acid, the pathogenesis mediated by many secretory and cell wall–related toxins, superantigens, and toxin factors.8,9 Three notable virulence factors associated with GAS infection include emm type mutations in the covR/covS system and the presence of superantigens. 10 In addition, iGAS that caused deep tissue and fascia infections and STSS can produce highly specific toxins with specific pro-inflammatory properties. 9 Studies have found that superantigens are key participants in GAS-induced disruptive tissue infections. 11 GAS can exploit human plasminogen for bacterial translocation across epithelial barrier. 12 Hyaluronidase, M protein, exogenous exotoxin, and a large number of inflammatory mediators can cause severe systemic inflammatory response, leading to extensive tissue destruction and organ dysfunction or even failure.
The typical presentation of streptococcal NF begins with less noticeable trauma and progresses rapidly. The clinical process presents as progressive exacerbation of infection. The main lesion in first 24 h presents as erythema, induration on the skin of lesion site or with pain, but the pain degree is out of proportion to the clinical feature. From the second day to the fourth day of onset, the pain is progressive, accompanied by fever and other systemic symptoms; such as swelling, purple rash, or blister outflow of pus occur in the lesion site. There are no obvious symptoms on the skin; and a small blister, bullae and skin necrosis, subcutaneous emphysema, and twist pronunciation appeared.
From fifth day to the sixth day of onset, septic shock or multiple organ dysfunction syndromes often can be seen. The progression of different types of NF infection is not consistent, fulminant NF is rapidly deteriorating in severe septic shock, and MODS and extensive subcutaneous tissue necrosis occurred within a few hours.13,14 The typical initial manifestation includes severe pain that does not correspond to the physical examination but is usually not shown at onset. Since there is a lack of specific clinical manifestations and skin necrosis appears later, it is difficult to make exact diagnosis in early course of NF. The clinical manifestations of NF are consistent with its microbiologic features. Because the infection is primarily focused on the subcutaneous and deep soft tissues, the overlying skin is initially minimally affected. It is generally accepted that microbial invasion of the subcutaneous tissue begins with inoculation of bacteria from a disruption in the epithelial barrier from minor trauma, cuts, abrasions, needle punctures, or other underlying skin conditions. 15 Our patient’ clinical course was basically consistent with the clinical findings summarized in the literature.
Laboratory tests associated with NF are nonspecific, including an elevated WBC counting and neutrophil percentage increase, elevated C-reactive protein, and PCT. The test results of our patient are shown in Table 1. A notable elevated myoglobin may be explained with rhabdomyolysis caused by sever sepsis since lesion on right thigh did not involve muscle that is shown on CT and MRI. In order to diagnose NF as early as possible and to distinguish NF from other soft tissue infections, laboratory scoring systems have been developed recently. The most important index is the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score, basic factors of LRINEC score are C-reactive protein, WBC, hemoglobin, serum sodium, creatinine, and glucose.16,17 The LRINEC score of our patient was 8 at admission, suggesting a high risk of NF. Studies have found that the LRINEC score ≥6 tends to have higher rates of mortality and amputation. 18 Imaging examinations are helpful for early diagnosis of NF. CT can show subcutaneous tissue inflammatory changes such as fascia edema, thickening, and abscess, showing subcutaneous emphysema. MRI can identify subcutaneous emphysema via signal loss and determine the secondary necrosis and inflammatory edema of the inflammation along the fascia by signal intensity changes, as well as distinguish NF from trauma or other noninflammatory factors. 19
Currently, there are no published guidelines for the optimal management of NF. Treatment must be rapidly conducted and requires multidisciplinary collaboration. Prompt debridement and broad spectrum antibiotics are the important principle for the treatment. In our case, the patient presented a severe infection of right thigh with shock on admission. Then the disease progressed rapidly, vital signs became instable, and organ dysfunction ensuing. With the diagnosis of severe septic, we actively began with fluid resuscitation and other measurements to anti-shock, broad spectrum to anti-infection, and organ function supportive therapy. Empiric antibiotic coverage of suspected organisms is recommended. We don’t know anything about pathogens, considering the dynamic microbiological monitoring of ICU, meropenem, linezolid, and ornidazole were combined application. This combination covered Gram-positive bacteria, Gram-negative bacteria, and anaerobic bacteria, also including the pathogen GAS in this case. Early debridement is currently more recognized. Since our patient was hemodynamically unstable, the debridement was delayed. Our patient was in the condition of shock at admission and rapidly progressed respiration failure on the third day of admission, the prompt treatment was to maintain stable vital sign such as fluid resuscitation, vasopressor, and ventilator supporting respiration. At the same time, potent broad-spectrum antibacterial agents were administrated. In the management of this patient, CRRT to eliminate inflammatory mediators, methylprednisolone to anti-inflammatory, and immunoglobulin to neutralize superantigens as well as other supportive measurements were applied. Surgical debridement and skin-grafting were undertaken when the patient passed through the acute course and was in stable condition. Finally, our patient had a satisfied effect with better prognosis. As known, early diagnosis is important for treatment and prognosis. Because of the characteristics of NF and practitioners’ clinical experience or other reasons, delayed diagnosis and misdiagnosis are very common. So early debridement is not always timely conducted. There have been publications documenting successful nonsurgical debridement of GAS eyelid NF. Under the condition of delayed debridement, we thought comprehensive management including CRRT, steroid, antimicrobial agent, as well as ICU prompt close monitoring played key role in our successful management. Regarding the effect, safety, and necessity of CRRT and steroid in the treatment of NF requires further studies to explore.
Studies has showed that patient’s age is a very important predictor of lethal outcome of NF. 20 Older patients have the poorest survival rate. There was a significant correlation between STSS and prognosis. In patients with STSS, mortality is about 80%–100%, while in those without STSS, mortality is about 30%. 21 The time of diagnosis of NF is also important to prognosis. Multivariate logistic regression analysis showed that surgical debridement time delay of more than 24 h from admission was the only independent risk factor for prognosis after adjusting for age, sex, diabetes, and hypotension on admission. 4
Conclusion
Fatal NF is clinical rare but critically disease, characterized as rapid progression, dangerous condition, and higher misdiagnosis rate. When physical examination does not match with the severe pain and infection progressively aggravates, the possibility of NF should be highly suspected. Early diagnosis should be made as soon as possible. Comprehensive treatment and closely monitoring in ICU contribute to improving the prognosis of NF and reduce mortality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.