
Abstract
Case report
A 91-year-old woman with a past medical history of hypertension and hyperlipidemia was referred by her family physician to our Emergency Department (ED) for suspected appendicitis. She complained of 1 week history of right iliac fossa pain, subjective fever, and anorexia. The pain was colicky, with no radiation, and was associated with some urinary frequency. She had been healthy prior to this episode.
At triage, she had a pulse rate of 88 beats/min, blood pressure of 98/56, and a temperature of 35.9°C. Examination of the abdomen revealed right iliac fossa tenderness together with guarding and rebound tenderness extending to the right flank and back. There were no external signs of a cutaneous infection such as warmth, erythema, crepitus, or open wounds.
Initial blood investigations revealed a raised white count of 25 × 109/L (normal range, 4–10 × 109 cells/L) with neutrophilia, and a C-reactive protein level of 277 mg/L (0.2–9.1 mg/L). Her lactate was elevated at 4.4 mg/dL. Microscopic urinalysis was unremarkable and an erect chest radiograph showed no free air.
A computed tomography (CT) scan of her abdomen and pelvis was ordered and revealed a large multi-loculated right iliopsoas abscess, measuring 7.0 cm by 22.0 cm by 12.5 cm, spreading in the retroperitoneal space from the hepatic flexure cranially to the femoral triangle caudally (Figures 1 and 2). It was suggested that the abscess might have originated from the sigmoid colon as there was a small extension of the abscess which effaced the fat plane of the sigmoid colon (Figure 3). The rest of the bowel including appendix were normal.
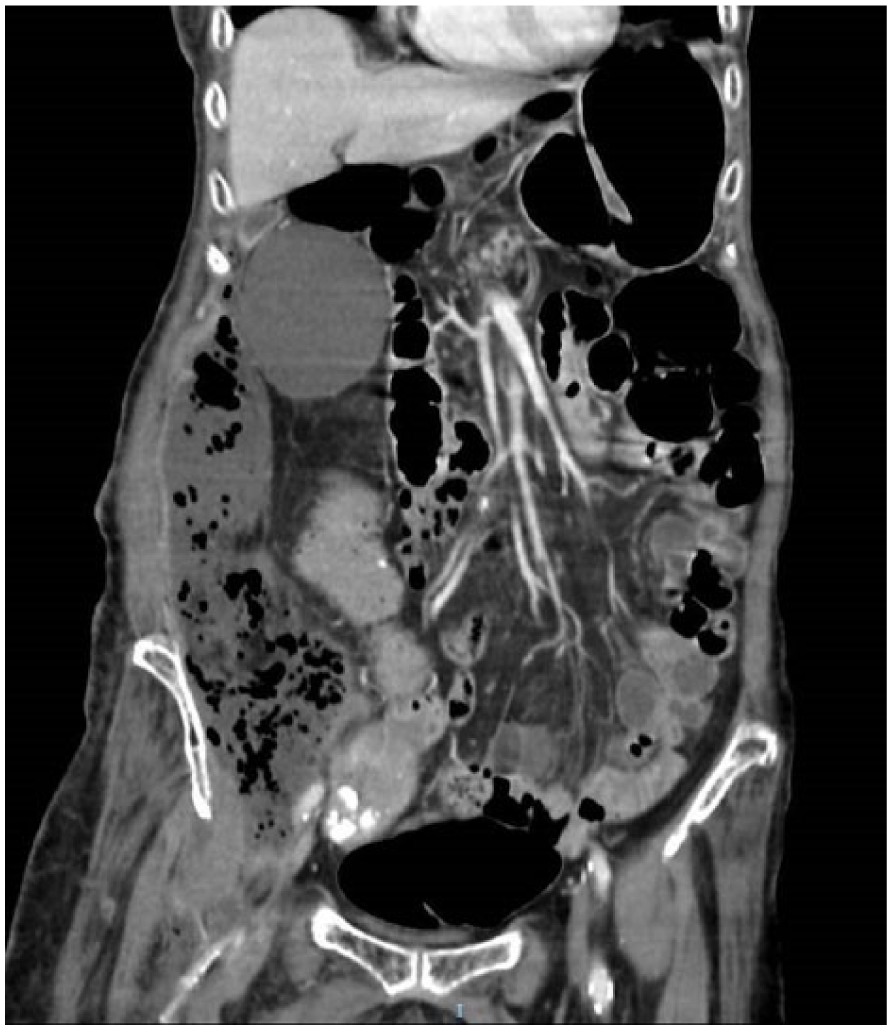
CT coronal view: note the extent of the infection.
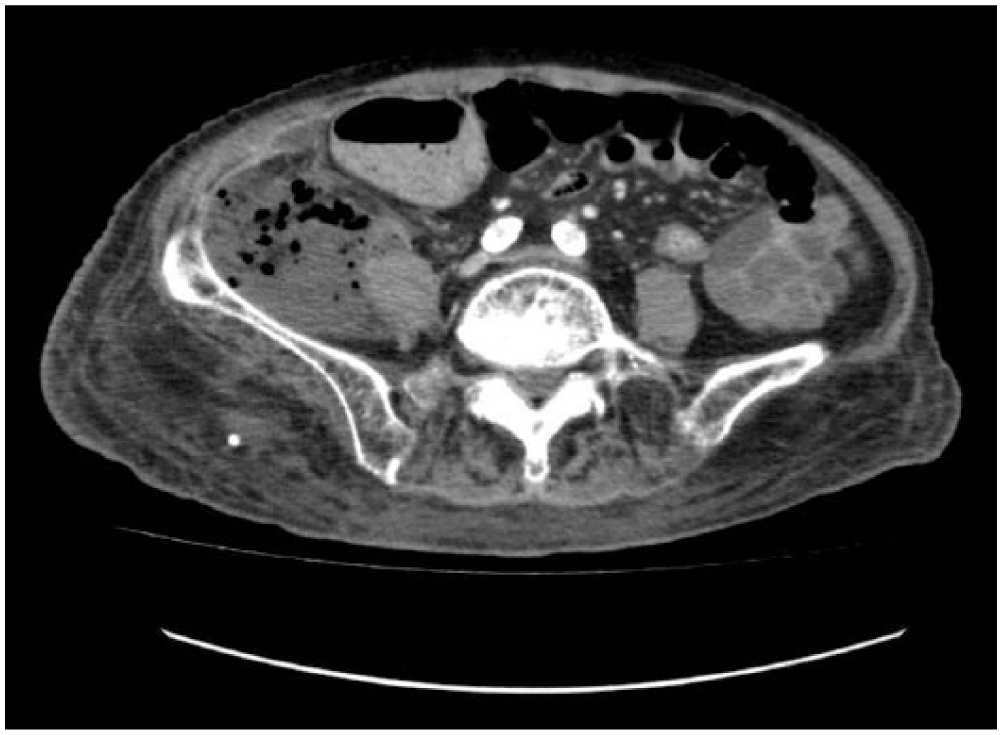
Transverse view on CT.
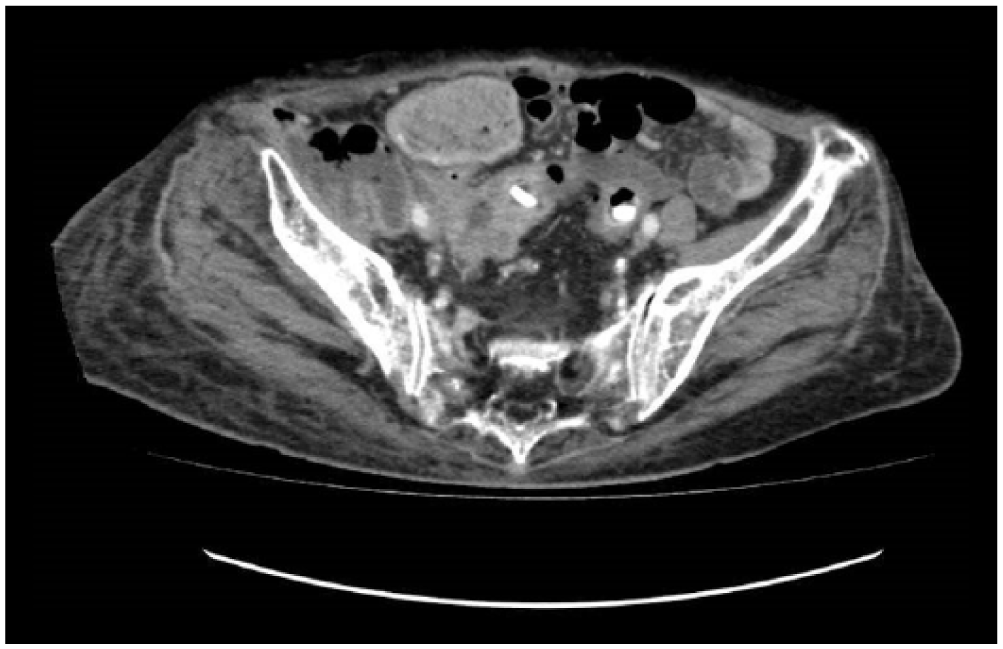
Fat plane of sigmoid effaced by abscess.
She was taken to the operating theater urgently, where copious foul-smelling pus was drained from the abscess, with extension along the fascia in between the internal oblique, external oblique, and transversalis, and also along the fascia of the psoas muscle. The bowel was noted to be clean.
The patient remained in the surgical intensive care unit where her stay was complicated by episodes of rapid atrial fibrillation and septic shock requiring inotropic support. She was empirically started on Clindamycin and Meropenem, which were then changed to Ampicillin and Sulbactam when intra-operative cultures taken showed growth of pan sensitive Enterococcus faecalis and gram positive bacillus. Blood cultures had no bacterial growth. Despite aggressive therapy and repeated debridement and vacuum-assisted closure (VAC) dressing, she developed multi-organ failure and subsequently passed away 3 weeks after admission.
Discussion
Necrotizing fasciitis (NF) is a severe infection of the soft tissue with a reported mortality rate of as high as 73%. 1 It is rare, occurring at a rate of 0.4 cases per 1000 person-years. 2 Risk factors include age, diabetes mellitus and other immunocompromised states, and illicit intravenous drug use. Urgent surgical intervention is key in the management of this condition; however, a lack of obvious cutaneous signs means diagnosis is often late rather than early. 3 Scoring systems 4 have been derived in an attempt to hasten the diagnosis. Sadly, NF still remains one of the most deadly surgical conditions, mainly due to the sudden onset, rapid spread, and resultant overwhelming scepticemia.5,6 Mortality is often divided into early and late. Early deaths are usually due to sepsis and septic shock, while late deaths are often after a protracted hospital course and progressive organ failure. 7
The typical signs of NF such as diffuse erythema, pain out of proportion to the apparent infection, and hemorrhagic bullae are specific but, however, are only 10%–40% sensitive and occur usually in advanced disease. And, despite vital signs being stressed in critical care literature, it has been found that only half of such patients are febrile, and less than a fifth present with hypotension. 8
Retroperitoneal NF due to iliopsoas abscess in an immunocompetent patient is even rarer, and to our knowledge, few such cases have been published. While it has been reported to mimic acute appendicitis, necrotizing NF mainly presents with fever, abdominal pain, and peritonitis. 9 One case was reportedly diagnosed early with the help of periumbilical and flank erythema, which were variants of the Gray Turner’s and Cullen’s signs. 10
Based on reported literature, retroperitoneal NF has been attributed to a wide range of conditions such as pyelonephritis,11,12 diverticulitis,13,14 peri-anal abscess, 15 retroperitoneal stromal cell tumor, and post procedures such as hemorroidectomy, 9 sclerotherapy for hemorrhoids, 16 intramuscular injection of non-steroidal anti-inflammatory drugs, 17 post vaginal delivery, 18 and cesarean sections. 19 The varied presentations, etiologies, and outcomes of case reports published since 2010 are listed in Table 1.
Cases of retroperitoneal necrotizing fasciitis published after 2010.
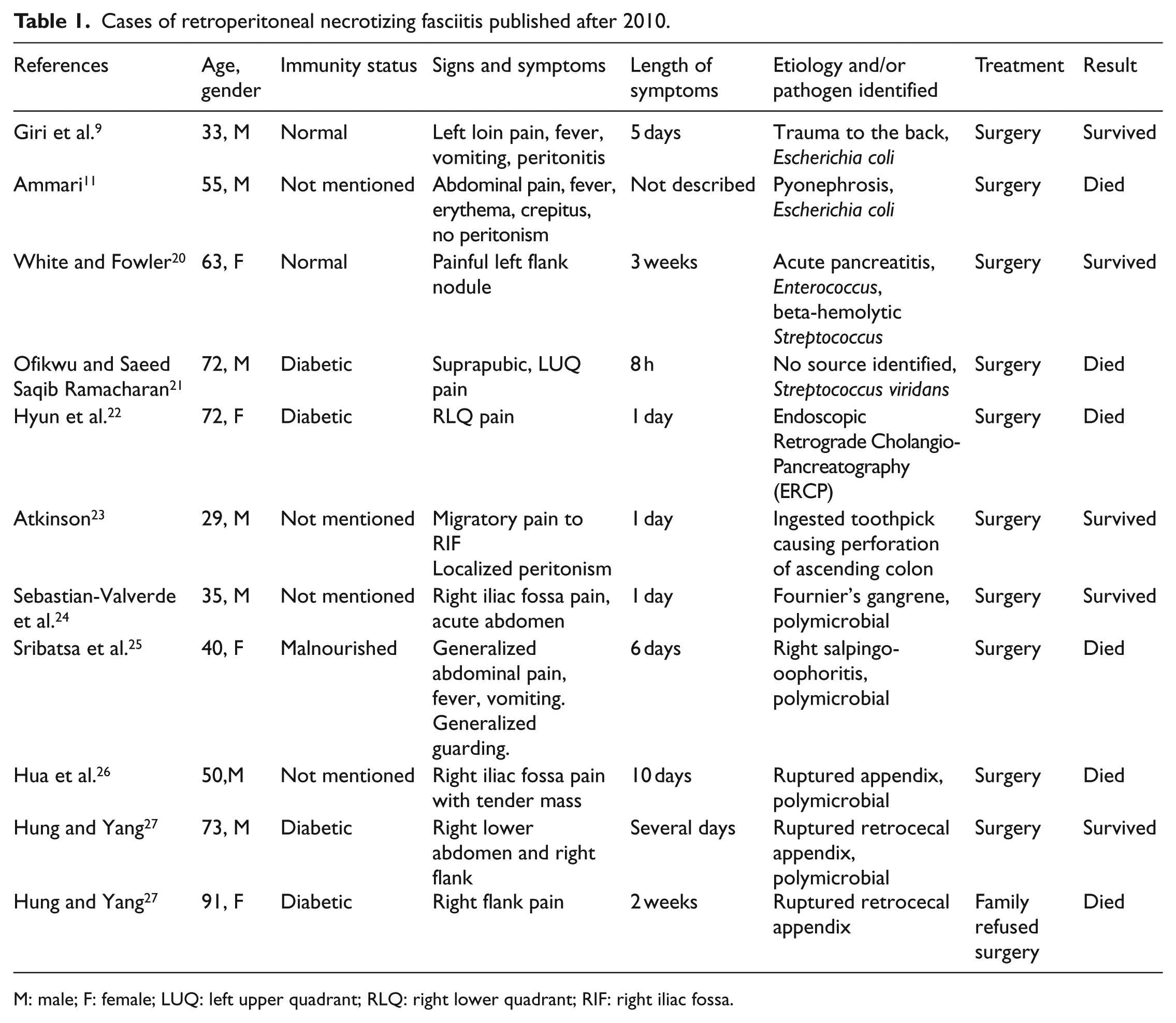
M: male; F: female; LUQ: left upper quadrant; RLQ: right lower quadrant; RIF: right iliac fossa.
In our patient, no obvious source of infection was found. Although her CT scan suggested the sigmoid colon as a source of seeding, intra-operative findings did not concur, while her cultures grew gut commensals. A case series of 19 cases of NF reported a mostly mixed infection, with Bacteroides species isolated from 10 patients. 28 Other associated microbes include Escherichia coli, 9 group A streptococcus, 29 enterobacteriaceae, and Pseudomonas species. Broad spectrum antibiotics including anaerobic and gram-negative coverage must be administered early, preferably within the first 1 h after presentation. 30
However, despite this knowledge, early diagnosis and prompt radical surgical intervention are the only definitive management of NF, regardless of anatomical location. Necrotic tissue is completely removed, with salvageable tissue preserved as much as possible. 31 Mortality rates increase when the extent of the debridement is restricted and if the initial surgery is performed more than 24 h after the onset of symptoms. Close monitoring for 24 h is crucial after the surgery, with repeat surgeries performed if clinically indicated. Wound care in the form of VAC therapy improves wound healing by absorbing exudates, reducing edema and pulling the wound edges together. 30
In our patient who presented a week after onset of symptoms, this might have come too late.
Summary
Retroperitoneal NF secondary to an iliopsoas abscess in an immunocompetent patient is rare and can present atypically. A high index of suspicion is required to diagnose and initiate management. As with all cases of NF, early recognition and surgical intervention are the only definitive treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written consent was obtained from the patient’s son to publish the case together with anonymized data, as the patient had passed away.
Ethical approval
As this is a case report, no ethical approval was required to be obtained.