
Abstract
Introduction:
Ortner’s syndrome is a rare condition, known as cardiovocal condition as patients present with hoarseness of voice due to cardiovascular causes.
Case presentation:
We present a case of Ortner’s syndrome secondary to leaking thoracic aortic aneurysm in a patient who came to emergency department with hypotension and hoarseness of voice for 3 months. Focused cardiac ultrasound (FOCUS) and rapid ultrasound in shock (RUSH) were performed which revealed a thoracic aortic arch aneurysm.
Discussion:
Focused cardiac ultrasound and rapid ultrasound in shock examination in the emergency department had expedited the diagnosis of this rare condition, hence the subsequent definitive investigation and management.
Conclusion:
This case highlights the need for high index of suspicion for thoracic aneurysm in patients with unexplained cardiovocal symptoms. It also highlights the importance of point-of-care ultrasound in the emergency department and the significance of utilizing the suprasternal view to look for pathology at the arch of aorta.
Keywords
Background
Hoarseness of voice due to paralysis of the recurrent laryngeal nerve (RLN) leading to vocal cord palsy is common, with numerous extra laryngeal etiologies. The most common cause of extra laryngeal vocal cord palsy is bronchogenic carcinoma. 1 However, cardiovascular etiologies such as severe pulmonary hypertension, left atrial enlargement, congenital heart disease, and thoracic aneurysm leading to hoarseness of voice have been reported. 2 Chest pain, back pain, or neurological symptoms are the common presentations for leaking thoracic aortic aneurysm (TAA). This article reports a rare case of hoarseness of voice secondary to painless leaking of aortic arch aneurysm. This case highlights the importance of high index of suspicion in patients with hoarseness of voice with associated cardiovascular symptoms and emphasizes on the benefit of bedside ultrasonography in emergency department in expediting this rare diagnosis.
Case presentation
A 70-year-old man, with 4 months history of hoarseness of voice presented to emergency department with signs of undifferentiated shock. The day before admission, he complained of lethargy and an episode of diarrhea. There were no other significant symptoms preceding the presentation. He has hypertension and previous history of endovascular repair for leaking infrarenal abdominal aortic aneurysm (AAA).
On arrival, patient appeared pale and hypotensive (70/40 mm Hg) with a weak pulse. His pulse rate was 90 beats per minute, respiratory rate of 24 breaths per minute, temperature of 37°C, and oxygen saturation is 96% under room air. He had dysphonia with no obvious abnormality in the oral cavity. There were no stigmata of Horner’s syndrome. The right jugular venous pulse was raised and auscultation of the chest revealed muffled heart sounds and bilaterally equal breath sounds. Abdomen was soft and non-tender with absence of expansile or pulsatile mass. Electrocardiogram showed sinus rhythm, no ischemic changes, or electrical alternans. His blood pressure improved after 500 cc of crystalloid infusion.
In view of hypotension, focused cardiac ultrasound (FOCUS) was performed using a 5-MHz phased array transducer. The inferior vena cava (IVC) was 2.2 cm with reduced respiratory variability, inconsistent with his hydration status. Subxyphoid view of the heart revealed pericardial effusion (2.2 cm) without evidence of cardiac tamponade (diastolic collapse of the right ventricle or systolic collapse of the right atrium) (Figure 1(a)). The pericardial collection has mixed echogenicity. A similar finding was seen in the parasternal as well as the apical view of the cardiac ultrasound. Subsequently, suprasternal view was performed and it revealed a well-defined rounded structure at the arch of the aorta distal to the subclavian artery measuring about 6 cm × 6 cm (Figure 1(b)).
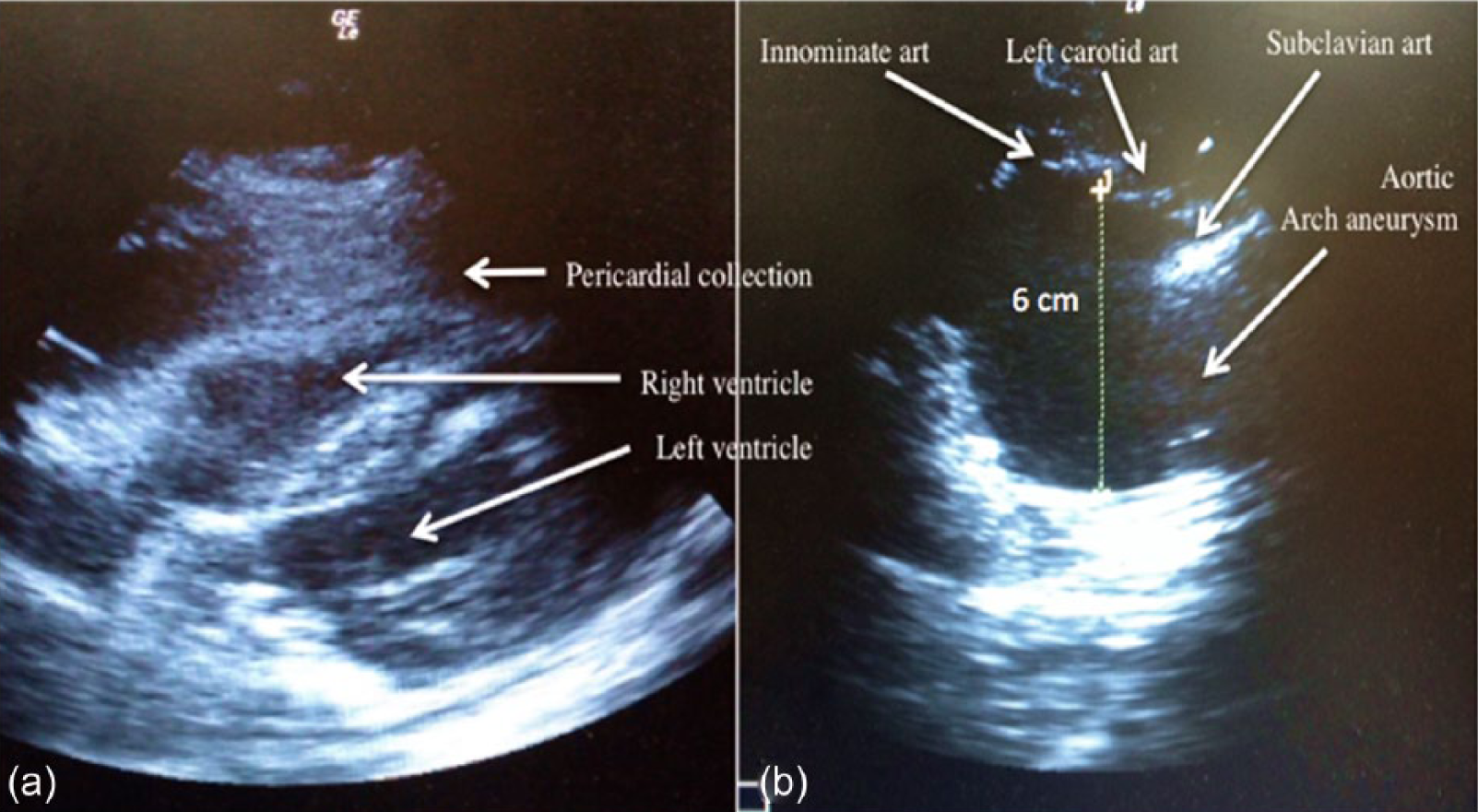
(a) Subxyphoid view echocardiography showing pericardial collection of mixed echogenicity. (b) Suprasternal view showing aortic arch aneurysm, normal anatomy of the aortic arch cannot be appreciated.
Mobile chest radiograph was subsequently obtained and it demonstrated widened mediastinum measuring about 13 cm in diameter (Figure 2(a)). Patient was subsequently sent for urgent computed tomography (CT) angiogram of the thorax, which revealed a fusiform aneurysm of the aortic arch measuring 6.8 cm × 8.6 cm × 7.8 cm. There was also hyper-density (blood) noted tracking down the mediastinum surrounding the heart, which appeared as a huge pericardial effusion from the bedside cardiac ultrasound. These findings confirmed the diagnosis of recent TAA rupture with contained leak.
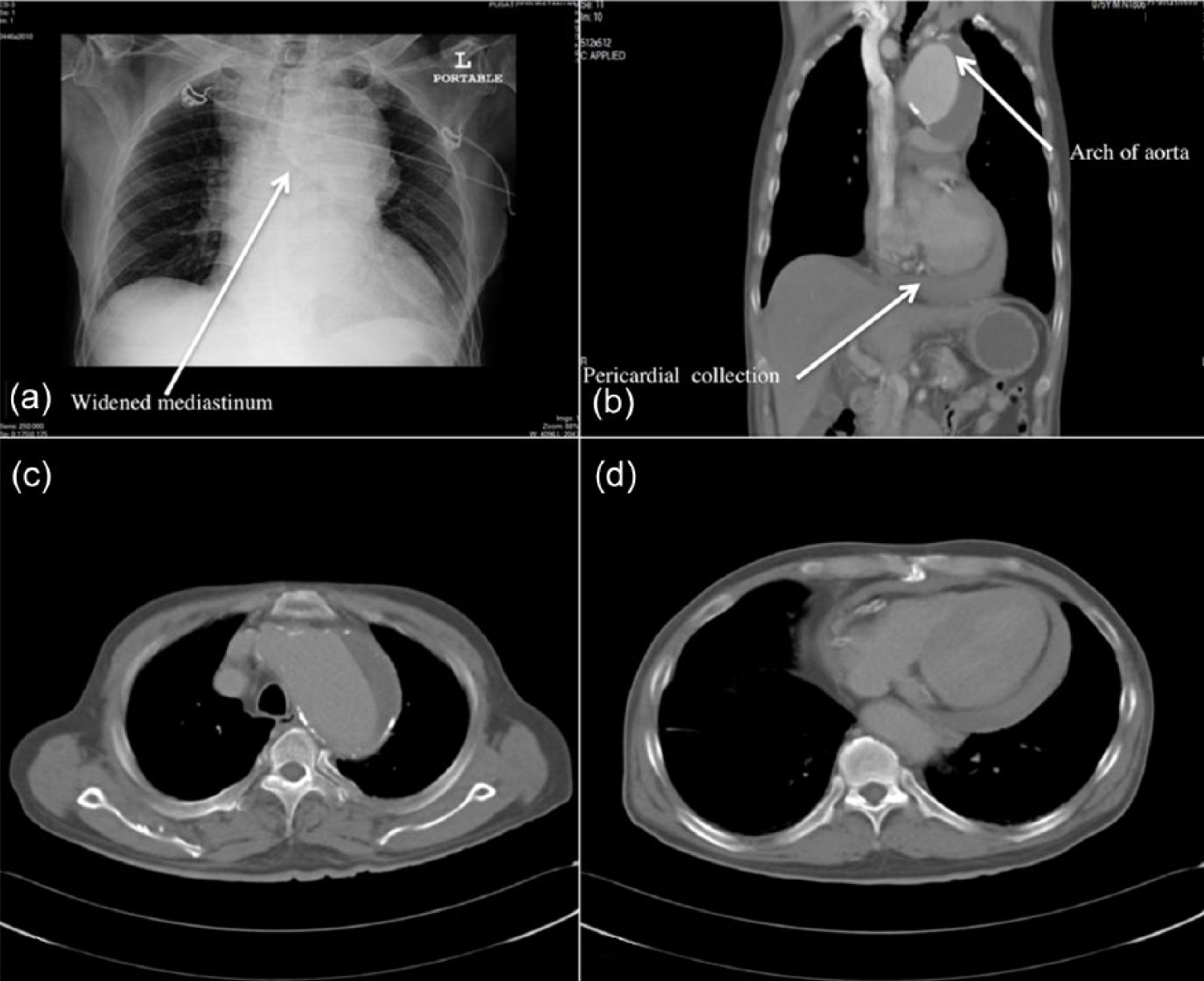
(a) CXR showing widened mediastinum. (b) to (d) CT thorax showing the aortic arch aneurysm and hemorrhagic pericardial collection secondary to the leaking aneurysm.
Fortunately, the patient showed positive response to supportive measures and the hemodynamic status remained stable in the emergency room (ER). He was subsequently admitted to High Dependency Surgery Unit and was planned for an operative repair. Nevertheless, considering that the leak had spontaneously sealed was spontaneously sealed and after series of discussions between the cardiothoracic team, radiologists, and the family members, conservative management was opted by the patient. As the magnitude of risks was high, patient refused to be subjected to any form of operative repair. He was closely monitored in the ward and his condition unexpectedly improved over the week. He was subsequently discharged with cardiothoracic follow up.
Discussion
Ortner’s syndrome is a cardiovocal condition first described by an Austrian Physician, Nobert Ortner in 1897. 3 It was initially described in a patient with vocal cord palsy secondary to left atrial enlargement due to mitral valve stenosis. Ever since, more cardiac causes have been implicated as the cause for RLN paralysis. Cardiovocal syndrome, albeit rare, perhaps is the only major clinical finding of a painless aortic rupture, 4 as seen in this reported case. Knowledge of the basic anatomy of RLN is crucial in understanding the pathogenesis of Ortner’s syndrome. RLN arises from the vagus nerve in the superior mediastinum. The right RLN curls back after crossing the first part of the right subclavian artery to follow a course between the esophagus and the trachea. However, left RLN arises on the antero-lateral aspect of the aortic arch, hooks back in a space called aorto-pulmonary window crossing the ligamentum arteriosum and ascends posteriorly in the tracheo-esophageal groove.5,6 Plastiras et al. 2 concluded that based on cadaveric studies on patients with Ortner’s syndrome, the nerve was compressed between the aorta, ligamentum arteriosum, and the left pulmonary artery. This causes paralysis of the vocal cord which subsequently lead to hoarseness of voice.
Among patients with hoarseness of voice, 11% have rare causes which include cardiovocal syndrome. 5 TAA, being one of the causes, commonly affects the ascending aorta. And, only 10% of these cases involved the aortic arch and mostly are asymptomatic. 7 Any symptomatic TAA warrants surgical intervention, and presence of hoarseness is an indicative of imminent aneurysmal rupture or leaking. 8 The size of the aneurysm is crucial in predicting the risk of complication such as rupture or dissection. About a third of patients with thoracic aneurysm size reaching 6 cm suffer a rupture or dissection. The risk of rupture per annum for TAA measuring 6 cm and 4–4.49 cm is 14.4% and 5.3%, respectively. 9 This patient’s aneurysm measured 6.8 × 8.6 × 7.8 cm from the CT, hence carried significantly high risk of rupture. Therefore, from the emergency perspective, Ortner’s syndrome secondary to aortic aneurysm can be fatal if missed.
Many reported cases of Ortner’s syndrome were incidental findings during ear, nose, and throat assessment.10,11 However, current usage of bedside cardiac ultrasound in the emergency department may help identify this pathology earlier. A consensus statement by the American Society of Echocardiography (ASE) and American College of Emergency Physician (ACEP) emphasized the importance of FOCUS in daily clinical practice and patients’ care as well as its significance for diagnostic evaluation in busy emergency department. 12
FOCUS evaluation principally includes the assessment of pericardial effusion, chamber size, global cardiac function, and intravascular volume status. Labovitz et al. 12 further stressed that FOCUS also helps in other pathologic diagnosis such as left ventricular (LV) thrombus, intracardiac masses, and aortic aneurysm or dissection.
In this reported case, rapid ultrasound in shock (RUSH) protocol was initiated as patient presented initially with hypotension. Its examination integrates early usage of ultrasound into clinical evaluation to rapidly diagnose the cause of shock. It incorporates the physiologic concept of “the pump,” “the tank,” and “the pipes” during the assessment and has shown to improve diagnosis in undifferentiated hypotension. 13 Evaluation of the “pump” means assessment of the cardiac status specifically looking for pericardial effusion, LV contractility, and right ventricular dilatation. It is a crucial first step in determining whether the cause for the shock is cardiac in origin. Presence of effusion with tamponade effect warrants an emergent life-saving pericardiocentesis. Depressed myocardial contractility with shock may indicate urgent need for inotropic support. Whereas, dilated right ventricular dilatation signifies possible obstructive shock, such as pulmonary embolism. Application of FOCUS as part of RUSH examination permits a more comprehensive assessment of cardiac status. Four classical views which are commonly used include parasternal long and short axis view, subxyphoid, and apical views. 14 In this present case, the assessment of the pump revealed a huge pericardial effusion with mixed echogenicity. The contractility, however, was not depressed, and no signs of tamponade was seen.
The assessment of “the tank” is aimed to determine the intravascular volume status by looking at the IVC. In a normal subject, IVC collapses during inspiration due to the negative pressure generated in the thorax. 14 IVC in this case showed diameter of 2.2 cm with reduced variability during breathing. This indicated a high central venous (CV) pressure of > 15 mm Hg and raised suspicion of possible cardiogenic or obstructive shock. FOCUS assessment confirmed the presence of pericardial collection, which studies have shown a high degree of specificity and sensitivity in detecting pericardial effusion. 15
Finally, the third component of RUSH examination, “the pipes” was evaluated. It helps evaluate the arterial and venous circulatory system with particular emphasis on ruling out life-threatening causes such as AAA and aortic dissection. Based on a large study in the year 1998 on aortic dissection in France, two most reliable findings to suggest aortic dissection were the presence of dilated segment of the aorta and visualization of the intimal flap which had specificities of 51% and 100%, respectively. 16 According to the recommendation by European Association of Echocardiography (EAE), suprasternal view is the best view to evaluate the thoracic aorta which primarily depicts the aortic arch and the three major supra-aortic vessels (innominate, left carotid, and left subclavian arteries). 17 Nevertheless, the utilization of suprasternal view in the emergency department particularly for assessment of aorta is still lacking. 18 It is technically, more difficult to acquire a good suprasternal view, as patient needs to lie supine with neck in slightly extended position. The probe needs to be placed in the sternal notch to direct the beam caudally with probe marker pointing towards the left shoulder. In selected patients such as trauma or neck injury patients, it may be impossible to perform such view. However, absence of positive findings in the suprasternal view does not rule out aortic dissection. With high index of suspicion, other more specific imaging modalities must be considered. Although, there is lack of evidence for suprasternal view in RUSH and FOCUS protocol, its utilization in addition to the standard ultrasound views must be recommended. This reported case, highlights the importance of suprasternal view in detecting leaking aortic arch aneurysm, in the context of undifferentiated shock.
Conclusion
In conclusion, Ortner’s syndrome is a rare cause for hoarseness of voice. TAA being one of the causes, carries high mortality if ruptures. The hoarseness of voice may be the only clue of the impending dooms. Therefore, emergency physicians must have high index of suspicion of thoracic aneurysm in patients who present with cardiovascular symptoms associated with change of voice. Point-of-care ultrasound using the RUSH and FOCUS protocol must be routinely practiced in the emergency department in the management of hypotensive patients. This include the suprasternal view as it has proven to expedite the diagnosis and management of life-threatening condition such as depicted in the present case.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the family member of patient for their anonymized information to be published in this article.