
Abstract
Energy drinks are increasingly used worldwide inspite of their side effects. These drinks has been linked to case reports that present with ST-elevation myocardial infarction, but in this case we report a case that presents with non-ST-elevation myocardial infarction after energy drink intake. The patient complained about chest pain after drinking two bottles of energy drink and vodka. Cardiac catheterization subsequently confirmed left anterior descending occlusion in this patient.
Introduction
Energy products are conventionally defined as items marketed and sold as beverages, energy shots (e.g. dietary supplements), as well as in pill or tablet form. The use of these energy drinks (EDs) is also increasing around the world, with a prevalence reported to be as high as 18% in children aged 10 years or younger, 68% in adolescents, and 30% in adults. ST-elevation myocardial infarction (STEMI) is predominantly disease associated with middle-aged and older adults and when found in younger adults it is usually associated with a strong family history. A review of ED toxicity cases with cardiovascular events identified 15 cases (5 atrial arrhythmias, 5 ventricular arrhythmias, 1 QT prolongation, 4 ST-segment elevations). In another review of EDs and myocardial ischemia revealed eight case reports, all of which described an association between huge intake (3 to 20 cans) of EDs and episodes of myocardial ischemia (non-ST-elevation myocardial infarction (NSTEMI)).1–3 Benjo et al. 4 reported a case taking three drinks of vodka mixed with an ED related with left main coronary artery acute thrombosis. In this report, we want to present a case of NSTEMI and established coronary artery disease in a patient with no chronic disease or risk factors.
Case report
A 37-year-old male admitted to our emergency department with a severe pain on sternum that radiates to left axilla and sweating after drinking two cans of ED with vodka 4 h ago. He did not have chronic medication intake and chronic disease history. He was not a regular caffeine consumer or smoker. There was no sudden death or coronary artery disease history in his family history. He drank 500 cc ED that contains caffeine, taurine, niacin, pantothenic acid, B6, B12 and glucose, and 60 ml vodka with 40% alcohol concentration. He did not take any physical exercise after drinking. His vital signs were blood pressure of 110/70 mmHg, heart rate of 102 beats/min, pulse oximetry of 99%, and temperature of 36.7°C. There was no abnormal finding in his physical examination. He underwent electrocardiography (ECG) and laboratory evaluation. There was no evidence of acute coronary syndrome or arrhythmia in his ECG (Figures 1 and 2). Laboratory examination revealed a leukocyte count of 10.41 K/uL (4–11 K/uL), glucose of 127mg/dL (70–110mg/dL), creatinine of 0.79mg/dL (0.5–1.2mg/dL), aspartate transaminase of 64 U/L (0–40 U/L), alanine transaminase of 4U/L (0–40U/L), high-sensitive troponin(hs-Tn) of 700.5 pq/mL (<100 pq/ml), creatine kinase (CK) of 222 U/L (<145 U/L), creatine kinase-MB (CK-MB) of 47.9 U/L (0–25U/L), ethanol of 20mg/ dL and the second hs-Tn of 1219 pq/mL, CK of 749 U/L, CK-MB of 104 U/L. Any toxicology screening was not performed. The patient underwent cardiology consultation and angiography. Only 300 mg acetylsalicylic acid was given orally before catheterization. Cardiac catheterization subsequently confirmed left anterior descending arter (LAD) occlusion in this patient.
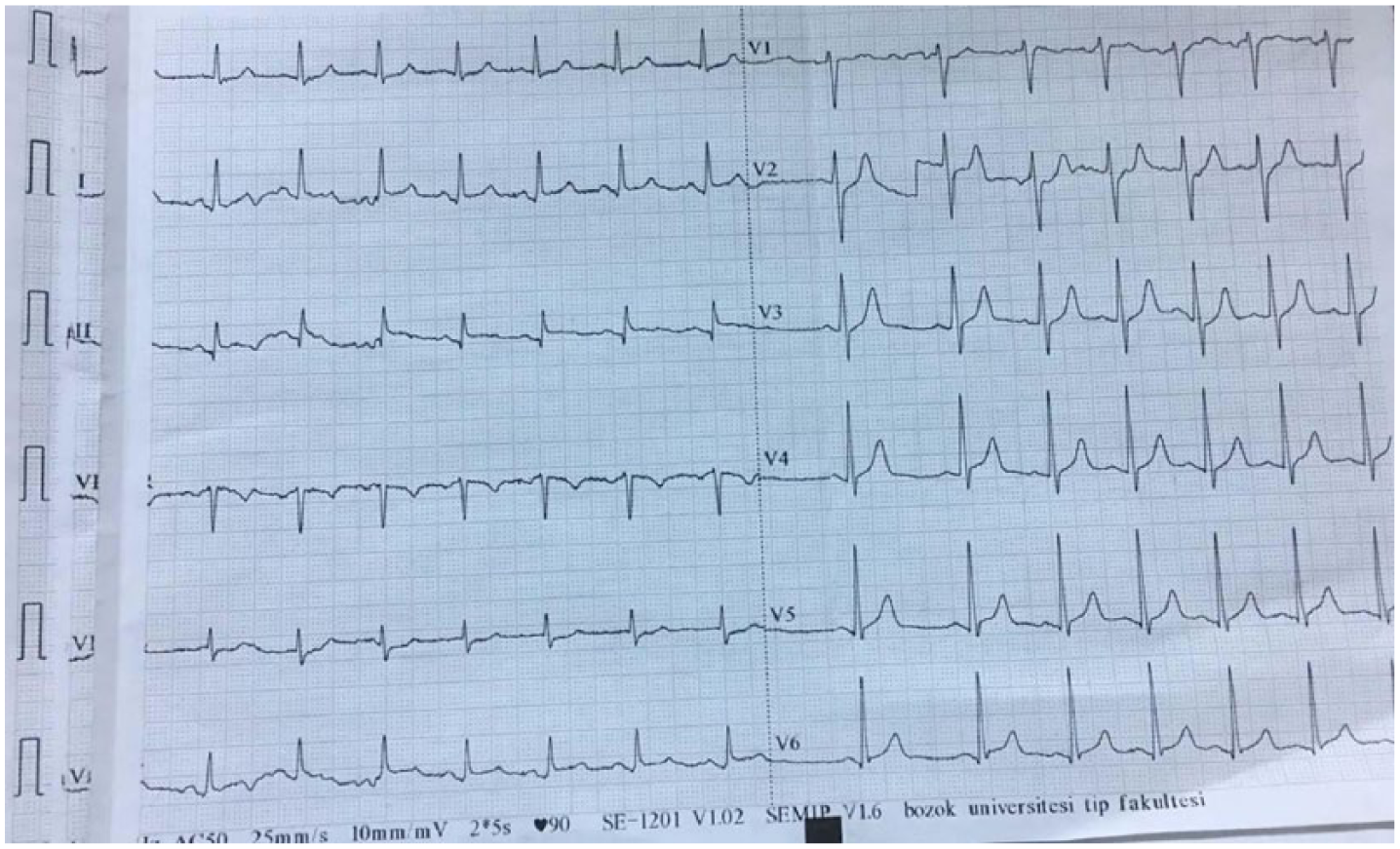
The first electrocardiogram of the patient.
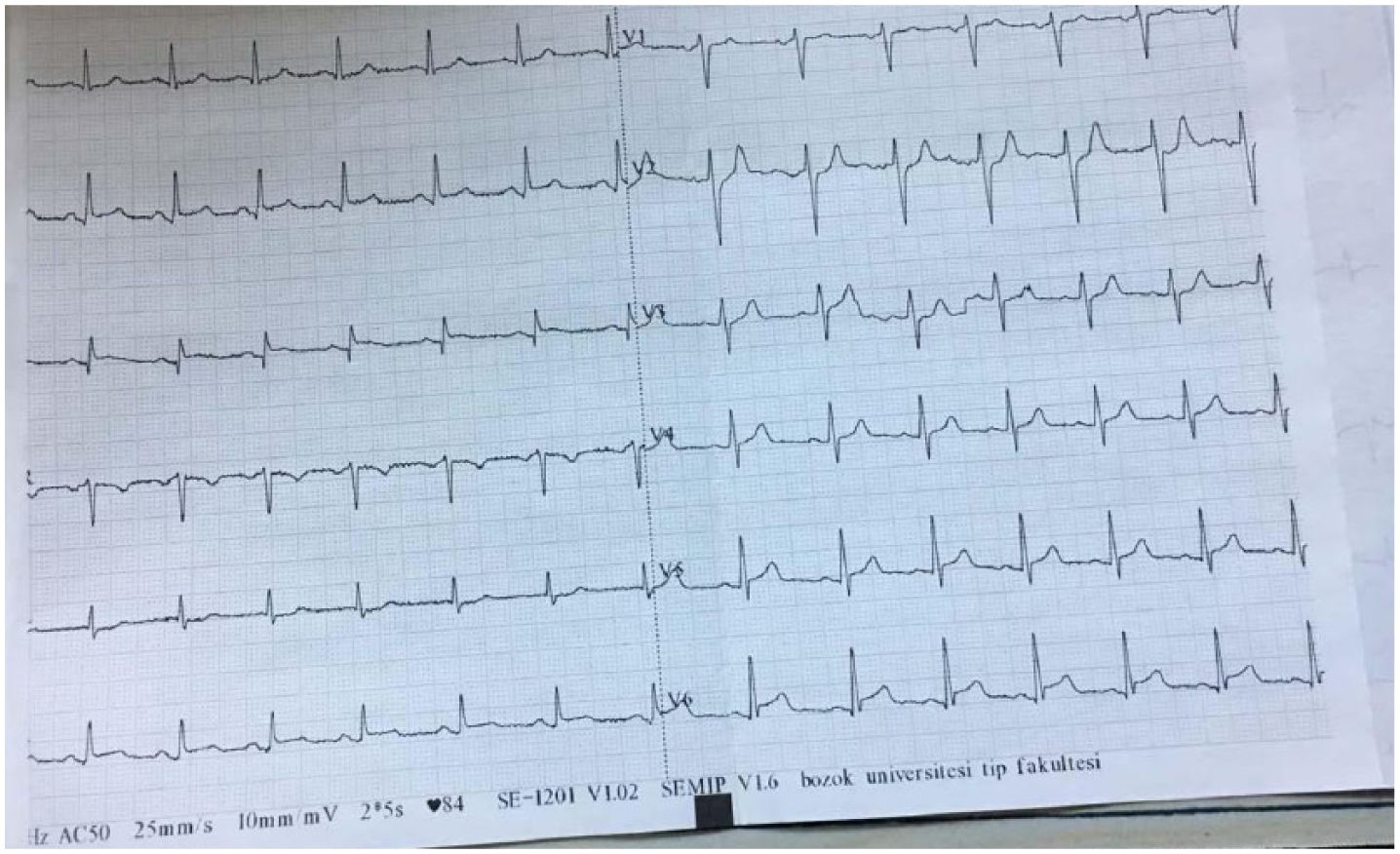
The second electrocardiogram of the patient.
Discussion
Most of the adverse effects and toxic effects related with EDs have been attributed to the high caffeine ratio of EDs. 5 In addition to the high caffeine amount, EDs are usually consumed by young people by mixing with alcohol and other substances and increasing the risk of adverse effects. 6
There are many factors associated with these cases. Most of these EDs contain caffeine and taurine, which are supposed to be the reason of the side effects. The cardiovascular effects of caffeine are perhaps well defined. It primarily inhibits adenosine receptors, induces catecholamine release and it also exerts a physiological effect upon intracellular calcium concentrations within vascular smooth muscle, potentially inducing a coronary vasospasm.1,7
In vitro studies have shown that taurine has an inotropic effect on cardiac muscle similar to that of caffeine and potentiates caffeine-induced muscle contracture. Both taurine and caffeine have been shown in vitro to have physiological effects on intracellular calcium concentration within vascular smooth muscle, and they might induce coronary vasospasm.1,8 The EDs probably may cause increased platelet aggregation, endothelial dysfunction, hyperglycemia as well as an increase in total cholesterol, triglycerides, and low-density lipoprotein cholesterol. 1
The previous case reports reported ST acute coronary syndromes related with large amount consumption of ED. In our case, the patient took two cans and non-ST acute coronary syndrome occurred. Benjo et al. 4 reported a case that the patient alleged drinking three drinks of vodka mixed with an ED. 4 And this case may be the eldest one in the literature when compared with others.
Conclusion
Patients complaining chest pain after ED intake should be searched for acute coronary syndrome in the emergency department. The patients should be monitored, checked with serial electrocardiograms and cardiac enzymes, and undergo cardiology consultation when indicated.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.