
Abstract
Background:
The prognosis of out-of-hospital cardiac arrest is generally poor. It is known that the survival of out-of-hospital cardiac arrest patients depends on treatments delivered in a very short time frame. Identifying outcome-associated factors may provide valuable information for decision-making in clinical practices.
Aim:
The objective of the present study was to assess the associations between various factors (e.g. serum biomarker levels and prehospital factors) and outcomes in adult, non-traumatic out-of-hospital cardiac arrest patients.
Methods:
Data from 386 consecutive out-of-hospital cardiac arrest patients treated from January 2012 to December 2015 at Taoyuan Chang Gung Memorial Hospital (Taiwan, ROC) were collected. While performing cardiopulmonary resuscitation in the emergency room, the levels of creatinine, aspartate aminotransferase, sodium, potassium, troponin-I, hydrogen bicarbonate and haemoglobin were determined, blood pH and pCO2 were measured and the white blood cell count was calculated. The response time and scene time interval were also recorded.
Results:
Here we found that out-of-hospital cardiac arrest patients with blood pH values of <7.34 had a lower chance of survival to 24 h (Odds Ratio (OR) = 2.77), survival to discharge (OR = 7.06) and a good neurological outcome (OR = 64.59). Moreover, patients without an automated external defibrillator shock had a lower chance of being discharged (OR = 4.27) and enjoying good neurological outcomes (OR = 25.09).
Conclusion:
Our data suggest that the blood pH and an automated external defibrillator shockable rhythm are two easily measurable factors strongly associated with the outcomes of out-of-hospital cardiac arrest patients.
Keywords
Introduction
Out-of-hospital cardiac arrest (OHCA) is a primary cause of death worldwide. 1 In Europe, more than 375,000 people suffer sudden cardiac arrests every year; 2 the annual figure for the United States is over 166,000. 3 In industrialised countries, the incidence of OHCA is 0.04%–0.13%, 1 and 11%–48% of OHCA patients have good neurological prognoses after discharge. The mortality rate is 40%–90%.4,5 In Taiwan, it was reported that around 1.4%–6.9% of all OHCA patients survived to hospital discharge.6–9 The low survival rates may attribute to the relative low witnessed rate, low bystander cardiopulmonary resuscitation (CPR) rate and long response interval in remote areas. 7 Although treatments delivered from the onset of an OHCA scene to the emergency room have evolved in recent decades, no significant improvement in survival rate is evident. Most patients die during the earliest stages of OHCA because spontaneous circulation often fails to resume. Patients admitted to intensive care units (ICUs) still experience high mortality rates or survive but with significant disabilities.10,11 Neurological outcomes are generally poor in those discharged from hospital. Consequently, predicting the survival and neurological outcomes of OHCA patients is important to avoid patient suffering and to limit the waste of medical resources.
Previous studies have suggested that several indices, including Glasgow Coma Scale score, 12 brain stem function after return of spontaneous circulation (ROSC), use of emergency medical services (EMSs), bystander CPR, initial cardiac rhythm, time to ROSC and levels of neuron-specific enolase,13–15 may aid in evaluation of OHCA patients and may predict survival and neurological outcomes. Investigations have also been focused on exploring the relationships between laboratory parameters and hospital mortalities in OHCA patients. Whittaker et al. 16 have shown that in addition to prehospital factors like non-shockable rhythm, absence of bystander CPR and downtime >15 min, an initial pH value of ≤7.11 was one of the predictors of in-hospital death. Other laboratory parameters, including blood gas tensions 17 and serum creatinine, 13 were also found to be independently associated with OHCA outcomes. Nevertheless, the discrepancy in factors identified across studies renders it a challenge for real-life applications. Substantial variations in EMS systems among cities or countries also result in the difficulty for the generalisation of cut-offs established elsewhere. Thus, it would be valuable to identify factors associated with OHCA unfavourable outcomes for individual hospitals. In this study, we aimed to explore the association between various parameters (laboratory parameters that are easily and rapidly measurable in combination with prehospital factors routinely recorded by emergency medical technicians (EMTs)) and clinical outcomes for adult, non-traumatic OHCA patients in a tertiary hospital in Taoyuan, a nonmetropolitan city of Taiwan.
Methods
Study setting
This was a retrospective observational study; we analysed data on 386 consecutive OHCA patients treated in the emergency department of Taoyuan Chang Gung Memorial Hospital (Taiwan, ROC) in a 4-year period. The hospital is located in northern Taoyuan City, which has a population of 1,958,686, an area of 1221 km2 and contains 35 fire stations. Taoyuan Chang Gung Memorial Hospital is the only medical centre in Taoyuan City. The local incidence of adult non-traumatic cardiac arrest is over 1500 cases per year.
In Taoyuan, EMTs are the primary providers of prehospital emergency care. In 2010, 104 EMT-1 (this grade is termed EMT-basic in the United States), 666 EMT-2 (EMT-intermediate in the United States) and 36 EMT-P (EMT-P in the United States) personnel were employed at various EMS stations in Taoyuan County. Taiwanese law states that only board-certified EMT-P personnel can perform endotracheal tube intubation and administer epinephrine intravenously. Both EMT-2 and EMT-P personnel can perform the laryngeal mask airway (LMA) technique and place intravenous lines delivering fluids, according to their clinical judgment and discretion. All grades of EMTs can use an automated external defibrillator (AED), depending on their judgment of periarrest conditions. In Taiwan, AEDs are routinely used to treat patients with non-traumatic cardiac arrest. Emergency system records are kept in the Utstein style. EMTs cannot perform thoracotomy or pericardiocentesis in the field.
Basic life support (BLS) is defined as a variety of noninvasive emergency procedures (such as CPR, AED, bag valve mask (BVM) and non-rebreather mask) performed to provide medically necessary supplies and services to patients who are experiencing life-threatening conditions. 18 Advanced life support (ALS), on the other hand, refers to more advanced medical assistance, such as LMA and endotracheal tube intubation, in order to continue the lifesaving care. Whereas intubation is only allowed to be performed by EMT-P, both EMT-2 and EMT-P are allowed to perform LMA.
Data collection
Data from 386 consecutive OHCA patients who did not return to spontaneous resuscitation on admission at Taoyuan Chang Gung Memorial Hospital between January 2012 and December 2015 were collected. Patients who had experienced trauma, who were <18 years of age, who presented with very low temperatures (below 30°C), who did not complete 2 min (five cycles) of CPR in the emergency rooms, who did not receive blood sampling were excluded. The OHCA databases contained regularly collected EMS data from ambulance run sheets and hospital admission notes. These notes were reviewed by the attending doctors, who performed follow-up assessments. The variables included medical histories, co-morbidities, resuscitation times, serum biomarker levels, outcomes, whether the patients survived to discharge and information on neurological recovery. These variables were chosen a priori on the basis of literature and clinical experiences. The neurological recovery was assessed using the Cerebral Performance Category (CPC) scale. The primary endpoint was death within 24 h, and the secondary endpoints were death before discharge and CPC outcome. A poor CPC outcome was defined as CPC grades 3–5. Demographic variables and serum biomarker levels between different endpoint groups were compared.
Blood samples
Blood samples were collected after 2 min (five cycles) of CPR; patients who did not undergo 2-min CPR on admission were excluded. The blood levels of creatinine, aspartate aminotransferase (AST), sodium (Na), potassium (K), Troponin-I, haemoglobin and hydrogen bicarbonate (HCO3–) were measured, and the pH, pCO2 and white blood cell (WBC) count were recorded. Complete and differential blood counts were performed with the aid of a Sysmex XE5000 platform. Biomarker levels were measured with the aid of a BXC 880i instrument. The pH and pCO2 were measured using a Siemens RAPIDPOINT 500.
Definition of response time, scene time interval, transport time and EMS time
The response time was defined as the interval between calling 119 to arrival of an EMS vehicle. The scene time interval (STI) was defined as the time the EMS remained at the scene. The transport time was defined as the time taken to drive from the scene to the hospital. The EMS time was the time that elapsed from calling 119 to the arrival of the EMS vehicle at the hospital, that is, the sum of the response time, the STI and the transport time.
Statistical analysis
Statistical analyses were performed using IBM SPSS software (Ver. 20; IBM Corp., Armonk, NY, USA) and a p < 0.05 was considered to reflect statistical significance. Categorical data are reported as percentages, and continuous variables with normal distributions are reported as means ± standard deviation (SD). The chi-squared test was used for between-group comparisons of demographic categorical variables, and Student’s t-test was used to compare continuous variables with normal distributions. The Youden indices were calculated to identify cut-offs for serum biomarker levels and all time intervals. The power of each cut-off was evaluated by determining the likelihood ratio and the area under the curve (AUC). Odds ratios (ORs) were calculated via both univariate and multivariate analyses.
Ethics statement
This study was reviewed and approved by the Institutional Review Board of Taoyuan Chang Gung Memorial Hospital (Taiwan, ROC; IRB Permit No.: 201600635B0).
Results
Baseline characteristics
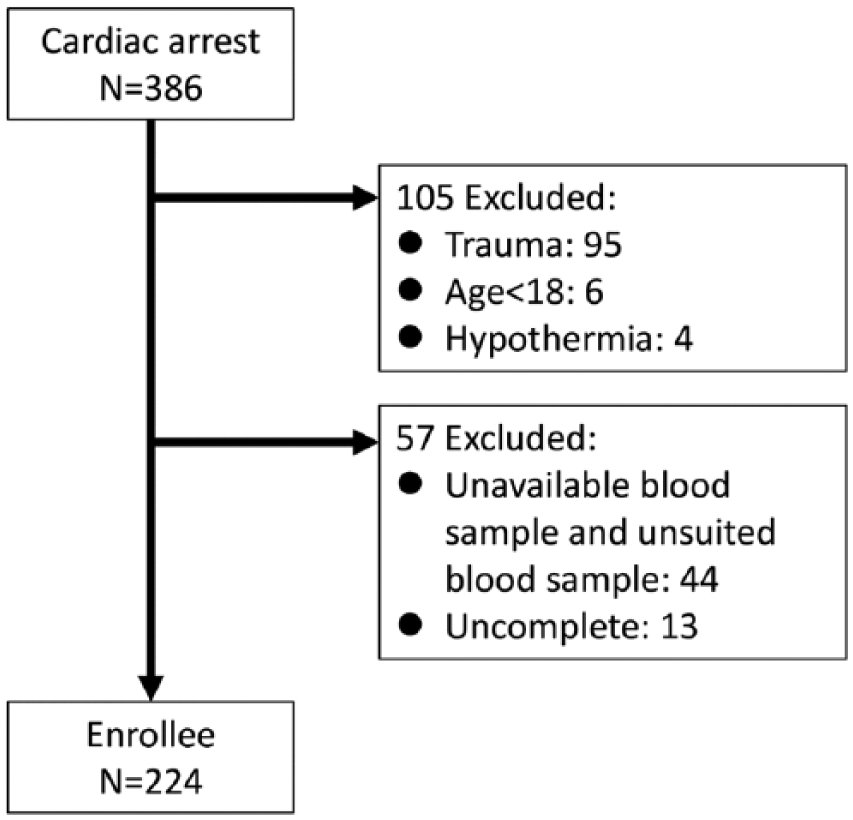
A total of 386 consecutive patients were screened in this study. One hundred and sixty-two patients were excluded by criteria (95 who had experienced trauma, 6 who were <18 years of age, 4 with very low temperatures (below 30°C), 44 who did not complete 2-min CPR (five cycles) on admission and 13 for whom blood data were incomplete (Figure 1)). Among the 224 patients analysed, 67 (29.9%) survived the first 24 h, 22 (9.8%) survived to discharge and 12 (5.4%) survived with good neurological outcomes (CPC 1–2).
Study groups.
Table 1 shows the comparison of baseline characteristics between groups. Statistically significant differences in demographic data, between patients who did versus did not die within 24 h, were evident in terms of gender, initial rhythm, response time, whether the collapse was witnessed, defibrillation by the EMS and the BLS/ALS distribution. The initial rhythm, STI, whether the collapse was witnessed and defibrillation by the EMS, differed in patients who did versus did not survive to discharge. The initial rhythm, STI, the frequency of application of bystander CPR and frequency of defibrillation by the EMS, differed between patients with poor versus good CPC.
Demographic findings of the study population.
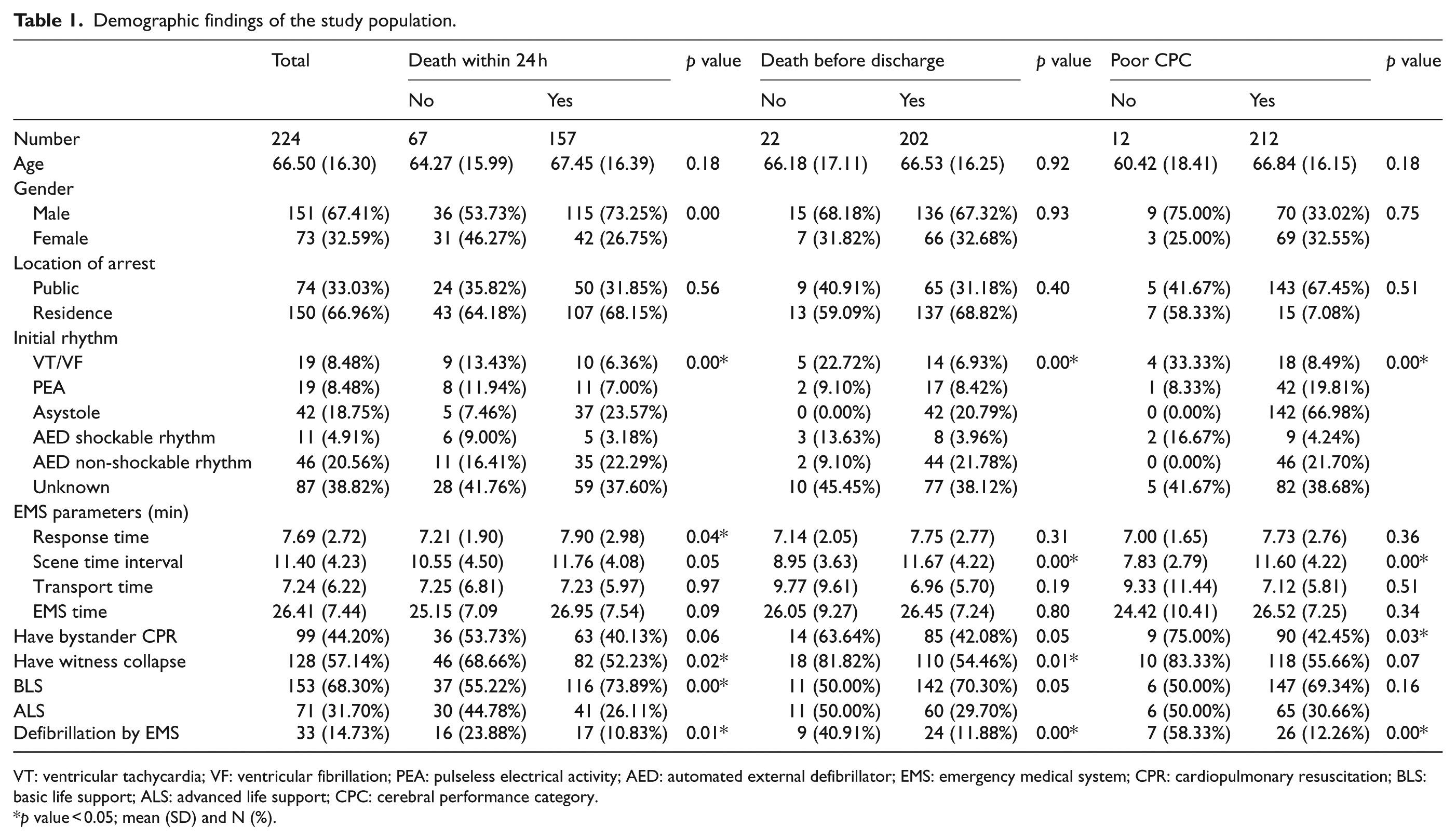
VT: ventricular tachycardia; VF: ventricular fibrillation; PEA: pulseless electrical activity; AED: automated external defibrillator; EMS: emergency medical system; CPR: cardiopulmonary resuscitation; BLS: basic life support; ALS: advanced life support; CPC: cerebral performance category.
p value < 0.05; mean (SD) and N (%).
Comparison of laboratory results
The serum biomarker levels of all groups are listed in Table 2. Patients who died within 24 h had higher Na and K levels, a higher pCO2, a lower body temperature and a lower blood pH (all p < 0.05) than those who survived for more than 24 h. Patients who died prior to discharge had higher creatinine, K, AST levels and pCO2, and a lower temperature and blood pH, than those who survived to discharge (all p < 0.05). Moreover, patients with poor CPCs had higher K and pCO2 levels, a lower temperature and a lower pH compared to those with good CPCs (all p < 0.05).
Temperature and serum biomarkers in all groups.
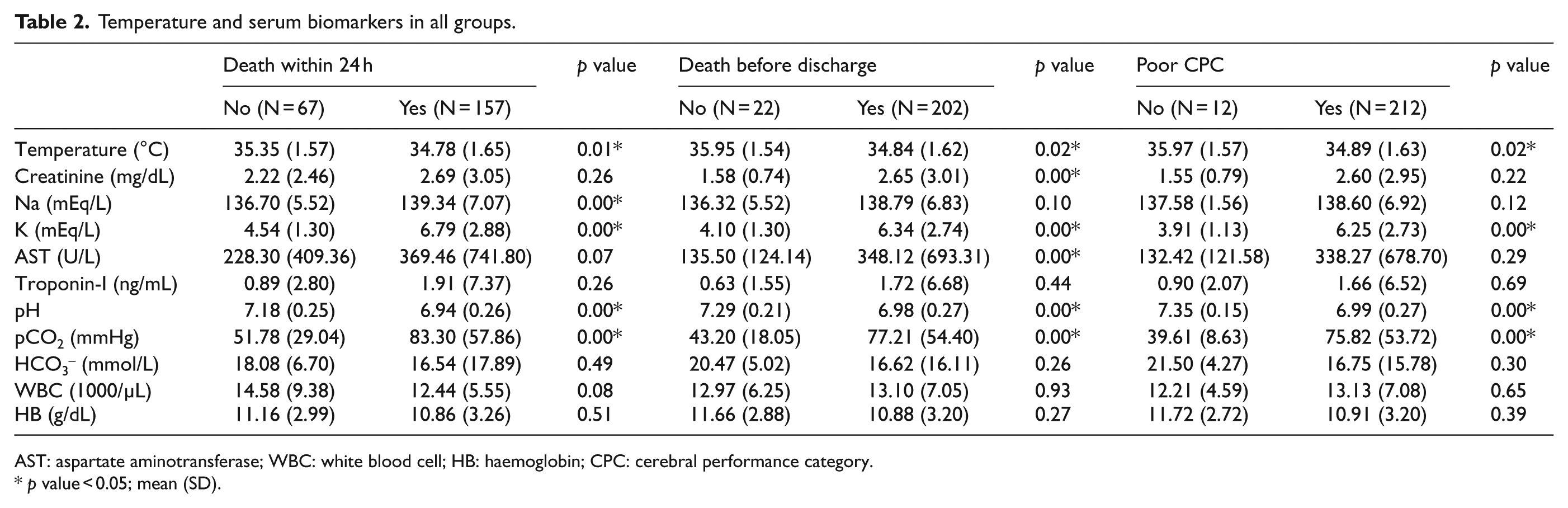
AST: aspartate aminotransferase; WBC: white blood cell; HB: haemoglobin; CPC: cerebral performance category.
p value < 0.05; mean (SD).
The association between individual variables and outcomes
Table 3 demonstrates the association between the collected variables and the outcomes in univariate and multivariate analyses. The best cut-off points for the variables were K = 4.95 mEq/L (AUC: 0.81; sensitivity (SEN): 63%; specificity (SPE): 92%), pH = 7.34 (AUC: 0.82; SEN: 90%; SPE: 63%), pCO2 = 57 mmHg (AUC: 0.75; SEN: 60%; SPE: 91%) and STI = 8.5 min (AUC: 0.69; SEN: 78%; SPE: 50%). The pH cut-off point was close to the lower limit of normal. The K and pCO2 cut-offs were close to the upper limits of normal.
Odds ratio in all groups.
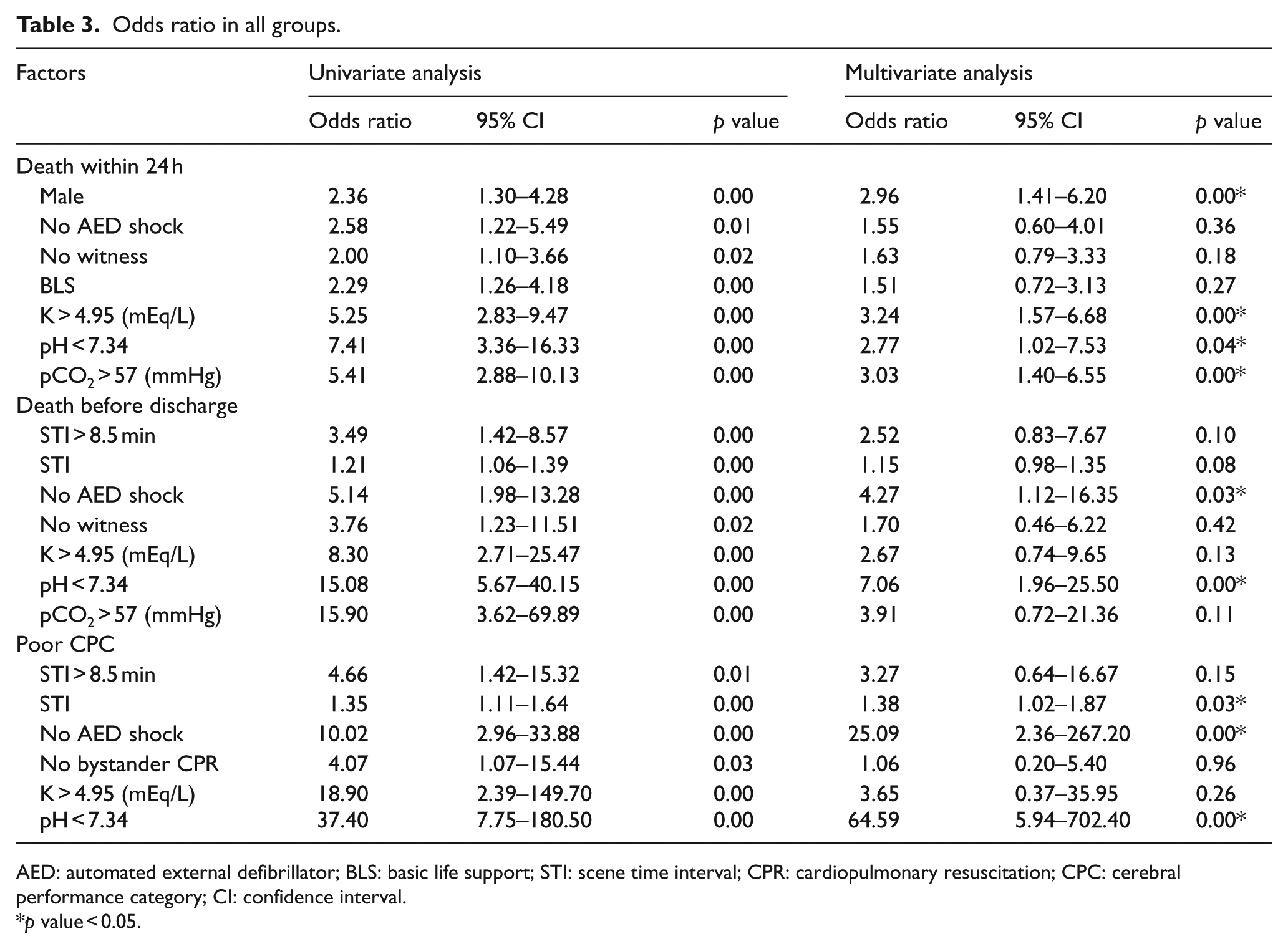
AED: automated external defibrillator; BLS: basic life support; STI: scene time interval; CPR: cardiopulmonary resuscitation; CPC: cerebral performance category; CI: confidence interval.
p value < 0.05.
As can be seen, a significant association is found in multivariate analysis between death within 24 h and male gender (OR = 2.96, 95% confidence interval (CI): 1.41–6.20), K > 4.95 mEq/L (OR = 3.24, 95% CI: 1.57–6.68), pH < 7.34 (OR = 2.77, 95% CI: 1.02–7.53) and pCO2 > 57 mmHg (OR = 3.03, 95% CI: 1.40–6.55). Regarding death before discharge, it is significantly associated with no AED shock at scene (OR = 4.27, 95% CI: 1.12–16.35) and blood pH < 7.34 (OR = 7.06, 95% CI: 1.96–25.50). Similarly, a significant association is found in multivariate analysis between a poor CPC and no AED shock at scene (OR = 25.09, 95% CI: 2.36–267.20) and blood pH < 7.34 (OR = 65.59, 95% CI: 5.94–702.40). Also, the OR for a poor CPC increased 0.38-fold per minute increase of STI.
Positive and negative likelihood ratios
Table 4 shows the positive likelihood ratio (LR+), negative likelihood ratio (LR–), SEN and SPE of a blood pH < 7.34 and no AED shock in death within 24 h, death before discharge and a poor CPC. The LR+ of blood pH < 7.34 were 1.45, 2.46 and 0.14, in death within 24 h, death before discharge and a poor CPC, respectively, and those of no AED shock were 1.17, 1.49 and 2.10, respectively.
The LR+, LR–, SEN and SPE of pH < 7.34 and no AED shock in death within 24 h, death before discharge and poor CPC.
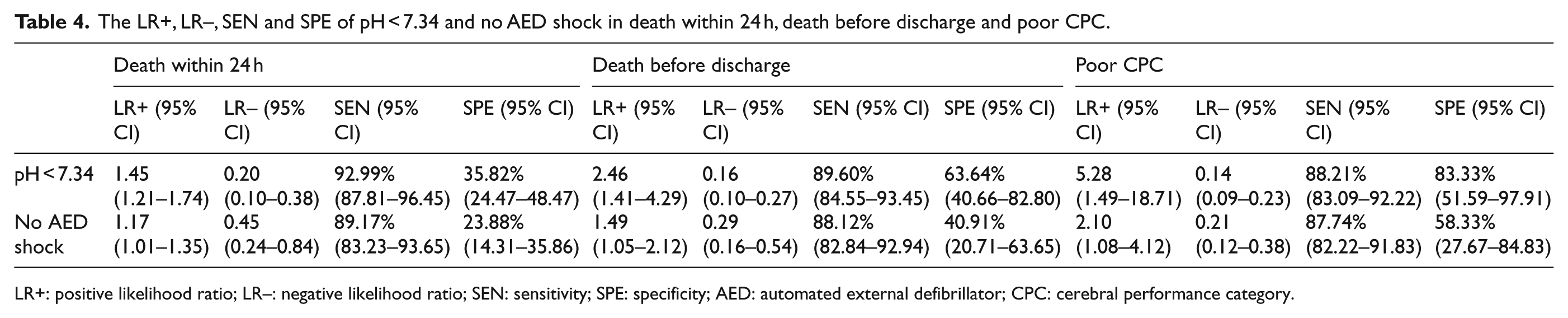
LR+: positive likelihood ratio; LR–: negative likelihood ratio; SEN: sensitivity; SPE: specificity; AED: automated external defibrillator; CPC: cerebral performance category.
Discussion
This was a retrospective observational study aimed to identify the association between prehospital and laboratory measurements and outcomes of OHCA patients. As these variables are routinely measured at resuscitation room of emergency department, they are readily available for physicians and nurses and thus serve as great candidates. Multivariate regression analysis was applied to examine whether the parameters were independently associated with one of the outcomes: death within 24 h, death before discharge and poor CPC. It was found that OHCA patients with lower serum pH values (<7.34) after 2 min (five cycles) of CPR were at a higher risk of death within 24 h, death before discharge and a poor neurological outcome. Moreover, patients without AED shock were less likely to survive until discharge and to have neurological–favourable outcomes.
With a similar setting, Whittaker et al. conducted a retrospective, single-centre analysis of consecutive patients to identify potential factors predictive of in-hospital mortality. The results demonstrated that non-shockable initial rhythm serves as a predictor of in-hospital death (OR = 5.5, 95% CI: 1.34–22.5). 16 Maupain et al., 19 on the other hand, used neurological status as the primary outcome and found that a non-shockable rhythm was one of seven parameters (the others were age, time from collapse to application of BLS, time from commencement of BLS to ROSC, location of the cardiac arrest, epinephrine dose given and arterial pH) that independently associated with poor neurological status (a CPC level 3–5). In agreement with studies mentioned above, we found that patients without AED shock were at a higher risk of death before discharge as well as a poor neurological outcome.
Timing is known to impact OHCA outcomes significantly. In Seoul, the cut-off STIs of 20 and 14 min for in-hospital mortality and poor neurological recovery were reported, respectively. 20 Similarly, Shin et al. 21 suggested that intermediate STI from 8 to 16 min was positively associated with good neurological outcome after OHCA in two metropolitan cities in Asia. These findings were in line with our results that increased STI correlated with poor cerebral performance. Unfortunately, the cut-off value identified (STI > 8.5 min) did not show statistical significance in the multivariate analysis. On the other hand, while that response time was not identified as an outcome variable in this study, other researchers have shown that OHCA survivors had shorter intervals from collapse to arrival of an ambulance (3.5 vs 6 min) or a mobile coronary care unit (MCCU) (5 vs 10 min) than non-survivors, 22 and that a 1 min reduction in response time could improve the odds of survival by 24%. 23 In Taichung, a metropolitan city of Taiwan, 24-h survival and survival to hospital discharge were not significantly different among the groups stratified by response time (<6, 6–12 and >12 min). 6 Other than these discrepancies among studies, the high price of reducing response time renders it not an ideal option from the cost-effect perspective. 15
Upon arrival at an emergency room, a pH value can be easily estimated with a whole blood analyzer and be obtained within 5–10 min. The significance of blood pH has been described in previous studies. OHCA patients with favourable outcomes tend to have higher pH values on hospital admission. 24 It is conceivable that the cut-off points identified for predicting unfavourable outcomes vary from study to study. An initial pH level equal to or below 7.11 was demonstrated to be a predictor of in-hospital death 16 and was independently associated with circulatory failure-related death. 25 Momiyama et al., 26 on the other hand, reported that pH > 7.05 was an independent predictor of favourable neurological outcome (CPC 1 and 2). Nolan et al. 10 showed that for each 0.1 reduction in pH below 7.25, the OR of death increased. Moreover, a combination of low pH level with two other parameters (age and high lactate) could predict a poor outcome after ROSC with a SEN and SPE of 1.0 and 0.51. 27 It is noteworthy that studies above used arterial blood for pH estimations. Due to the retrospective nature of the present study and the technical difficulties in collecting blood samples during resuscitation, whether the blood was arterial or venous could not be fully assured. Thus, although the results suggest that patients with venous blood pH values < 7.34 were at higher risk of all three unfavourable outcomes evaluated (death within 24 h, death before discharge and a poor CPC), it is warranted that the significance of blood pH value should be investigated in a prospective setting for further clarification.
Under physiological conditions, the body pH is closely linked to the pCO2. In a cohort study, survival probabilities could be inferred by measuring PaCO2 and PaO2 levels in post-cardiac arrest patients. 17 In another report using multivariate regression analysis, a patient with arterial pCO2 < 75 mmHg was 3.3 times more likely to achieve ROSC. 28 In this study, we found that patients with pCO2 > 57 mmHg had a higher odds of death within 24 h but not death before discharge or poor CPC, which is consistent with the results reported by Yanagawa et al. 15
The influence of gender on the OHCA outcomes has been investigated by several groups of researchers. The univariate analysis showed that women who suffer OHCAs have lower rates of survival as compared with men. Nevertheless, after adjustment for confounders, no significant difference was found between genders,29,30 indicating that there was no independent effect of gender on OHCA outcomes. In fact, Bougouin et al. conducted a meta-analysis using data from 13 studies (409,323 patients) and concluded that women were more likely to survive to discharge (OR = 1.1, 95% CI: 1.03–1.20) after sudden cardiac arrest. Further studies, however, are needed to confirm the finding and to explore the underlying mechanism causing the discrepancy.
Adrie et al. 13 studied patients who recovered spontaneous circulation after OHCA; those with good outcomes (CPC grades 1 and 2) had a lower serum K level (3.6 mmol/L) compared to those who had poor outcomes (CPC grades 3–5) (3.9 mmol/L). In OHCA patients with severe kidney disease, significantly higher serum potassium and magnesium and lower pH and haemoglobin level were found when comparing with other two groups (normal kidney function or mild kidney disease and moderate kidney disease). 31 A post hoc analysis further showed that patients with severe kidney disease had higher incidences of hypermagnesemia and severe hyperkalemia. 31 In the present study, of OHCA patients who completed 2 min (five cycles) of CPR on admission, those with serum K levels >4.95 mEq/L had a higher OR for death within 24 h. Nevertheless, the cut-off point identified for potassium in this study is close to the upper limit of normal in most laboratories. Whether this cut-off value could be applied in other setting needs to be verified in future studies.
Although our study did not identify bystander CPR as an independent variable influencing the OHCA outcomes, different results have been reported by other researchers. In rural Taiwan, Hung et al. 32 showed that bystander CPR might increase the chance of survival (survival for emergency department discharge; OR = 2.79, 95% CI: 1.28–6.05). Noticeably, although insignificant results with respect to bystander CPR have been reported by various groups,6,7 a meta-analysis performed by Sasson and colleagues concluded that patients who receive bystander CPR have a higher likelihood of survival (OR = 3.9 in studies with low baseline survival and OR = 16.1 in studies with high baseline survival). The data were extracted from 32 studies and contain 76,485 patients with sufficient data for assessing the association between survival and bystander CPR. 11 It was also pointed out by the authors that the highly variable nature of EMS systems may contribute to the heterogeneity between studies.
The East Asian EMS systems are mostly single-tier systems. 33 For these countries, BLS, ALS and AED shock can be applied to, and rhythm analyses are performed on OHCA patients before arrival at the hospital. However, certain details, such as the number of attending ambulance staff and the rescue protocols, differ among countries, which may lead to the different results following analysis. The STI cut-off values are influenced by factors such as geography, crew size of EMS team and regional EMS protocols. The density and distribution of hospitals and EMS stations also markedly affect STI values. Since outcome predictors are highly region-specific, to identify parameters that can be applied to regional clinical practices is of great value for patients who suffer OHCA. Further investigations, perhaps in the form of a large-scale prospective study, are warranted to confirm the significance of factors and their cut-offs identified in the present study.
Limitations
This was a retrospective study that used data from a single local hospital in northern Taiwan, Taoyuan Chang Gung Memorial Hospital. Statistical bias may have been introduced by the small sample size, limited local population and selection bias. In addition, the data collected in the present study did not contain information regarding subsequent treatment, such as therapeutic hypothermia and percutaneous coronary intervention (PCI), which was found to significantly affect survival.34,35 Furthermore, the serum biomarker values varied among laboratories. Thus, the cut-off value identified in a single hospital may not be directly applied to other hospitals or emergency departments. As the study was conducted retrospectively and the technical difficulty in blood sampling during resuscitation, it was uncertain that whether the specimens obtained were arterial or venous. Similar limitations have also been reported by others. 31
The presence or absence of bystander CPR was one of the variable examined. Nevertheless, there was no information regarding the quality and duration of bystander CPR. Moreover, patients who did not receive complete 2-min CPR on admission were also excluded. These criteria were to ensure that the blood samples obtained were under good-quality CPR, and that the results could be interpreted correctly. Nevertheless, selection bias may arise as blood samples were not obtained from some cases or were not suitable for analysis. On the other hand, as the number of on-scene emergency life-saving technicians were found to be associated with survival and neurological outcome for patients suffering OHCA, 36 information regarding the number and levels of EMTs in each OHCA case were not included for analysis. Finally, the disease aetiology (cardiac-cause versus non-cardiac cause OHCA) and medications (e.g. epinephrine) may significantly affect the analysis results; these variables should be included in future studies to clarify the key variables involved in determining OHCA outcomes. The results provided in the present study could only serve as hypothesis-generating and should be verified in future investigations.
Conclusion
The present study demonstrated that after persistent high-quality CPR, OHCA patients with a blood pH < 7.34 have higher chance to have unfavourable outcomes. In addition, patients who received no AED shock also have lower chance to survive to discharge and recovery with good cerebral performance. These two factors identified are easily measured and may be valuable for the decision-making process for OHCA treatment.
Footnotes
Acknowledgements
L.-H.T. and C.-B.C. are the first authors. The first two authors contributed equally to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.