
Abstract
A cecal bascule is a rare cause of intestinal obstruction, and the diagnosis is often challenging because the symptoms and signs are similar to those of small bowel obstruction. We, herein, present the case of an 82-year-old female who presented to our emergency department with lower abdominal pain. Computed tomography showed anterior medial folding of the cecum over the ascending colon with cecal dilatation, without bowel ischemia or perforation. A good outcome was obtained immediately after supportive care. To the best of our knowledge, this is the first report of a cecal bascule that was improved by supportive care.
Keywords
Introduction
A cecal bascule is a rare cause of intestinal obstruction that occurs when a mobile cecum folds upward over the ascending colon and obstructs the ascending colon. 1 Although the signs and symptoms associated with a cecal bascule are less severe than those of other types of cecal volvulus, all reported cases of cecal bascules are treated using operative management.2–5 We, herein, report a case diagnosed with a cecal bascule that was improved by supportive care.
Case report
An 82-year-old female with a history of Parkinson’s disease and hypothyroidism presented to our emergency department with lower abdominal pain. Upon arrival, the patient’s level of consciousness was a drowsy mental state (Glasgow coma scale: 14), her blood pressure was 70/40 mm Hg, her pulse rate was 52 beats/min, and her body temperature was 34.1°C. A physical examination demonstrated abdominal distention and tenderness of the lower abdomen. An electrocardiogram showed sinus bradycardia. Laboratory testing produced the following results: amylase, 266 IU/L (normal range: 36–128 IU/L); lipase, 528.5 IU/L (normal range: 22–51 IU/L); blood urea nitrogen, 45 mg/dL (normal range: 6–26 mg/dL); creatinine, 2.56 mg/dL (normal range: 0.4–1.2 mg/dL); and C-reactive protein, 1.36 mg/dL (normal range: 0–0.5 mg/dL). Urinalysis revealed the followings: white blood cells, >30/high-power field (HPF) (normal range: 0–2/HPF); red blood cells, 21–29/HPF (normal range: 0–2/HPF); leukocyte esterase, 3+; and nitrite positive. All other laboratory test results were within normal limits. An abdominal supine X-ray showed an isolated cecal dilatation of 14 cm (Figure 1). Computed tomography of the abdomen and pelvis was performed to rule out any abdominal disorder; it showed anterior medial folding of the cecum over the ascending colon with cecal dilatation, without bowel ischemia or perforation (Figure 2). The patient was diagnosed with a urinary tract infection with septic shock, hypothermia, and a cecal bascule. Antibiotics and a vasopressor were given to treat septic shock due to the urinary tract infection. A nasogastric tube was placed to aid in bowel decompression. Warm blanket was placed to treat hypothermia. After 2 h, the patient’s blood pressure was 130/80 mm Hg and her pulse rate was 100 beats/min; thus, the vasopressor was tapered. The patient was admitted to the intensive care unit and treated with supportive care. After 7 days, the patient’s abdominal distention was decreased, and a passed stool was observed. After 8 days, a soft diet was started, and she had no abdominal pain or distention. After 27 days, computed tomography of the abdomen and pelvis showed improvement of the cecal bascule (Figure 3). The patient was discharged without any complications.

Abdominal supine X-ray showed an isolated cecal dilatation of 14 cm (white arrow).
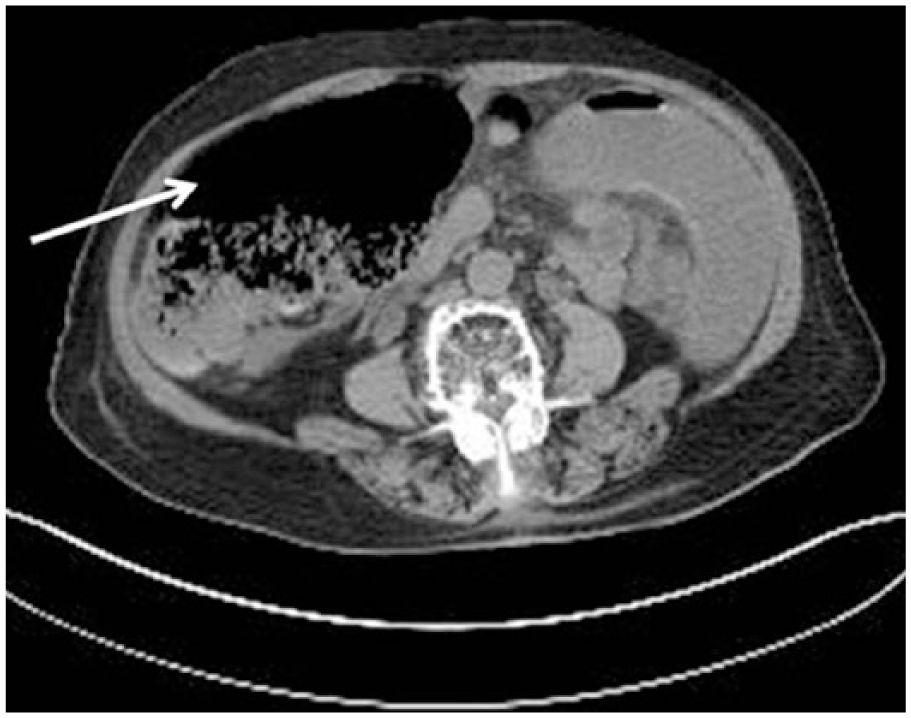
Computed tomography of abdomen and pelvis showed anterior medially folding of the cecum over the ascending colon with cecal dilatation without bowel ischemia or perforation (white arrow).
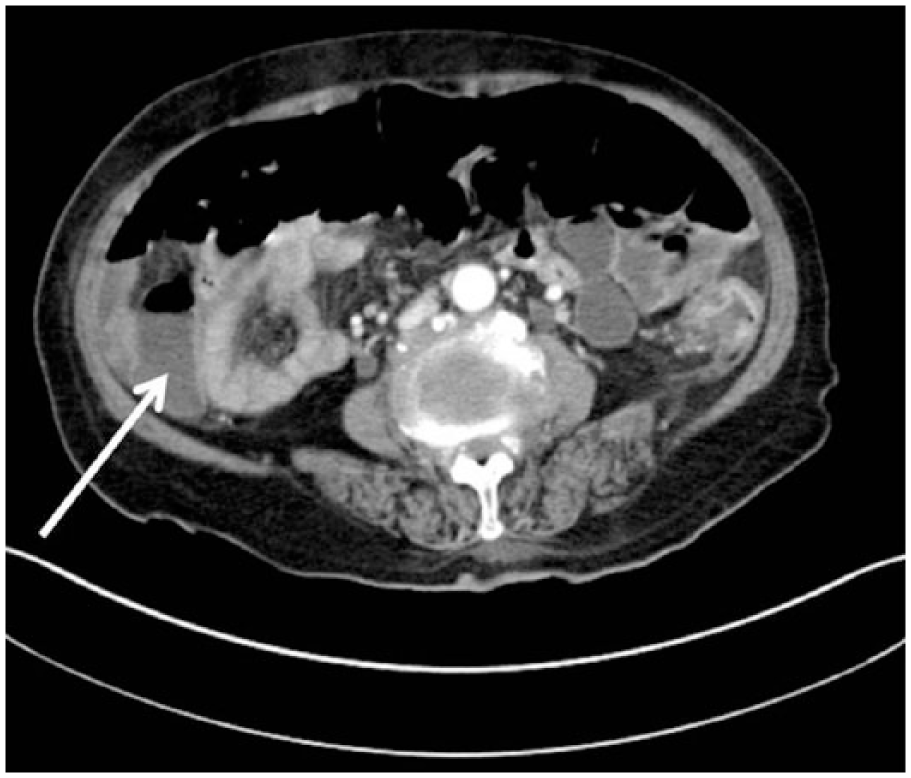
Computed tomography of abdomen and pelvis showed improvement of the cecal bascule with diminution of the cecal dilatation (white arrow).
Discussion
A cecal bascule is a type of cecal volvulus, 6 which accounts for 1% of all large bowel obstructions and 10%–60% of all colonic volvulus cases.6–8 During embryogenesis of the colon, incomplete fixation of the right colon to the retroperitoneum results in an excessively mobile cecum. Although this excessively mobile cecum influences the development of cecal volvulus in certain patients, a cecal volvulus is associated with various conditions, including sepsis, malignancy, hepatic or renal failure, cardiac disease, electrolyte abnormalities, and neurologic and pulmonary abnormalities.2–9 Most cecal volvulus cases occur by twisting of the terminal ileum, cecum, and ascending colon; they are classified as type 1 or 2 depending on the direction of axial twisting (clockwise or counterclockwise rotation, respectively). 2 A cecal bascule occurs when a mobile cecum folds upward over the ascending colon and obstructs the ascending colon. 1 A cecal bascule is classified as a type 3 cecal volvulus; it accounts for <1% of all cases of large bowel obstruction. 6 The patient’s age at presentation is affected by several geographical and dietary influences. 10 Gupta and Gupta 10 reported that the average age at presentation in western countries was 53 years, while Katoh et al. 11 from Japan reported that the peak age in patients treated between 1999 and 2008 was 60–79 years. However, in advanced age, a number of other conditions that decrease colonic motility, including dementia and psychiatric disorders, may cause a cecal volvulus.1,2,12
The clinical presentation of a cecal volvulus is usually similar to that of a small intestinal obstruction and includes nausea, vomiting, abdominal pain, and distention. 3 Although the bowel habits and palpable cecum of the patient may help diagnose a cecal volvulus, the differentiation between a cecal volvulus and small bowel obstruction may be difficult clinically. Additionally, laboratory evaluations are neither sensitive nor specific for the diagnosis of a cecal volvulus, particularly in patients with early acute obstruction; therefore, early radiological evaluations are needed to diagnose a cecal volvulus. 7 On abdominal X-ray film, isolated cecal dilatation in the right upper quadrant with or without a small bowel obstruction may be observed in patients with a cecal bascule; however, these radiologic findings are not pathognomonic signs as are the “coffee bean sign” observed in patients with a cecal volvulus.3,7 A barium enema can be performed to diagnose and reduce a cecal volvulus. However, this modality takes some time to complete the procedure and has the potential for contrast extravasation. Thus, a barium enema is not recommended in critically ill patients with advanced obstruction and in those with suspected bowel perforation and a suspected gangrenous bowel.1,7 Computed tomography is the preferred imaging modality for a more accurate diagnosis and differentiation from other abdominal emergency diseases. 12 Computed tomography of the cecal bascule demonstrates a massively dilated cecum positioned anterior to the ascending colon and an ileocecal valve located in the right upper quadrant. 4 Our case showed anterior medial folding of the cecum over the ascending colon with cecal dilatation that was consistent with a cecal bascule.
Until recently, the definitive therapy for a cecal volvulus, including a cecal bascule, was operative management.1–12 Alternative operative management such as cecopexy and cecostomy was not recommended because of the high risk of recurrence and complications.2,6,7,12 Although the most appropriate operative strategy can be determined by the operating surgeon after considering a patient’s status, the risk of recurrence and complications, and the surgeon’s expertise, a right hemicolectomy and primary ileocolic anastomosis are recommended.6,7 However, in our case, operative management was not performed, and the patient improved with supportive care alone. The extent of bowel necrosis in a cecal volvulus is predominantly determined by the pattern, severity, and duration of the intestinal obstruction. 7 Unlike other cecal volvulus types, patients with a cecal bascule have less severe symptoms and signs because there is no axial torsion of the mesenteric vasculature. Additionally, the cecal bascule may have intermittent subacute obstruction because of flopping of the cecum back into its anatomical position. Therefore, bowel ischemia occurs less frequently in a cecal bascule than in the organoaxial subtypes (types 1 and 2) of cecal volvulus. 5 For this reason, we assumed that bowel ischemia did not occur, and the patient improved with supportive care, without operative management. We agree that operative management is associated with the lowest recurrence and complication rates. However, a minimally invasive procedure may be recommended for the management of a cecal bascule without bowel ischemia, and no prospective trials concerning the management of a cecal bascule have been reported.4,5 Thus, various options for the management of a cecal bascule may be considered depending on the patient’s condition.
Conclusion
A cecal bascule is a rare cause of intestinal obstruction and computed tomography should be considered to aid in its early diagnosis. Until recently, the definitive treatment for a cecal bascule was operative management. However, a cecal bascule causes less frequent bowel ischemia than other cecal volvulus types. In our case, the patient was improved by supportive care and was discharged without any complications. The most appropriate strategy for the treatment of a cecal bascule without bowel ischemia should be determined based on the patient’s condition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.