
Abstract
Carotid artery dissection accounts for 20%–30% of all ischemic strokes in young patients aged <50 years. Recent guidelines on carotid disease management do not differentiate between traumatic and spontaneous dissection. We present a case of a 36-year-old male patient with the right internal carotid artery dissection treated with two XACT Abbot 6–8 mm × 40 mm stents placement after he was strangled during Krav Maga training. It is the most effective way to prevent the imminent stroke in the penumbral region. The safety and outcome of stent placement in internal carotid artery dissection remains unclear and further randomized trials are needed.
Introduction
Carotid artery dissection accounts for 20%–30% of all ischemic strokes in young patients aged <50 years. 1 Although it occurs spontaneously, up to 4% of all dissections are related to severe trauma. Recent guidelines on carotid disease management do not differentiate between traumatic and spontaneous dissection. The recommended medical treatment includes either anticoagulant or a platelet inhibitor.1–4 However, endovascular approach is becoming more popular and might be a better alternative for selected patients.5–7
Case report
A 36-year-old male patient was admitted to the Vascular Surgery Department after strangulation during the Krav Maga training. Krav Maga is a self-defense system developed by the Israeli army that consists of some elements of judo, boxing, karate and wrestling. Directly after the training, he experienced nausea and vertigo. On admission to the hospital, he was conscious with 15 points in Glasgow Coma Scale, but during the physical examination, he demonstrated progressive left-sided weakness, left-sided full Horner’s syndrome, and a rapid respiratory failure.
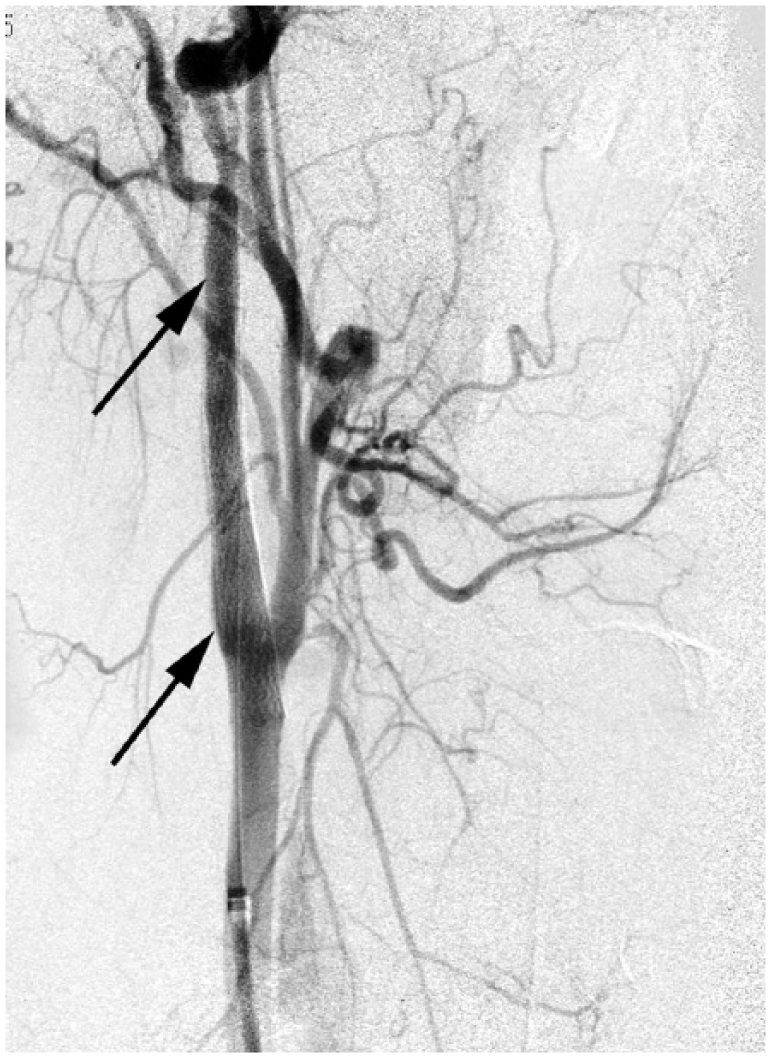
Due to a strong clinical suspicion of stroke, the angiotomography and the digital subtraction angiography (DSA) were performed, which revealed the right internal carotid artery dissection (ICAD) and acute thrombosis in left vertebral artery (Figure 1).

Digital subtraction angiography (DSA) shows the absence of blood flow in the left vertebral artery (black arrow).
At that time, the head CT scan was normal. Patient was immediately transferred to vascular surgery department. The diagnostic angiography confirmed the dissection and showed existence of significant hypoperfusion in the right frontoparietal area of the brain (Figure 2).
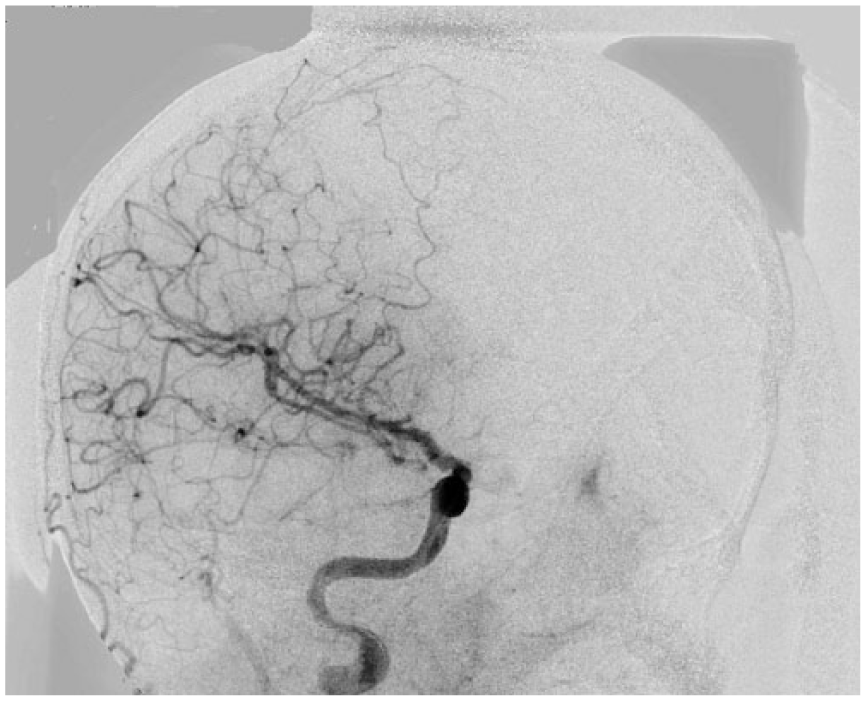
Angiography shows the significant hypoperfusion in the right frontoparietal area of the brain (contrast agent was injected into the right internal carotid artery).
Moreover, a decrease in blood flow on the left side of Willis circle was detected. Therefore, two XACT Abbot 6–8 mm × 40 mm stents were implanted in right internal carotid artery, resulting in fully restored blood flow in right internal carotid artery and normal perfusion in frontal and parietal lobules (Figure 3).
Angiography shows two XACT Abbot 6–8 mm × 40 mm stents implanted in the right internal carotid artery (black arrows).
Due to acute thrombosis of the left vertebral artery, a high dose of intravenous heparin sodium of 5000 IU was administered immediately. The following day, a control brain computed tomography (CT) scan demonstrated extensive left cerebellum infarct and several infarcts in the right frontal and parietal lobe (Figure 4).
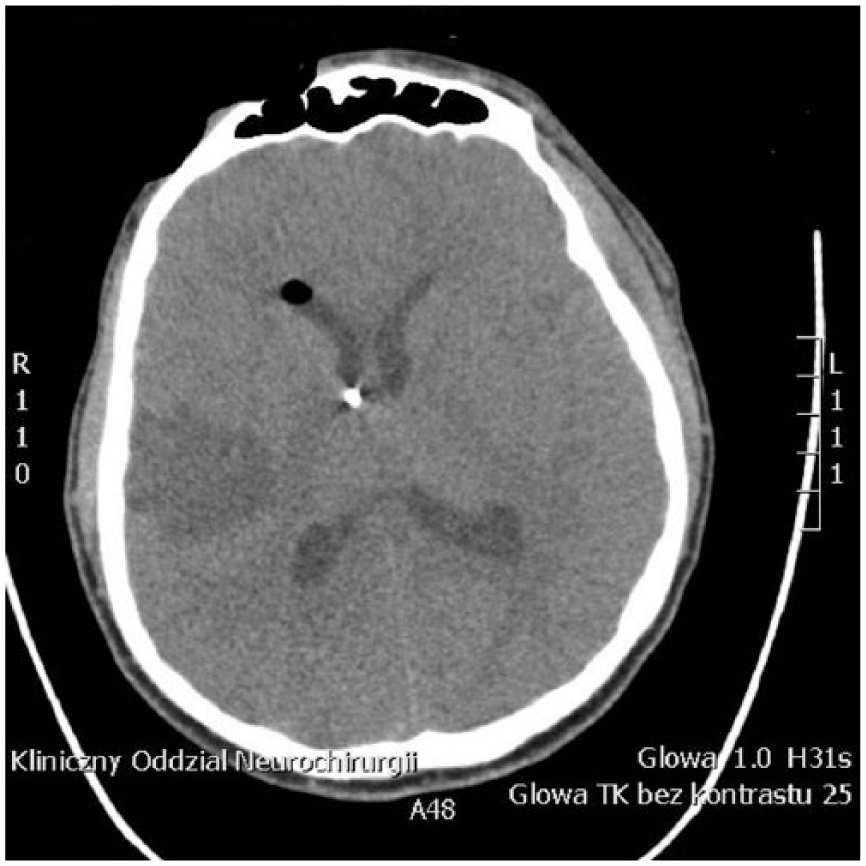
CT scan without contrast shows the extensive infarct in the right frontal and parietal lobes.
Directly after the procedure, patient stayed unconscious, but a few days later, he started recovery of neurological function. Due to extensive infarct of left cerebellum caused by vertebral artery thrombosis, he presents ataxia of the right limbs. Additionally, the left upper limb monoplegia persisted.
Discussion
Carotid artery dissection is a well-known entity, but until now, no evidence-based guidelines for the treatment exist. Although most arterial carotid dissections occur spontaneously, about 4% of them are caused by trauma. 8 The most common example of traumatic dissection is road traffic accident. 9 Usually, it includes blunt trauma or acceleration–deceleration injuries to the neck. However, there have been some cases described in literature caused by strangulation.10–12 Arterial dissection results from an intimal tear that initiates intramural hematoma. Normally, subintimal dissection is the reason of stenosis, while subadventitial dissection tends to cause aneurismal degeneration. 1 The clinical presentation of the traumatic carotid artery dissection varies from being asymptomatic to a fatal stroke. Delayed appearance of focal neurological signs is common and only 10% of cases demonstrate immediate symptoms. Usually, it starts with headache and Horner syndrome on one side of the head and it is followed by acute brain ischemia. Horner’s syndrome results from the damage of the sympathetic trunk and is characterized by the classic triad of miosis, partial ptosis, and loss of hemifacial sweating (i.e. anhidrosis). In our case, one of the first clinical sign was vertigo and nausea and they were related to acute thrombosis of vertebral artery, not to carotid dissection.
According to American Heart Association, the basic management of carotid dissection is antithrombotic treatment with either an anticoagulant or a platelet inhibitor (Class IIa). 1 The recent randomized studies show no difference between antiplatelet and anticoagulant drugs at preventing strokes after carotid dissection; however, they did not compare it to endovascular treatment. 4 The recommendation of using antithrombotic medications is based on the opinion that the most common mechanism of stroke after cervical artery dissection is embolization of thrombi on the intimal flap. 13 Another cause of a stroke is hemodynamic hypoperfusion made by critical stenosis of a true arterial lumen.14,15 In our case, right carotid dissection was a reason for insufficient blood circulation in the Willis circle. Moreover, we detected hypoperfusion of the total right, frontoparietal area of the brain. To prevent the imminent evolution into an irreversible stroke of the whole ischemic region, an immediate action had to be taken. Only stent placement was the way to restore the proper blood flow in the brain arteries and to decrease the area of brain ischemia. Six hours after the cessation of the blood supply, neurons started to irreversibly damage. During this period of time, the brain cells in the penumbra zone can still be salvaged and patient can achieve better neurological outcome.
Stenting can be especially appropriate treatment in the acute, clinically dynamic phase of dissection when there is neuroradiological proof of the hypoperfusion or a large penumbra existence. This kind of treatment may change the clinical course toward a favorable outcome.
In addition, in our case, we used antithrombotic treatment due to acute thrombosis of the left vertebral artery, which was revascularised in control angiography after 2 weeks. Due to extensive stroke of the cerebellum, significant ataxia persisted.
Conclusion
We think that in acute traumatic carotid dissection, in case when there is still vital brain tissue to salvage, the best medical treatment is stent implantation. It is the most effective way to prevent the imminent stroke in the penumbral region. The safety and outcome of stent placement in ICAD remains unclear and further randomized trial should be done in this subject.
Footnotes
Acknowledgements
No writing assistance was required for this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article.