
Abstract
Aortic dissection is a life-threatening cardiovascular emergency, and despite medical advances, its diagnosis is often shrouded by the diversity of its clinical presentation. Physician must have high index of suspicion, especially in those with unusual combination of features that may occur in acute painless dissection. We report a case of a man presented with right-sided weakness and syncope associated with pulse deficits at multiple levels. Physical examination of the lower limb is consistent with acute limb ischemia. Computed tomogram thorax done after emergency embolectomy revealed extensive Stanford type A aortic dissection down to the level of abdominal aortic bifurcation. The diagnosis of aortic dissection is delayed due to his atypical symptoms, which is likely resulted from malperfusion syndrome of aortic dissection.
Introduction
Aortic dissection is a life-threatening condition and a cardiovascular emergency. The rarity of aortic dissection is established in a study done in the United States where the frequency of aortic dissection is reported to be 1 for every 12,200 visits to emergency department (ED). 1 The hallmark feature of aortic dissection is the sudden onset of chest pain radiating to the back; however, painless dissection may occur in between 5% and 15% of cases. 2 Unfortunately, the diagnosis of aortic dissection remains elusive despite advances in its diagnostic imaging and treatment. This is contributed mainly by its diverse clinical presentation and may not associate with sudden onset of pain. Diagnosis of aortic dissection in atypical presentation such as neurological symptoms is often overlooked. Unusual combination of clinical features should raise suspicion of an underlying vascular pathology such as aortic dissection. 3 This matter is illustrated in a case of aortic dissection presented with classic symptoms of cerebrovascular accident (CVA) but with clinical signs of acute limb ischemia. We emphasize the discussion on association of neurological symptoms as predominant features and explore the subject of malperfusion syndrome in aortic dissection.
Case report
A previously well 44-year-old man presented with a complaint of sudden onset of right-sided weakness, predominantly in the lower limb. He had a brief syncope after the onset of weakness and was fully conscious on arrival to the ED. Vital signs on arrival to ED were unremarkable with blood pressure (BP) 124/70, heart rate of 64 beats per minute, respiratory rate of 16 per minute and oxygen saturation of 98% under room air.
There was discrepancy in the BP of both upper limbs with right-arm BP of 115/69 mmHg and left-arm BP of 83/52 mmHg. Cardiovascular, respiratory and abdominal examinations were unremarkable. Examination review noted that right leg was cold. The femoral to dorsalis pedis pulses was absent. Left radial pulse was also feeble on palpation. Other pulses were normal. These findings were confirmed with bedside Doppler assessment. Neurological assessment noted that power over right upper and lower limb was 3/5 (movement against gravity according to Medical Research Council scale for assessing muscle strength) with normal tone and hyporeflexia over the affected side.
Electrocardiogram showed normal sinus rhythm. Bedside ultrasound revealed aortic root of 5 cm with no pericardial effusion. Abdominal aorta was 1.7 cm. His initial venous blood gas showed mild metabolic acidosis and high lactate level of 5 mmol/L. There was mild acute kidney injury noted on renal profile and mild derangement of liver function with bilirubin of 28.5 mmol/L, alanine aminotransferase of 804 mmol/L and alkaline phosphatase of 67 mmol/L. Other blood investigations were normal. Chest radiography of anteroposterior view showed mediastinum width of 9.2 cm (Figures 1 –4).
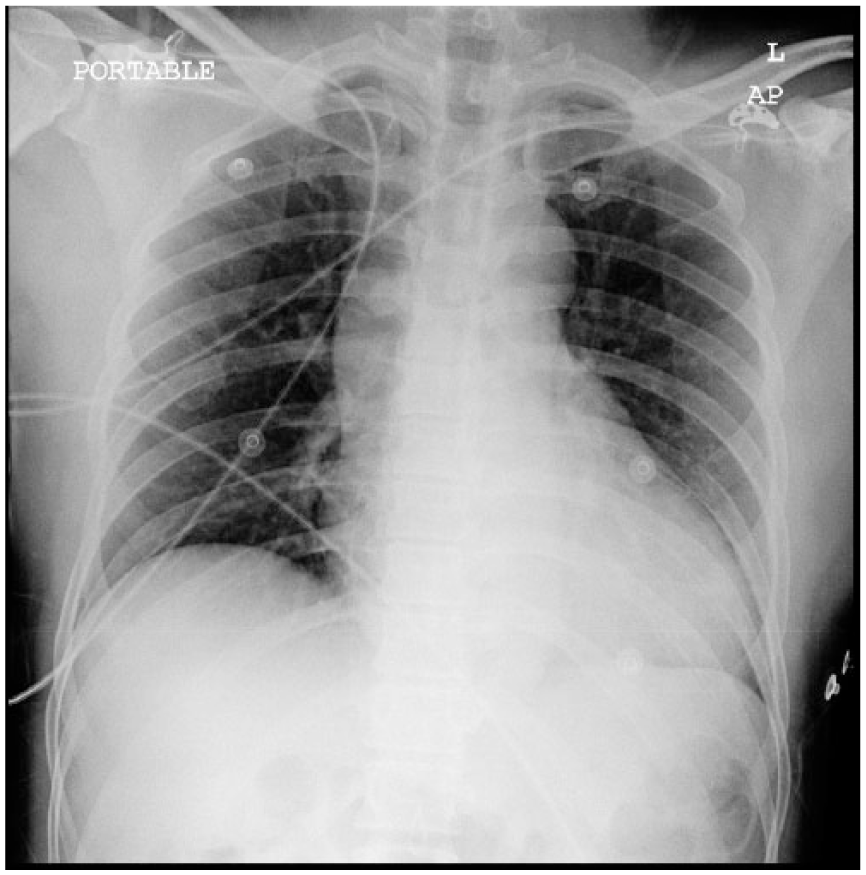
Anteroposterior (AP) view of portable chest radiograph showed a mediastinum width of 9.2 cm.
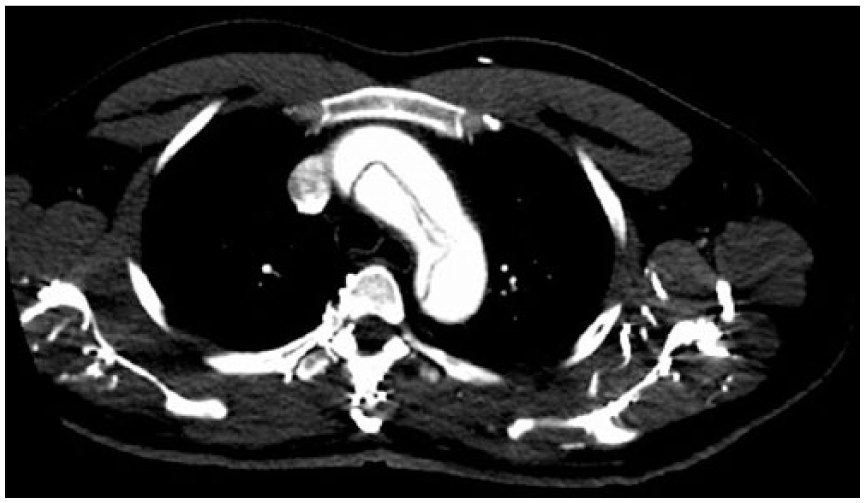
CT angiography showed aortic dissection involving the aortic arch.

CT angiogram showing dissecting lumen of ascending and descending aorta.
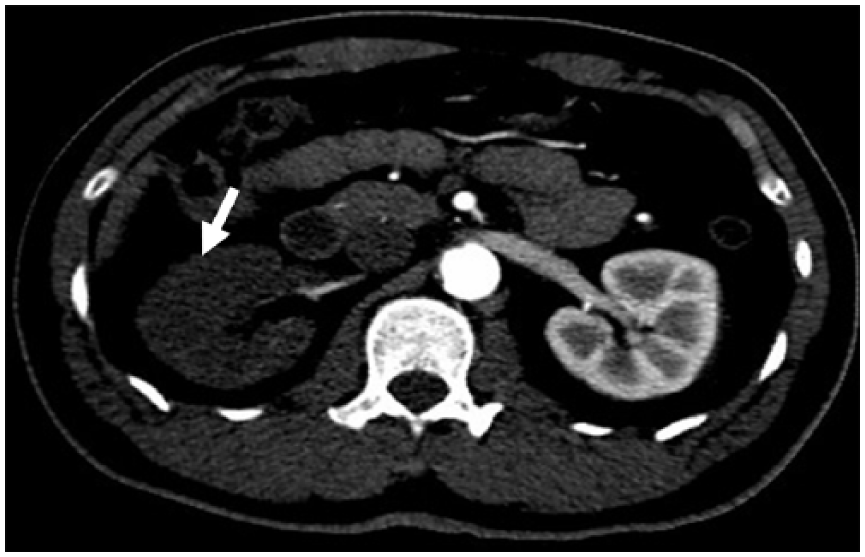
CT angiogram showing right kidney (white arrow) with no contrast in the right renal collecting system suggestive of malperfusion to it.
The patient was reviewed by neuro-medical and surgical team. Initial diagnosis was acute right lower limb ischemia. The patient was immediately scheduled for an emergency embolectomy and findings noted presence of small thrombus. However, the procedure only improved the flow of the femoral artery but not popliteal artery. He was then subjected to computed tomogram (CT) thorax angiography which surprisingly revealed extensive aortic dissection involving aortic root until the abdominal aortic bifurcation with superior extension to all aortic arch branches, compression of superior vena cava and left brachiocephalic vein by the dilated aortic root and right renal ischemia from a thrombus at true lumen (Stanford type A). Patient initially refused for any operative procedure, however, agreed for Bentall procedure after 3 days. Unfortunately, patient deteriorated intra-operatively and succumbed 1 h after procedure.
Discussion
Red flag of aortic dissection for this patient was the brief episode of syncope. He had predominant neurological symptoms without any pain which are observed in one-third of patients with type A aortic dissection. 3 It is caused by dissection or occlusion of aortic-side branches supplying the brain, spinal cord or peripheral nerves and symptoms appear shortly after the onset of dissection. Tsai et al. in 2009 noted that 33.9% of patients with painless aortic dissection presented with history of syncope, while Imamura et al. in 2011 noted a 25% association between transient losses of consciousness with painless aortic dissection.2,4 Occlusion of aortic bifurcation, iliac or femoral arteries and subclavian artery may result in peripheral ischemic neuropathy, pulse deficit and severe cases as paralysis, which was occurring in this patient. Lower extremity pulse deficit in the absence of peripheral vascular disease is commonly associated with malperfusion syndrome of aortic dissection. It is usually found in approximately half of patients with thoraco-abdominal or aortic arch involvement. 5
Malperfusion is recognized as second most common lethal complication of acute aortic dissection after rupture, and it is defined as loss of blood supply to arterial branches due to obstruction caused by the dissection. 6 Dissection ensues after a tear in the intimal layer of vessel creating a space within the plane of the medial layer which is known as false lumen. The hydrodynamic gradient balance between true and false lumen will then influence the progress of dissection to antegrade or retrograde. 7 The end of false lumen is often found at the ostia of aortic branch which may cause protrusion of intimal flap into the ostium causing thrombosis leading to a malperfusion of the limb and kidney as seen in this patient. 8 The distribution of pain, the level of neurology and pulse deficits will assist in determining the dissection level.
The broad spectrum clinical features post challenges in recognizing aortic dissection, and it may mimic other conditions that are more prevalent. Early diagnosis and distinguishing the extent of the dissection is essential as the fatality risk is high. It is fundamental to differentiate acute lower limb ischemia arising from embolism or thrombosis from lower limb malperfusion syndrome of aortic dissection as the treatment pathway differs. Collective findings from history, physical examination and laboratory results in this patient were sufficient to raise suspicion of malperfusion syndrome. High lactate level with metabolic acidosis, deranged liver function and abnormal renal profile are among the indicators for end-organ malperfusion. 6 Aortic dissection and its complications are normally diagnosed with computed tomography angiography (CTA). It is reported that radiological involvement of aortic branches is commonly seen in patients with acute limb ischemia, and both mesenteric and renal malperfusion are similarly associated with acute limb ischemia. 9 Presence of malperfusion syndrome in aortic dissection confers bad prognosis, and long-term survival was noted to be significantly lower (45.4%) than those without organ malperfusion (70.2%). 10
In retrospect, non-correlation between several features in our patients warrants suspicion of aortic dissection and presence of malperfusion syndrome. An earlier imaging evaluation could have been beneficial for a prompt diagnosis. Initial misdiagnosis is seen in 60% of cases. 6 Patients without pain of any type are typically not diagnosed or treated early. In a review done by Harris et al. using International Registry of Acute Aortic Dissection (IRAD) published in 2011 observes that pain characteristic had significant impact on the time to surgery. 11 Therefore, those with painless aortic dissection have higher risk of misdiagnosis and delay in treatment. To date there are no exact guidelines outlining management of such cases. Recognizing aortic dissection in patient presented atypically has proven to be particularly challenging, in which having high clinical suspicion and intuitiveness is imperative for clinician.
Conclusion
Aortic dissection presented with neurological symptoms is rare and requires high level of suspicion, especially in cases with unusual presentation. The pitfall in this case study is the delay in diagnosing aortic dissection and recognizing malperfusion syndrome due to its atypical symptoms. Early suspicion and prompt diagnostic imaging would have been essential for prompt differentiation of diagnosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymised patient information to be published in this article.