
Abstract
Introduction:
Tracheal intubation using video laryngoscopes has been a better approach for trauma patients requiring cervical immobilisation. The aim of this study was to compare the time to successful intubation by novice intubators using three types of intubation stylets with the new McGrath MAC video laryngoscope in a manikin model.
Methods:
This was a randomised crossover manikin study. The participants performed tracheal intubations using three intubation stylets (arcuate shape malleable stylet, McGrath MAC-shaped malleable stylet and McGrath MAC-shaped rigid stylet) in a difficult airway model with cervical immobilisation. The order of the stylets was randomised. The primary outcome was the time to successful intubation. The secondary outcomes were the overall success rates, incidence of dental trauma and ease of intubation. All intubation attempts were assessed by trained assistants. The data were analysed using a multilevel model followed by Tukey’s post hoc test.
Results:
A total of 68 nurses participated in this study. The time to successful intubation of the McGrath MAC-shaped malleable stylet was significantly shorter than that of the arcuate shape malleable stylet (24.5 (18.0–51.0) s vs 31.5 (21.0–89.0) s, p = 0.005). The overall success rate of the McGrath MAC-shaped malleable stylet was also higher than that of the arcuate shape malleable stylet (p = 0.047). The participants indicated that intubation was easier using the McGrath MAC-shaped malleable stylet compared with the other stylets.
Conclusion:
The McGrath MAC-shaped malleable stylet, when used by novice intubators, may be an optimal stylet shape for tracheal intubation using the McGrath MAC in cervical immobilisation.
Introduction
In severely injured patients, the cervical spine must be protected by in-line immobilisation during airway management. 1 If orotracheal intubation is required, then manual in-line stabilisation is recommended to facilitate tracheal intubation to secure a space for tongue displacement into the submandibular space. 2 However, even manual in-line stabilisation can make alignment of the oral, pharyngeal and laryngeal axes difficult, resulting in a poor direct laryngoscopic view and prolonging the intubation time.3,4
Video laryngoscopes, which do not require a direct line of sight, generally provide a better laryngeal view. They are easy to use and have a high success rate and short tracheal intubation time in patients with predicted difficult airways. 5 Thus, the use of video laryngoscopes is recommended as a first-line choice when a difficult laryngoscopy is anticipated. 6 Successful use of video laryngoscopy is increasing for airway management of patients with trauma in the emergency department (ED).7–9 Some researchers argue that the use of video laryngoscope is the best approach for tracheal intubation in these situations. 10
If particular video laryngoscopes are used, then a specific stylet is recommended for tracheal intubation.11,12 Although a stylet is not routinely used for tracheal intubation, particularly when using the video laryngoscope with the Macintosh type blade, 13 it often facilitates tracheal intubation in patients with cervical immobilisation. 14 The McGrath MAC® video laryngoscope (McGrath MAC) (Aircraft Medical, Edinburgh, UK) has a conventional Macintosh type blade and demonstrates a good intubation profile. 15 However, no studies have investigated the most effective stylet for use with the McGrath MAC during tracheal intubation in patients with trauma.
The aim of this study was to compare the time to successful intubation (TTSI) using three types of stylets in simulated cervical immobilisation for tracheal intubation with the McGrath MAC. The types of stylet included the malleable stylet (Malleable Arcuate) with a bow shape, which is consistent with the shape of commonly used tracheal tubes; the malleable stylet (Malleable MAC), which is shaped similarly to the blade of the McGrath MAC; and the rigid stylet, which was created by the researchers for this study and is configured similar to the distal McGrath MAC and is quite stiff (Rigid MAC).
Methods
Study design and setting
This was a randomised crossover manikin study. Based on the random sequence of the intubation stylet (Malleable Arcuate vs Malleable MAC vs Rigid MAC), each stylet was assigned to all participants (Figure 1).
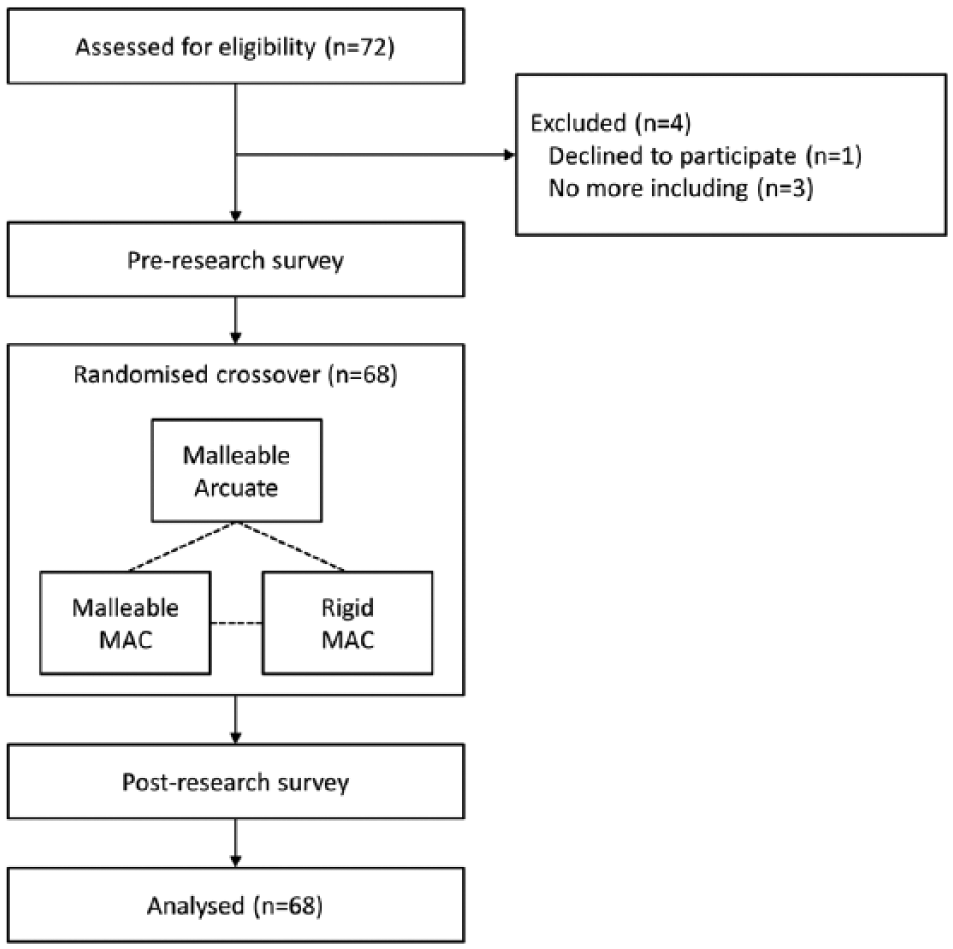
Flow diagram of the study.
This study was performed in the clinical skill laboratories of a 600-bed teaching hospital in South Korea. The manikins (Laerdal Airway Management Trainer; Laerdal Medical, Stavanger, Norway) were placed on hospital beds in the clinical skill laboratory along with the McGrath MAC with a size 4 blade, tracheal tube with a 7.5-mm internal diameter and the three different intubating stylets. The Institutional Review Board of The Catholic University Bucheon St. Mary’s Hospital approved this study (HC12OOSI0099).
Study participants
Among the nurses who participated in the 4-h emergency airway management training for nurses, we enrolled participants who had been working at an ED or in intensive care units and had been involved in emergency tracheal intubation as an assistant. The training programme included lectures on upper airway anatomy, a first pass success strategy for tracheal intubation and post-intubation management, and an exercise of bag valve mask ventilation and tracheal intubation. Those who had performed intubations on patients more than 10 times or wished not to participate in the study were excluded. Before the study, we provided an overall description of the study and obtained written informed consent from those who volunteered to participate in the study.
Study protocol
After training, the participants listened to the instructor’s explanation of the McGrath MAC and observed a live demonstration performed by the instructor. Subsequently, prior to initiating the study, all participants practised laryngoscopy using the McGrath MAC to become familiar with the device, but they were not allowed to insert the tracheal tube into the trachea of the manikin.
A rigid neck collar was applied to the manikin to reproduce cervical immobilisation, which was confirmed by three researchers to be Cormack–Lehane grade III or IV. The participants were instructed not to remove the neck collar and were asked to perform video-assisted tracheal intubation three times using the McGrath MAC with different stylets. The stylets were each used once by the participants for tracheal intubation (Figure 2).
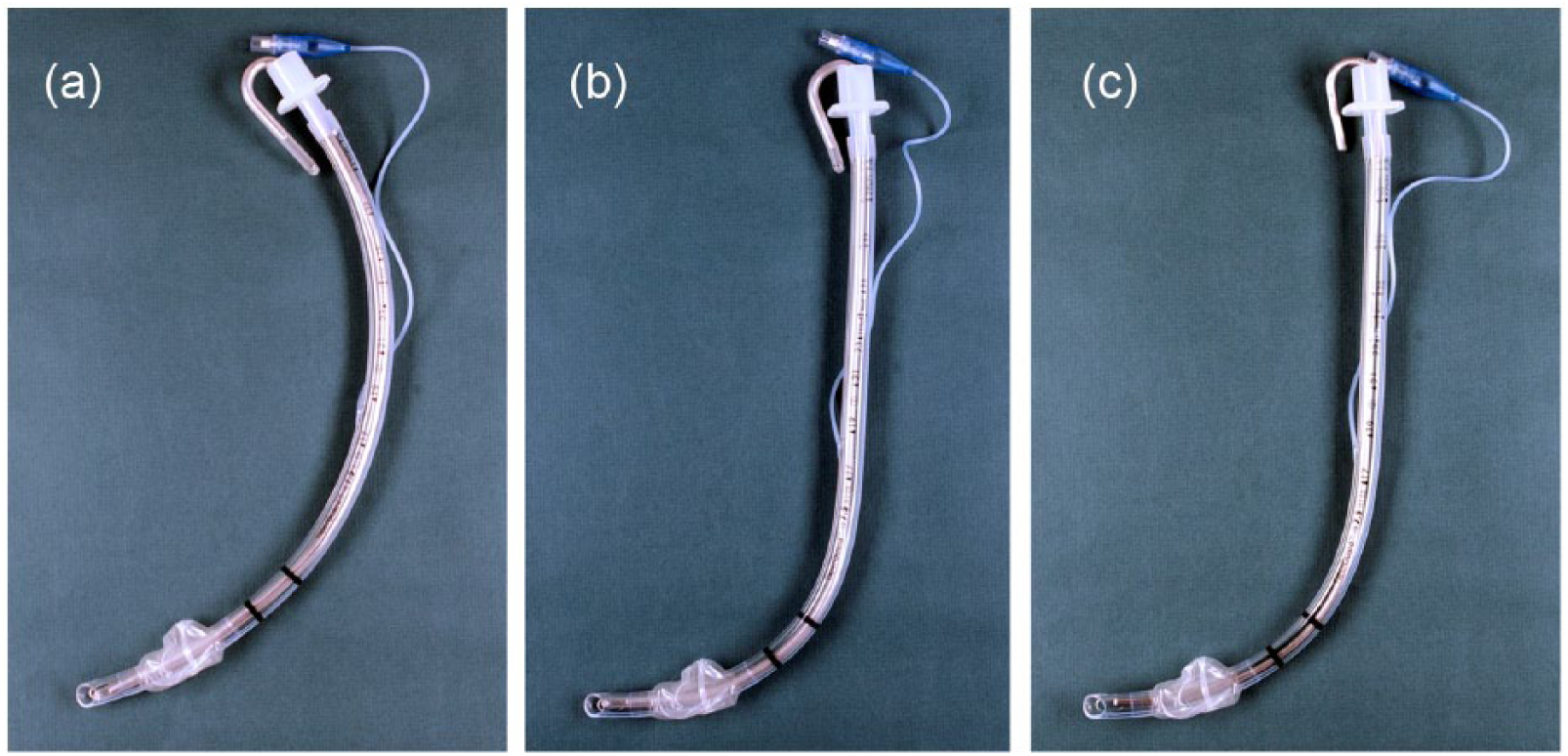
The three types of intubation stylets inserted in the tracheal tube: (a) Arcuate shape malleable stylet, (b) McGrath MAC-shaped malleable stylet and (c) McGrath MAC-shaped rigid stylet.
The order of stylet use was assigned randomly. A statistician who did not participate in the study created a random code for the sequence of stylet use and generated symbolised lots based on that code. The participants selected a lot from an opaque document envelope and then performed tracheal intubations according to the pre-determined random sequence.
Standardised assistants who were blinded to the purpose of study altered the malleable stylet to a specified shape, prepared three types of stylet-tracheal tubes and applied lubricant before intubation. After each intubation attempt, the assistants removed the stylet and performed ventilation using a bag valve mask. Both the participants and the assistants were blinded to the stylet sequences.
Outcome measures
The primary outcome was the TTSI with three types of intubating stylets for tracheal intubation with the McGrath MAC. The secondary outcomes were overall success rate, incidence of dental trauma and evaluation of the intubation stylets by the participants. TTSI refers to the time from when the laryngoscope tip passed the mouth of the manikin to when the artificial lung of the manikin was inflated by squeezing the bag valve mask. The overall success rate refers to intubation success within 300 s, regardless of oesophageal intubation, and the incidence of dental trauma was investigated by counting the frequency of dental click sounds of the manikin. A blinded and trained observer measured TTSI using a stop watch and investigated the overall success rate and incidence of dental trauma.
We collected data for the baseline characteristics of the participants, including sex, age, workplace, service years and experience in tracheal intubation before the study. The participants evaluated the intubation stylets after the study by completing questionnaires.
We used a crossover design to compare the three types of intubation stylets. We performed a priori sample size estimation and assumed a mean and standard deviation of the difference in the time to intubation between intubation stylets of 20.0 and 21.1 s, respectively, based on a study of the McGrath series 5 (Aircraft Medical, Edinburgh, UK). 16 In this estimation, a crossover design with α = 0.0167 and a statistical power of 80% would require 56 subjects. Thus, based on a 20% dropout rate, 68 test subjects were enrolled in this study.
Data analysis
The baseline characteristics of the participants are presented as frequencies and proportions for categorical variables and as medians (interquartile range (IQR)) for continuous variables based on the normality of the data distribution. To compare the TTSI and the incidence of dental trauma, we used the general linear model analysis of variances (GLM ANOVA) with the post hoc Tukey–Kramer method. To compare overall success rates, we used the chi-square test with the post hoc Bonferroni method. All hypothesis testing was two-sided with a significance level of 0.05. All statistical analyses were performed using SAS software (version 9.12, SAS Institute, Inc., Cary, NC, USA).
Results
A total of 68 novice intubators participated in this study, and all were nurses working in the ED or intensive care units who had been assisting with tracheal intubation (Table 1). In all, 30 nurses had experience performing tracheal intubation in clinical situations.
Baseline characteristics of the participants.
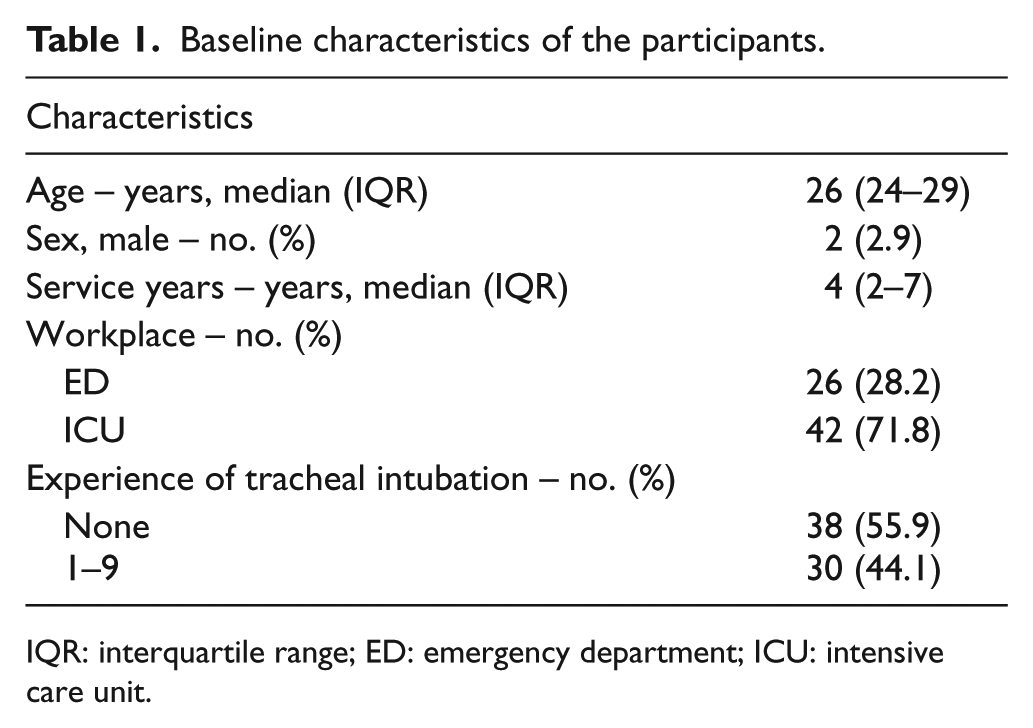
IQR: interquartile range; ED: emergency department; ICU: intensive care unit.
There was no carryover effect, but there was a group effect between groups for TTSI (p = 0.007) (Table 2). In the post hoc analysis, the TTSI with the Malleable MAC was shorter than that with the Malleable Arcuate (p = 0.005). The TTSI with the Rigid MAC did not differ from those with the Malleable Arcuate and Malleable MAC (p = 0.14 and 0.39, respectively). There was no carryover effect, but there was a group effect between groups for the overall success rate (p = 0.046) (Table 2). In the post hoc analysis, the overall success rate of tracheal intubation was higher with the Malleable MAC than with the Malleable Arcuate (p = 0.047). The overall success rate of the Rigid MAC did not differ from those with the Malleable Arcuate and Malleable MAC (p = 0.19 and 0.38, respectively). The incidence of dental trauma during tracheal intubation did not differ between stylets. When rating the ease of intubation, the largest part of the participants preferred the Malleable MAC (27 participants (39.7%)). The Malleable Arcuate was found by the largest group of participants to give the most difficult intubation (30 participants (44.1%)) (Table 3).
End points of tracheal intubation using the McGrath MAC video laryngoscope with three types of intubation stylets.
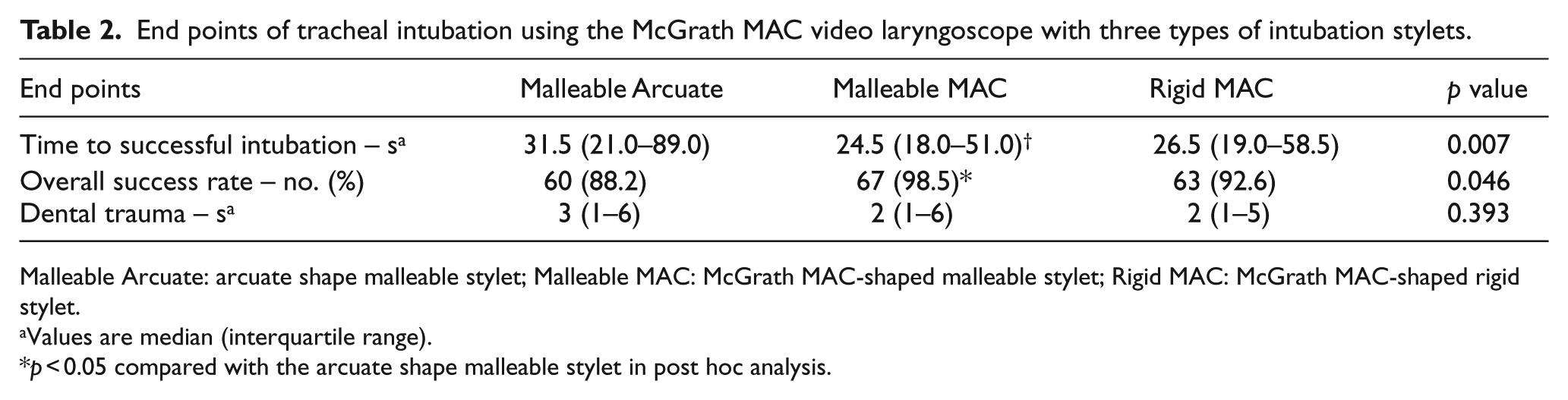
Malleable Arcuate: arcuate shape malleable stylet; Malleable MAC: McGrath MAC-shaped malleable stylet; Rigid MAC: McGrath MAC-shaped rigid stylet.
Values are median (interquartile range).
p < 0.05 compared with the arcuate shape malleable stylet in post hoc analysis.
Evaluation of the intubation stylets by the participants after all tracheal intubations.

Malleable Arcuate: arcuate shape malleable stylet; Malleable MAC: McGrath MAC-shaped malleable stylet; Rigid MAC: McGrath MAC-shaped rigid stylet.
Discussion
In this study, we compared three types of stylets for tracheal intubation with the McGrath MAC in simulated cervical immobilisation (Malleable Arcuate vs Malleable MAC vs Rigid MAC). We found that the Malleable MAC had the best performance characteristics when used by novice intubators. To the best of our knowledge, this is the first study to investigate the optimal stylet shape for tracheal intubation with the McGrath MAC in simulated cervical immobilisation.
Anterior angulated stylets such as the Malleable MAC have been reported in studies investigating video laryngoscopes with an angulated blade, such as the Glide video laryngoscope (Verathon Inc., Bothell, WA, USA) or McGrath series 5. Intubation was easily achieved using an anterior angulated stylet,11,12,17 and the use of video laryngoscopes with a stylet has shown high success rates compared with the Macintosh laryngoscope in predicted difficult or failed airways.18,19 These video laryngoscopes usually present an adequate glottic view,11,17 but improved glottic visualisation does not always guarantee successful tracheal intubation. Because the distal blade is angulated anteriorly, insertion of the tracheal tube into the larynx can be difficult. 20 Thus, the use of an angulated stylet is recommended for tracheal intubation using video laryngoscopes with an angulated blade.21,22
According to the manufacturer, the McGrath MAC, which has a Macintosh type blade, offers the benefit of both direct laryngoscopy and indirect video-assisted laryngoscopy. Video-assisted laryngoscopy using the McGrath MAC also provides an improved view of the glottis and a high success rate.23,24 Although the need for a stylet for tracheal intubation of a normal airway is reduced using video laryngoscopes with the Macintosh type blade,25,26 the J-shaped stylet could reduce intubation challenges associated with difficult airway situations such as a manual in-line stabilisation. 14 McElwain et al. 26 reported that the hockey-stick stylet with the C-MAC video laryngoscope (Karl Storz, Tuttlingen, Germany), which also has a Macintosh type blade, demonstrated the best performance in simulated difficult tracheal intubation scenarios. Compared with the non-angulated strategy, which does not change the shape of the tracheal tube, the angulated strategy of the distal tracheal tube shortened the tracheal intubation time and improved the intubation success rate. In this study, the McGrath MAC-shaped stylet had a shorter TTSI and a higher success rate than the arcuate shape stylet, which maintained the original shape of the tracheal tube. Considering that video-assisted laryngoscopy does not require alignment of the oral, pharyngeal and laryngeal axes, it may be difficult, even with the Macintosh type blade, to direct the tracheal tube through the opening of the glottis without a stylet. Because difficult airway situations such as cervical immobilisation cause this manifestation to become prominent, it may be helpful to use an angulated stylet with a similar shape to the blade.
In this study, there were no statistical differences in outcomes according to the rigidity observed with the Malleable MAC and the Rigid MAC. Previous reports examining video laryngoscopes with angulated blades have provided some conflicting results. In a study using a GlideScope video laryngoscope in normal airways in the operating room, there were no differences in TTSI between the GlideScope®-specific rigid stylet (Verathon Medical Inc., Bothell, WA, USA) and the malleable stylet, 27 whereas another study showed a tendency towards a shorter TTSI with the malleable stylet. 28 However, in a study using the GlideScope video laryngoscope in various groups of ED patients among whom approximately 50% had a cervical collar, the GlideScope-specific rigid stylet had a higher first attempt and overall success rate compared with the malleable stylet. 29 In this study, the malleable stylet showed the best performance. Additionally, the participants considered the malleable stylet to be more useful for intubation compared with the rigid stylet. This difference could be due to the ease of advancing the tracheal tube that is in contact with the tracheal wall into the trachea or the ease of stylet withdrawal before advancement. Additional studies are needed to determine the appropriate rigidity of the stylet for tracheal intubation using video laryngoscopy with the Macintosh type blade.
This study has some limitations. First, this was a manikin study, which does not provide a perfect substitute for a human study. However, we measured the efficacy of three types of stylets during tracheal intubation using the McGrath MAC in simulated cervical immobilisation. Based on the potential harm to patients, a manikin study was considered to be appropriate as an initial study to determine the best stylet. Second, all participants were nurses. The participation of clinicians who perform the actual intubation would be ideal, but it was thought that novices with little exposure to McGrath MAC would be appropriate for identifying the advantages and efficacy of various stylets in McGrath MAC-utilised tracheal intubation. The nurses who participated in this study attended a 4-h airway management training course and practised tracheal intubation. Although actual clinical experience was lacking, based on this training course, they were considered to have acquired basic knowledge and the skills required for tracheal intubation. Thus, this condition may reflect situations where junior emergency physicians make the first intubation attempt at teaching hospitals. 30 Third, we only simulated cervical immobilisation to investigate the proper shape of the intubation stylets for tracheal intubation with the McGrath MAC in severely injured patients. The results did not affirm that the Malleable MAC is always required for other situations, such as facial trauma and active oral bleeding. However, because the maintenance of cervical immobilisation without disruption of the neutral position during tracheal intubation in patients with multiple traumas is very important, it is regarded as a minimum condition to identify the usefulness of stylets in a trauma situation.
Conclusion
For tracheal intubation by novice intubators using the McGrath MAC, the Malleable MAC showed shorter TTSI and a higher overall success rate in a simulated difficult airway with cervical immobilisation. Intubation using the Malleable MAC was considered the easiest among the three types of stylets. Using a conventional malleable stylet that is McGrath MAC-shaped for tracheal intubation with a McGrath MAC video laryngoscope may be useful for difficult airway situations.
Footnotes
Acknowledgements
We thank Ae-Sook Choi, Jeong-Soon Ryu, Geom-Sook Kim and Hea-Sook Shim from the Nursing Department at Bucheon St. Mary Hospital for their assistance with the preparation of the research and outcome measures. We also thank Mi-Sun Park, Seung-Hee Jeong and Hyeon-Woo Yim in the Clinical Research Coordinating Centre at the Catholic Medical Centre for the statistical analysis and interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.