
Abstract
Study objective:
While some research has been done on Valsalva maneuvers in treating supraventricular tachycardia, there is no standardized algorithm on which technique has been the most effective for the termination of supraventricular tachycardias. In this study, we compare different Valsalva maneuver techniques in order to determine the exact technique needed for maximal vagal response.
Methods:
This was a repeated measures clinical study, which enlisted a sample of healthy adult volunteers. Participants performed four different Valsalva maneuver techniques (40 mm Hg—10 s, 40 mm Hg—15 s, 50 mm Hg—10 s, and 50 mm Hg—15 s) while lying in a supine position. The maneuvers were repeated three times. An electrocardiography printout was obtained during each trial, and heart rate differences between pre-maneuver and post-maneuver were measured.
Results:
Among the 97 volunteers who participated in the study, 7 were excluded because the target Valsalva maneuver pressures were not reached, and 1 volunteer was excluded due to T-wave inversion that developed after Valsalva maneuver. We enrolled 89 participants. There was no significant difference in the heart rate decrease among the four techniques. In addition, there was no difference between the vagal responses in terms of age, gender, and body mass index.
Conclusion:
This study shows that the four different Valsalva maneuver techniques were not superior to one another in terms of decreased heart rate.
Introduction
Background
Supraventricular tachycardia (SVT) is a general term used to define dysrhythmias, including atrioventricular reentrant tachycardia, atrioventricular nodal reentrant tachycardia, junctional tachycardia, atrial tachycardia, and atrial flutter with a heart rate over 100 beats per minute. 1 Stable patients with SVTs usually present with palpitations, shortness of breath, and dizziness. These symptoms are commonly uncomfortable for the patient. 1 The effective methods to terminate SVTs in these patients are vagal maneuvers and medical or electrical cardioversion. Due to the ease of application and the safe side effect profile, vagal maneuvers are the first line of treatment in SVT termination. 1 Valsalva maneuver (VM), carotid sinus massage, and diving reflex are commonly used vagal maneuver techniques. These techniques work by increasing the vagal tone and decreasing atrioventricular conduction. The end result is slowing of the heart rate and termination of SVTs. 2 If these maneuvers fail to convert the rhythm to sinus rhythm, medical and electrical cardioversion can be attempted. 1 For medical cardioversion, adenosine is commonly used, but has quite unpleasant side effects, including chest discomfort and flushing. 1 Taking the side effect profile of adenosine and electrical cardioversion into account, VM is a safe and non-invasive intervention, and therefore, the exact VM technique that gives the optimal vagal response should be investigated. 3
Many studies have evaluated the superiority of different vagal maneuvers. These studies showed that the VM was the most effective method of SVT termination among vagal maneuvers.4–7 VM consists of three components, which are patient’s posture, straining pressure, and straining duration.3,8,9 Different combinations of these components were tested in an attempt to provide maximum vagal (bradycardic) effect in some studies.7,9–11 Among these studies, a consensus was made that in the supine position, 40 mm Hg pressure strain for 15 s is the current standard of treatment.3,7,11 However, due to the lack of a gold standard VM technique,1,3 physicians either use different combinations of the three components or decide on a maneuver they are most comfortable using.10,12 Therefore, the success of VM’s cardioversion differs among studies.3,11 Due to the lack of a universally accepted, standardized VM, much research is being done to find the most effective VM technique.
The purpose of our study was to compare the standard technique of VM (supine posture, 40 mm Hg, 15 s) to different VM durations and pressure levels in the same posture, in order to find out which technique accomplishes the most effective vagal response.
Materials and methods
Study design (and setting/selection of participants)
We conducted a repeated measures study at Koç University Hospital’s tertiary care emergency department in Istanbul, Turkey, between June 2015 and November 2015. Our hospital’s institutional review board approved this study. Written informed consent was obtained from all volunteers before enrollment.
A convenience sample of healthy adult (aged ≥18 years) volunteers who work in our hospital were enrolled. The participants that were included had not consumed tobacco, caffeine, or alcohol for a minimum of 6 h prior to the investigation. All were self-reportedly healthy, with a sinus rhythm on the pre-maneuver electrocardiography (ECG).
Exclusion criteria were the presence of a chronic disease (cardiorespiratory disease), regular medication use, pregnancy, and history of major intracranial and thoracoabdominal surgery. We also excluded participants in the testing period who could not achieve the pressure needed to perform the VM (40 and/or 50 mm Hg). Volunteers who did not have flushing and/or visible jugular venous distention were warned not to use intraoral pressure only (closed glottis). If they were not able to correctly apply the maneuver and only intraoral pressure was used after being warned, these patients were also excluded from the study.
Methods of measurements
Our investigation was conducted in the observation room of the emergency department with a mean ambient temperature of 23.5°C. Four attending emergency medicine physicians were assigned as investigators. After informed consent was given, we collected data on participant demographics, including age, sex, height, weight, and body mass index (BMI).
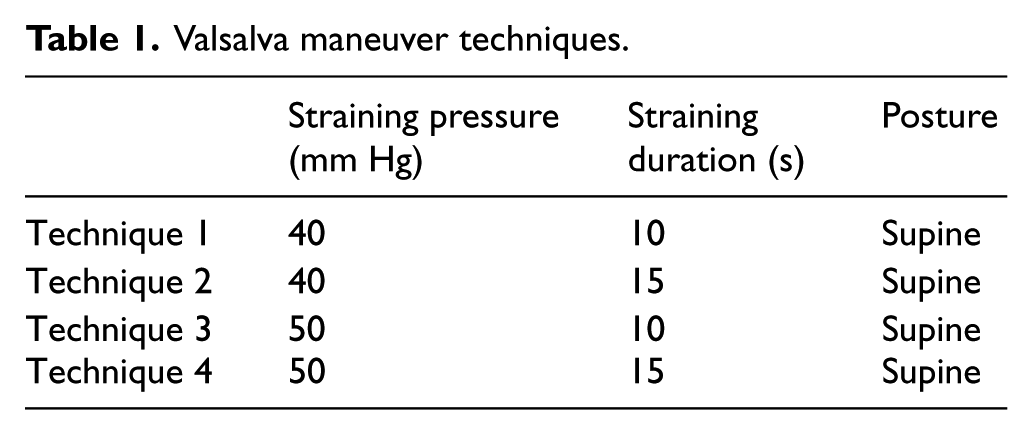
Each participant performed four different VM techniques (Table 1) three times under the supervision of two attending emergency physicians who were blinded to calculating R-R interval. Four techniques were written on paper and placed into four closed envelopes, which were then randomly chosen by nurses who were in charge of care. Thus, for each participant, 12 trials were attempted in one session. We ensured 3 min of resting time between maneuvers to restore cardiovascular functions, blood pressures, and intrathoracic pressures. 9 The desired pressure was achieved (40 or 50 mm Hg) in 1–3 s, following a deep inspiration for 1–2 s, with a straining duration of 10 or 15 s. 13
Valsalva maneuver techniques.
Prior to the test, the participants lay in a supine position for 5 min. During this period, the study protocol was explained to the volunteers by the investigator, and their blood pressure was measured. All participants were in a supine position during the test and were monitored with a defibrillator (Nihon Kohden, TEC-5531K). To obtain the particular pressure values in VM, we used a sphygmomanometer (Riester, big ben®, wall design) with a single use, disposable device for blowing.
Participants were able to see the sphygmomanometer monitor. After a couple of minutes of resting, we started to record a continuous ECG (Lead II, 25 mm/s) and instructed the participant to start the maneuver whenever they felt ready. During each trial, we marked the start and the end of each strain on the ECG printout for later analysis. ECG recording continued for 20 s after the strain was completed. Participants were requested to abstain from speaking or moving during the ECG recording.
After the VM test session was completed, all the intervals were calculated by two attending emergency physicians blinded to testing phase. The pre-maneuver R-R interval was calculated using the mean of 10 consecutive R-R intervals before VM. The longest R-R interval within 20 s of termination of VM was considered as the post-maneuver R-R interval. Additionally, pre-maneuver and post-maneuver R-R interval differences for each VM were calculated with 95% confidence interval (CI). Thus, we calculated heart rate changes and bradycardic effects for each VM. In pre-maneuver studies, we had concluded that the effects of the vagal response could be evident up to 20 s after VM, so recording time was continued for a minimum of 20 s after VM.
Volunteers were investigated for headache, dizziness, and any other complaint between trials and after the testing.
All statistical computations were generated by an attending emergency physician who did not participate in the testing and calculating process, using IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp., Armonk, NY, USA, Released 2013). The chi-square test and logistic regression analysis were used for categorical variables in the comparisons between groups. The paired-samples t-test and repeated measures analysis of variance (ANOVA) tests were performed for numerical variables that were normally distributed, whereas the Mann–Whitney U-test, Wilcoxon sign test, and Friedman test were used for numerical variables that were not normally distributed.
Primary data analysis
We calculated our sample size with G*Power 3.1.6 software. Assuming the mean heart rate changes to be clinically inconsequential during each pre-maneuver phase, with an α of 0.05 and β of 0.05 (95% power), 87 participants were required for analysis.
Results
During the entire study period, 97 volunteers participated in the study. Seven female participants were excluded since they were unable to achieve the desired pressure during VM (4/7 had 40 mm Hg and 3/7 had 50 mm Hg). One participant was excluded from the study since T-wave inversion occurred at his second VM trial. T-wave inversion was detected 5 s after the strain finished (Figure 1) for Technique 2 (40 mm Hg—15 s), and normal sinus rhythm was spontaneously achieved 30 s later. He had no complaints or unstable vital signs during and after test. Cardiology consultation was ordered for the patient and was evaluated with selective myocardial perfusion scintigraphy, which showed normal results.
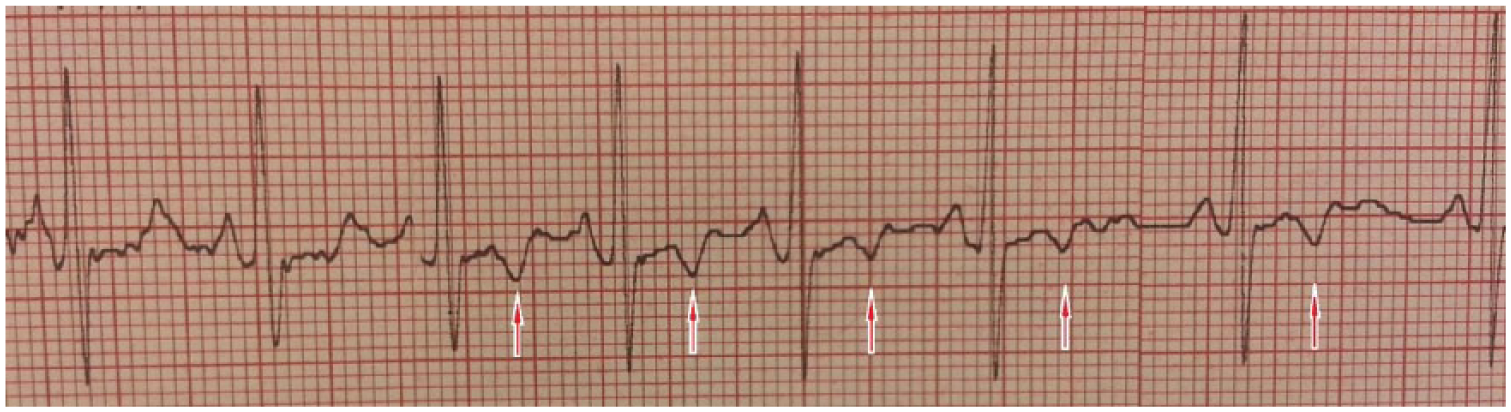
Development of T-wave inversion (T inversions are shown with red arrow).
A total of 89 participants, 57% female (n = 51), were enrolled. Baseline characteristics of participants are shown in Table 2.
Baseline characteristics of participants.
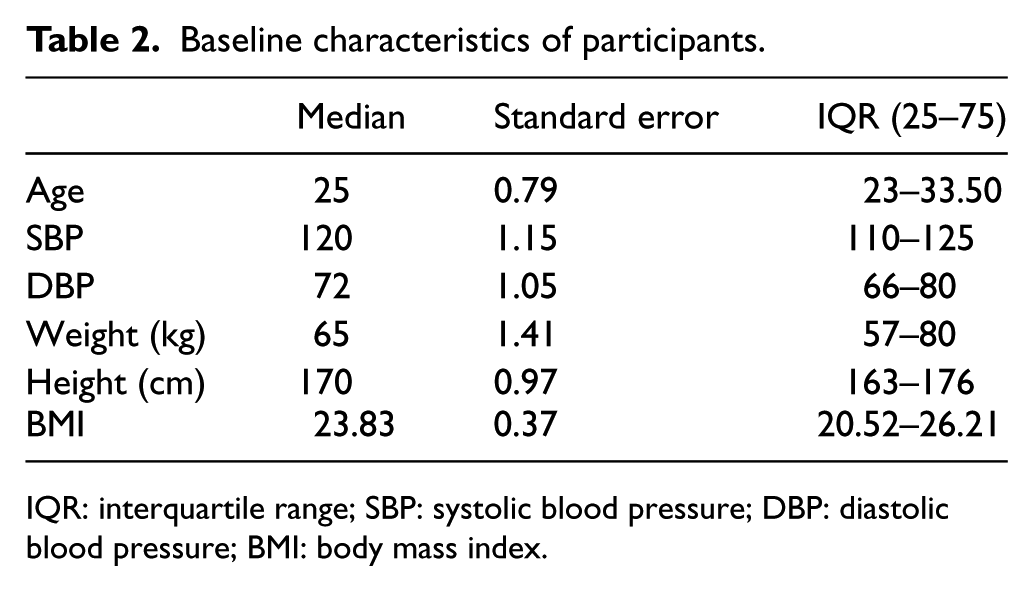
IQR: interquartile range; SBP: systolic blood pressure; DBP: diastolic blood pressure; BMI: body mass index.
The statistical analysis showed that the pre-maneuver heart rates of the participants were normally distributed. There were also no significant differences between the pre-maneuver heart rates and the heart rates in between trials for participants (p = 0.72) (Table 3).
Statistical analysis results of pre-maneuver and post-maneuver heart rate values.
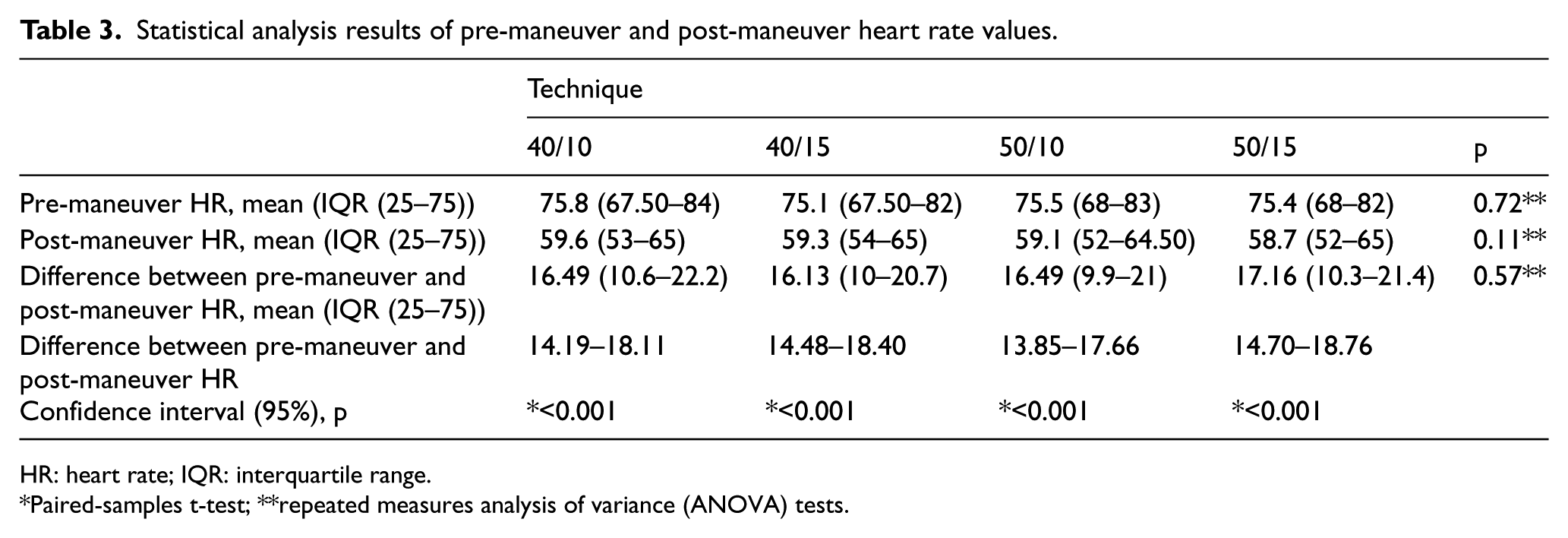
HR: heart rate; IQR: interquartile range.
Paired-samples t-test; **repeated measures analysis of variance (ANOVA) tests.
Statistically significant differences were identified in the pre-maneuver and post-maneuver heart rates for different VM pressures and durations (Table 3).
It was observed that all the techniques had reductions in heart rates that were statistically significant. When the techniques were compared with each other, it was shown that none of the methods were statistically superior to each other in terms of lowering heart rate (p = 0.57) (Table 3).
When comparing the effects of sex, age (19–29, 30–39, 40–49, 50–55 years), and BMI on pre-maneuver and post-maneuver heart rates, no statistically significant correlation was observed (Table 4).
p-values for pre-maneuver and post-maneuver heart rates when comparing sex, age, and BMI.
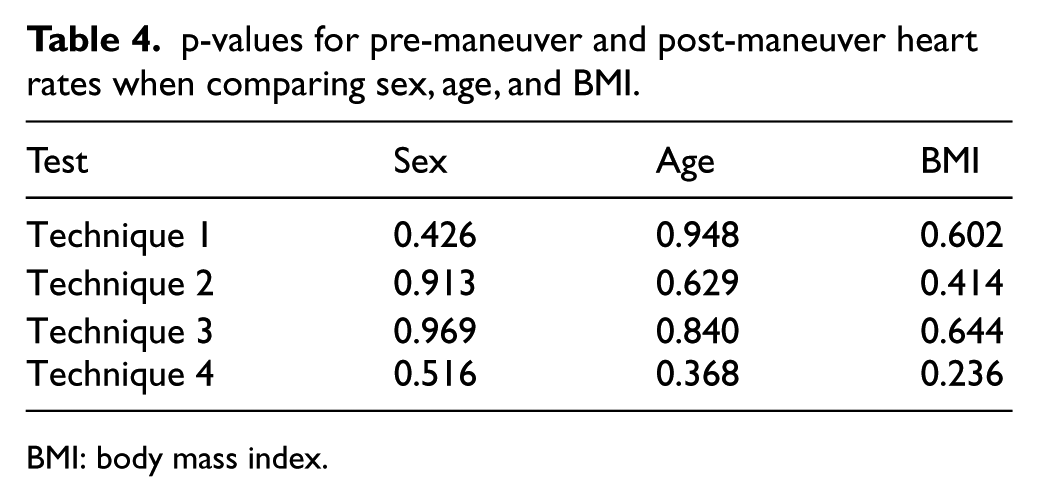
BMI: body mass index.
When participants were queried if they had any complaints during strain phase, five (5.6%) participants felt dizzy, three (3.3%) participants had a headache, three (3.3%) participants reported “seeing spots,” and one (1.1%) participant’s headache continued for a couple of minutes after the strain phase, then resolved spontaneously. There was no difference among different techniques in terms of side effects. The side effects were not severe enough to terminate the test.
Discussion
The bradycardic effect of VM was first reported by Weber in 1851. 13 From that time on, VM has been used with the aim of termination of stable SVTs. There are still ongoing studies on the optimal VM variables, including strain pressure, strain duration, and posture.
Although there are many studies recommending VM to be performed in the supine position,3–9,12 there have been a few studies that recommend otherwise. Walker and Cutting 10 claimed that Trendelenburg posture achieves a higher number of successfully terminated SVTs; however, the “standard technique” that they compared their studies consisted of many different postures and durations. Appelboam et al. conducted a randomized controlled study where they accepted the semi-recumbent position as their standard VM position. They compared applying a VM in their standard position versus placing the patient in a supine position after applying a VM in the standard position and found that postural modification had a higher success rate of terminating SVTs. 11 In addition to the studies that claim supine position is more effective in terminating SVTs, the 2015 Guideline for the Management of Adult Patients with SVT also suggests that VM should be performed with the patient in the supine position. 1 Therefore, our study was conducted with patients lying in the supine position.
In the literature search, we observed that there was paucity of research in comparing the effectiveness of VMs in different pressures and durations. A study conducted by Denq et al. 8 required at least a 30-mm Hg pressure and a 10-s duration for their volunteers to be included in their study. Walker and Cutting 10 have used pressures of at least 40 mm Hg. Looga 13 suggested that there is a positive correlation between strain pressure and post-maneuver bradycardia. In light of these data, we used 40 and 50 mm Hg for effective VM pressure values with a straining phase of 10–15 s.
In their case series, Un et al. 14 has reported termination of SVTs by quickly changing the patient’s positions from erect to supine and letting them breathe slowly and deeply afterwards.
In our study, we observed that a patient developed T-wave inversion without any complaints or abnormal clinical findings after the maneuver was finished. Feldman et al. 15 and Hosseini and Jamshir 16 has reported that a decrease in the amplitude of the T-wave is possible during a VM, but no studies showed a development of T-wave inversion during a VM.
Since we did not observe superiority between the techniques measured in this study (Figure 1), we can conclude that a VM of 40 mm Hg for 10 s will be enough for maximal bradycardic response. Studies have shown that using a 10-mL syringe, patients in a pre-hospital or hospital setting, or patients who were educated on using a syringe for VM, can easily achieve a 40-mm Hg pressure.7,11
We observed that age, sex, or BMI did not have statistically significant effects on bradycardic response. Hence, we can conclude that position and duration of a VM does not need to be modified based on these factors.
Seven participants were not able to achieve the desirable pressures. When analyzing studies regarding VM done on healthy volunteers or patients with pathologies, we did not encounter this scenario. In addition, the volunteers need to be fully cooperative when the physician is giving directions. For patients that are not able to reach the desired pressures, we recommend that they reach the highest pressure they can during the maneuver or to try a different vagal maneuver.
During the trials, 12 patients reported either dizziness, headache, or seeing “white spots.” These symptoms resolved spontaneously during rest, and the tests were continued.
Limitations
The most important limitation of this study is that the trials were done on healthy individuals, with normal sinus rhythms. We also observed an increase in the pre-maneuver heart rate for patients who experienced the 40 mm Hg trial or the 10-s trial and were then told that they had to perform a 50-mm Hg and a 15-s trial. This was due to the patients being concerned that the trials might be too difficult and therefore induced anxiety. However, these increases in heart rate were not enough to change the mean values in pre-maneuver heart rates and were therefore not taken into account. Our individuals were young, so this population was not completely representative of all patients who presented with SVTs.
Conclusion
This study shows that the four different vagal maneuvers (40 mm Hg for 10 and 15 s, 50 mm Hg for 10 and 15 s) done in the supine position were not superior to one another in terms of decreased heart rate. Because of failure to achieve the desired pressure, applying VM in 40 mm Hg for 10 s may be easier for patients.
For patients with chronic disease, different pressures and durations may need to be applied in order to terminate SVTs. Additional studies need to be done for further evaluation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was not necessary because no patient data has been included in the manuscript.