
Abstract
Background:
This study aims to determine the relationship between troponin levels and 30- and 90-day mortality rates in patients who applied to emergency service with paroxysmal supraventricular tachycardia.
Materials and methods:
The data of our study were obtained from the retrospective screening of the files of 321 patients who applied to the emergency department between 1 January 2015 and 31 December 2016 with International Classification of Diseases diagnosis with I47.1 (supraventricular tachycardia). Unstable patients, patients under 18 years, and patients with comorbidities that could increase troponin levels did not participate in the study. A total of 159 patients diagnosed with paroxysmal supraventricular tachycardia were included in the study. These patients’ files were examined, and their examination and anamnesis information at the time of admission to hospital, demographic characteristics, and applied treatments were analyzed. The 30- and 90-day mortality rates of the patients were examined.
Results:
The study was carried out with 159 patients. Troponin was positive in 25 (15.7%) cases, while it was negative in 134 (84.3%) cases. There was no significant difference between the two groups in terms of 30- and 90-day mortality rates. Coronary artery disease was found to be higher in patients with positive troponin than patients with negative troponin.
Conclusion:
No significant difference was found between patients with positive troponin values compared to patients with negative troponin values in terms of 30- and 90-day mortality rates. We believe that prospective observational studies or large-scale retrospective studies will better elucidate this issue.
Introduction
Supraventricular tachycardia (SVT) is a general term for all types of tachycardia originating above the ventricles in the atria or atrioventricular (AV) node. SVT is a clinical syndrome characterized by the presence of an abrupt onset of rapid tachycardia on a regular basis, in which QRS complex is less than 120 ms and atrial rate is between 120 and 250 beats/min. 1 There are two tachycardia types which are often referred to as paroxysmal supraventricular tachycardia (PSVT): atrioventricular nodal reentrant tachycardia (AVNRT), which occurs in the AV node, originating from the reentry ring, constituting 60% of the PSVTs, and the atrioventricular reentrant tachycardia (AVRT), which originates from the reentry ring and includes the AV bypass tract and constitutes 20% of the PSVTs.2,3
There are no recommendations for the follow-up of these patients in guidelines on the use of cardiac biomarkers in emergency services. Hs-troponin I level, which is a cardiac biomarker, is one of the requested analysis for the diagnosis of acute coronary syndrome. In addition, increased Hs-troponin I levels without myocardial ischemia are also used as a marker of poor prognosis. 4 The mechanism of myocardial damage seen in PSVT patients has not been fully explained. The most widely accepted theory is that coronary perfusion occurs during diastole, resulting in myocardial damage and increased troponin due to the failure of coronary perfusion during tachycardia. 5 Previous studies showed that patients with increased troponin values had normal coronary angiograms.6,7
This study aims to determine the relationship between troponin level and 30- and 90-day mortality rates in patients who applied to emergency service with PSVT.
Materials and methods
This study was conducted at Fatih Sultan Mehmet Education and Research Hospital, Istanbul, Turkey, with an annual patient load of 220,000. The data of our study were obtained from the retrospective screening of the files of patients who applied to the emergency department (ED) between 1 January 2015 and 31 December 2016 with International Classification of Diseases (ICD), 10th revision, diagnosis with I47.1 (SVT). Patients under 18 years of age, unstable patients (ischemic chest pain, altered mental status, acute pulmonary edema, and hypotension-systolic blood pressure <90 mm Hg), patients with comorbidities (stroke, kidney failure, etc.) that could increase troponin levels, and patients without PSVT as a result of electrocardiogram (ECG) evaluation did not participate in the study. As a result of the evaluation of these exclusion criteria, patients who were evaluated by emergency medicine specialists in our clinic and diagnosed with PSVT were included in our study. These patients’ files were screened, and their examination and anamnesis information, comorbid diseases at the time of admission to hospital, demographic characteristics, and applied treatments were examined. In this study, a 12-lead ECG device (SCHILLER CARDIOVIT AT-102 plus, Switzerland) that was used in the Emergency Medicine Clinic of our hospital was utilized. Abbott Architect brand Hs-troponin-I kit was used for the evaluation of patients’ serum Hs-troponin levels. In accordance with the values of the Hs-troponin Architect kit in the 2015 European Society of Cardiology NSTEMI Guidelines, the cut-off value was taken as 15.6 and 34.2 pg/mL for females and males, respectively. A sample of venous blood for hs-cTnI testing was taken at the time of ED presentation. Biomarkers were rechecked at 3 h in troponin test positive–patients. If the first measurement was within normal ranges for hs-cTnI, the patients were excluded from further sampling.
Patients were contacted via their phone numbers registered in the hospital registration system, and their complications or death status after discharge was inquired to determine the 30- and 90-day mortality rates of the patients. In cases that could not be reached by phone, the mortality status was investigated via the Internet-based national “Death Notification System.” The Human Investigation Committee of our institution reviewed and approved the study.
Statistical analysis
While evaluating the data obtained in this study, IBM SPSS Statistics 22 (SPSS IBM, Turkey) software package was used for statistical analyses. Shapiro–Wilk test was used to assess the suitability of the parameters to normal distribution while assessing the study data. While evaluating the study data, in addition to the descriptive statistical methods (mean, standard deviation, and frequency), Student’s t-test was used for the two-group comparisons of the normally distributed parameters and the Mann–Whitney U test was used for the two-group comparisons of the data without normal distribution in comparison of the quantitative data. Chi-square test, Fisher’s exact Chi-square test, and continuity (Yates) correction were used to compare qualitative data. Logistic regression analysis was performed for multivariate analysis. Significance level was found to be p < 0.05.
Results
As a result of the evaluation of 321 patients who were registered with SVT ICD code in our ED between 1 January 2015 and 31 December 2016, 137 patients were excluded from the study due to exclusion criteria. A total of 184 patients diagnosed with PSVT were included in our study. Since 10 of these patients had incomplete data in the files and 15 of them did not have their troponin level checked, they were not included in the study and our study was carried out with 159 patients (Figure 1).
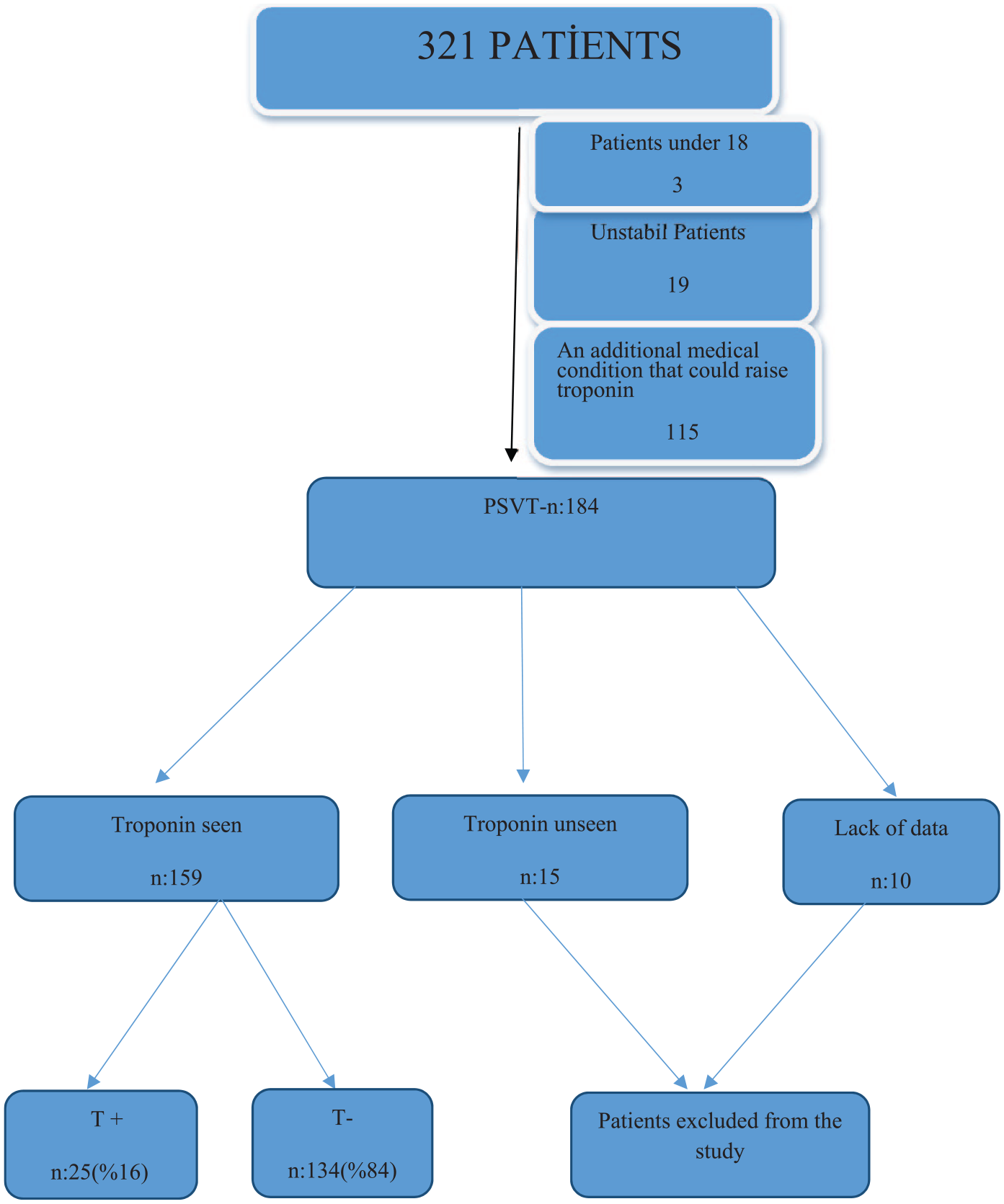
Patient flowchart.
Of the patients, 93 (58.5%) were female and 66 (41.5%) were male. Their age ranged from 18 to 90 years and the mean age was 53.70 ± 16.10 years. While troponin was positive in 25 (15.7%) cases, it was negative in 134 (84.3%) cases. Table 1 shows the age and gender, and Table 2 shows vital signs of troponin-positive and troponin-negative cases at the time of admission to hospital.
Age and gender evaluation according to troponin positivity.
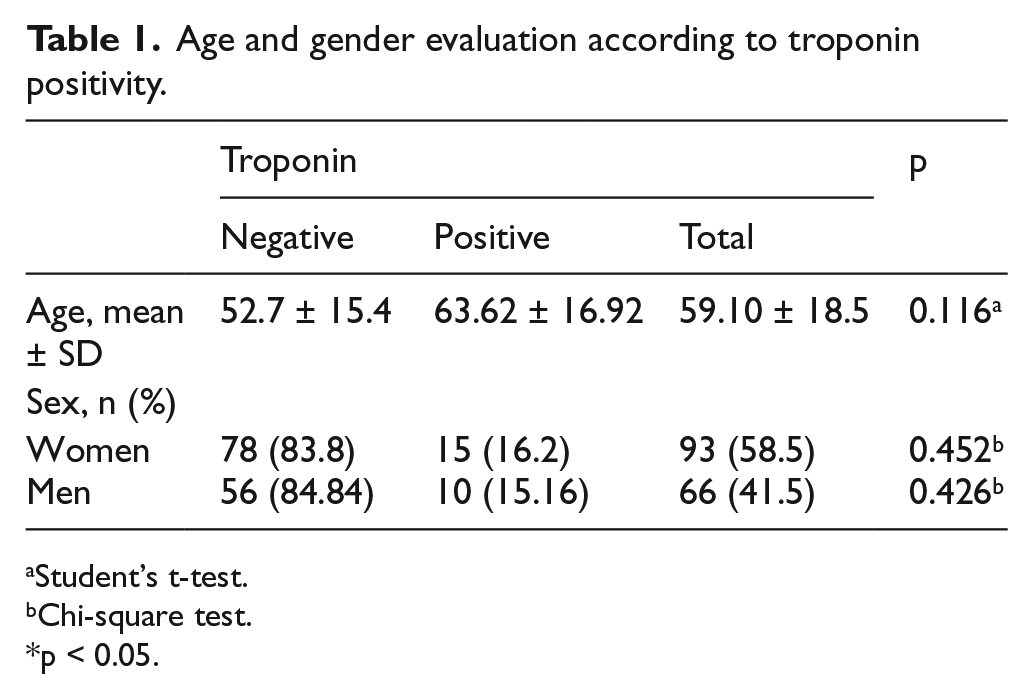
Student’s t-test.
Chi-square test.
p < 0.05.
Evaluation of systolic blood pressure, diastolic blood pressure, and pulse according to troponin positivity.
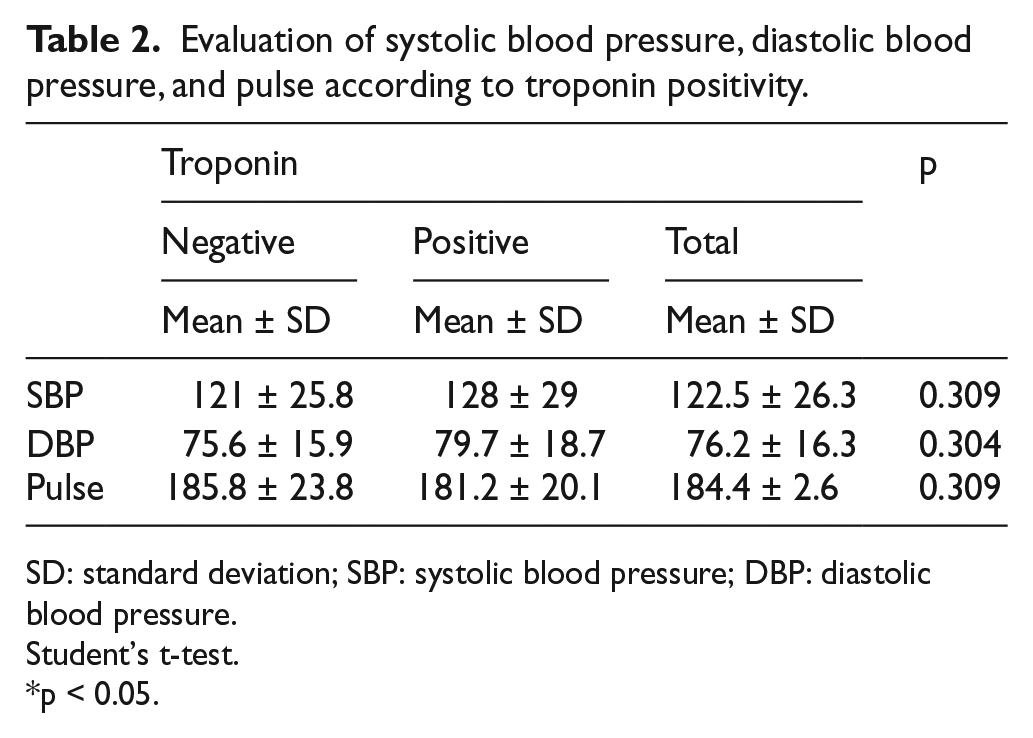
SD: standard deviation; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Student’s t-test.
p < 0.05.
In the 30-day mortality examination of troponin-positive and troponin-negative patients, mortality was not observed. In troponin-positive cases, 90-day mortality rate was 0%, and in troponin-negative cases, it was 0.8%, and there was no statistically significant difference between them (Table 3).
Evaluations of troponin positivity.
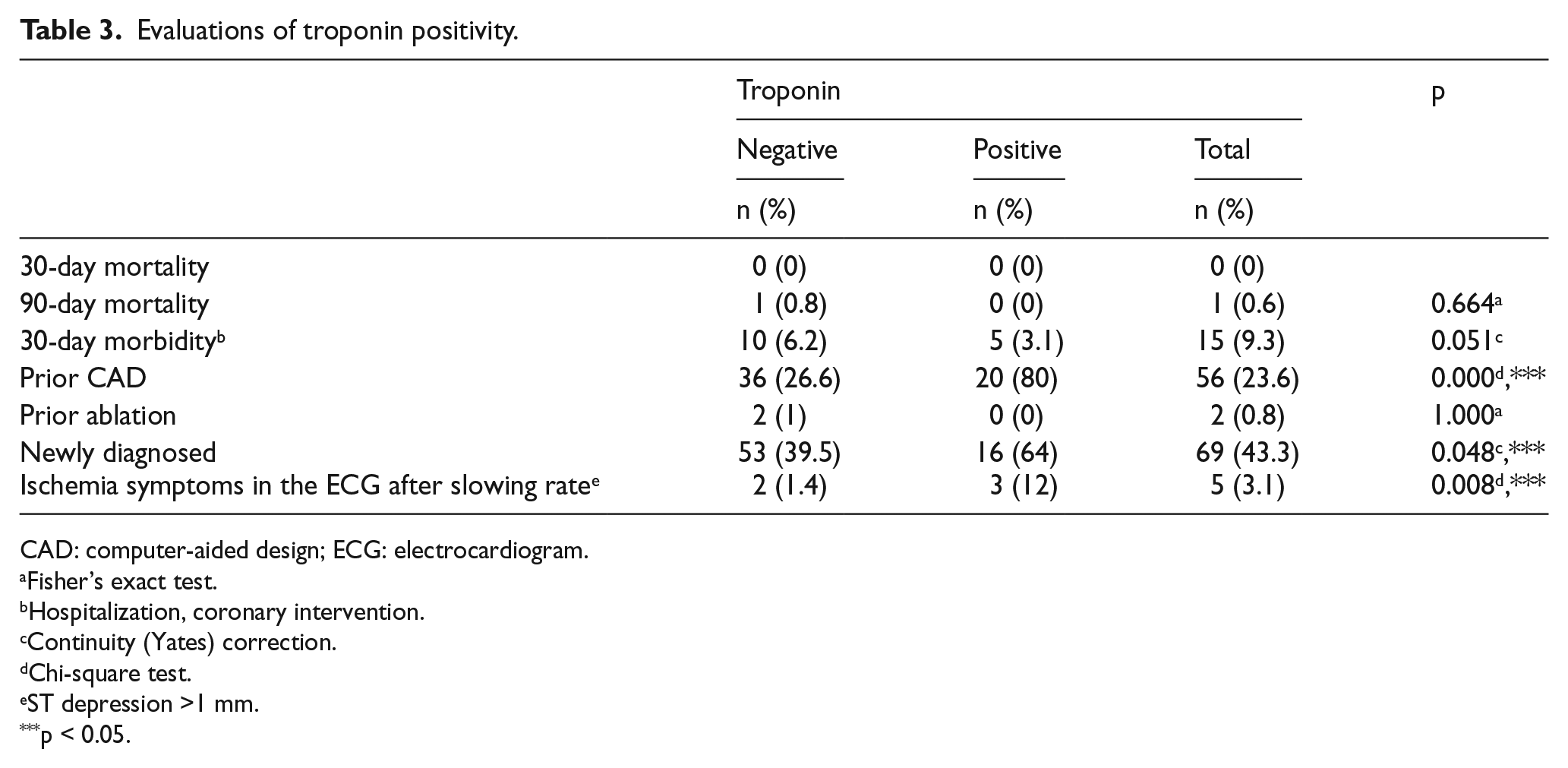
CAD: computer-aided design; ECG: electrocardiogram.
Fisher’s exact test.
Hospitalization, coronary intervention.
Continuity (Yates) correction.
Chi-square test.
ST depression >1 mm.
p < 0.05.
Troponin-positive cases (80%) had significantly higher rate of family history of coronary heart disease compared to troponin-negative cases (26.6%) (p < 0.05). The risks of encountering family history of coronary heart disease in troponin-positive cases are 3.07 times higher (odds ratio: 3.0673; 95% CI: 1.738–6.916).
There is no statistically significant correlation between having troponin-positive and ablation history. The rate of troponin-positive cases, being a new diagnosis, was 39.5%, while this rate was 64% in troponin-negative cases, and there was a statistically significant difference between them (Table 3).
The rate of observing ischemia in the ECG was statistically significantly higher in troponin-positive cases (12%) than that of the troponin-negative (1.4%) cases after the rate slowed down (p = 0.008; p < 0.05) (Table 3).
The risk of observing ischemia in the ECG is 8.5 times higher in troponin-positive cases (odds ratio: 3.353; 95% CI: 1.2–9.365) (Table 3).
As a result of subsequent percutaneous coronary intervention performed in 9 cases, acute myocardial infarction was detected in 3 of 9 cases with troponin-positive in patients with PSVT (Table 4).
Characteristics of patients diagnosed with PSVT and who underwent coronary intervention.
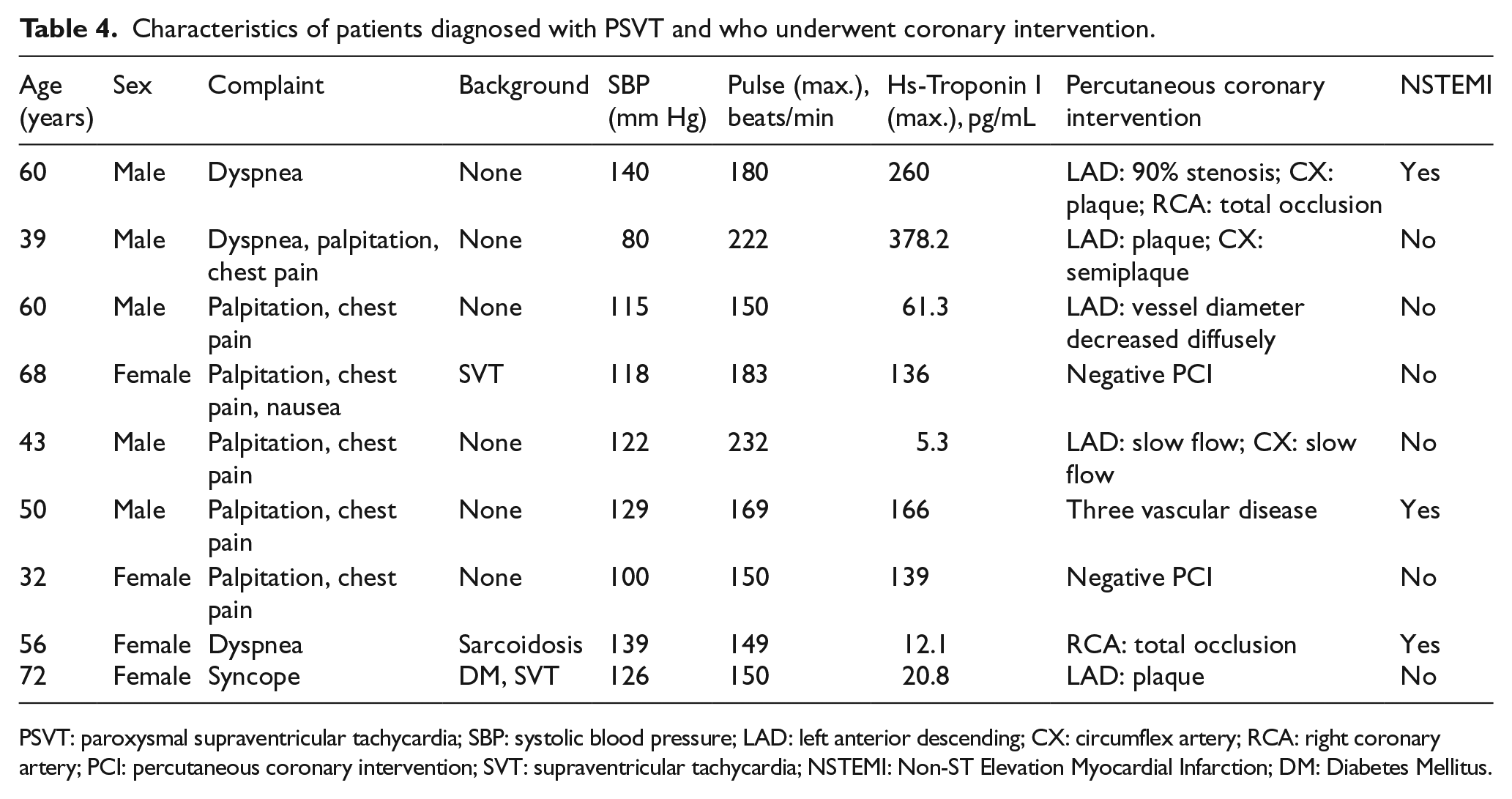
PSVT: paroxysmal supraventricular tachycardia; SBP: systolic blood pressure; LAD: left anterior descending; CX: circumflex artery; RCA: right coronary artery; PCI: percutaneous coronary intervention; SVT: supraventricular tachycardia; NSTEMI: Non-ST Elevation Myocardial Infarction; DM: Diabetes Mellitus.
Discussion
This study aims to determine the relationship between troponin levels and the 30- and 90-day mortality rates in patients applied to the emergency service with the diagnosis of PSVT. There was no significant difference between the 30- and 90-day mortality rates among patients with positive and negative troponin values.
PSVT is a heart rhythm disorder that is seen in 35 out of 100,000 people on average every year. 8 Patients are frequently referred to emergency services and receive their first treatment here. 9 PSVT can be seen in all age groups. 10 A study by Goebel et al. 11 indicated the mean age of patients with SVT as 60 years, Dogan et al. 12 indicated it as 57.9 years, Luber et al. 13 indicated it as 53 years, and Karcıoğlu et al. 14 indicated it as 49 years. The mean age in our study was 53.7 years, which is similar to previous studies.
It is stated in previous studies that PSVT was more common among women. 11,15 Goebel et al. reported that 70% of the SVT cases, Luber et al. 13 reported that 51% of the PSVT cases, and Karcıoğlu et al. 14 reported that 52.9% of the cases were female. Similar to previous studies, the incidence of PSVT was more frequent in female patients (58.5%).
In our study, the prognostic value of troponin values in PSVT patients was investigated, and it was observed that 25 out of 159 PSVT patients had troponin-positive. As a result of examination of the data, no statistically significant difference was observed between these patients and patients with troponin-negative in the 30- and 90-day mortality and 30-day morbidity rates. In a retrospective study by Carlberg et al., troponin value was measured at least once in 38 of 51 patients with PSVT. A total of 11 patients with increased troponin values were followed up for 30 days, and no cardiovascular events were observed in any of the patients. 16 In a study performed by Chow et al., 29 out of 78 PSVT patients had an increase in their troponin level, and they were followed up for an average of 2.2 ± 1.7 years. As a result of this study, it was concluded that a mild elevation in troponin increases the risk of cardiovascular events, such as death in PSVT, myocardial infarction, and hospitalization. 17
In our study, three out of nine patients who underwent angiography were found to have clogged coronary arteries, and when the 90-day mortality of the patients was inquired, it was learned that one patient died from non-cardiac causes. Previous studies examining the relationship between troponin levels and cardiovascular events and mortality rates are mostly case reports, case series, or retrospective studies. Coronary arteries 6 were open in all PSVT patients who underwent angiography due to increased troponin in the case series with seven patients by Kanjwal et al., 7 in case report by Miranda et al., 18 in the case series with three patients by Yeo et al., 19 in the case series with four patients by Zellweger et al., in a prospective cohort study with three patients by Bakshi et al. 20 , and in a retrospective cohort study with seven patients by Redfearn et al. 21 However, Chow et al. 17 in their studies including 78 patients with PSVT diagnosis reported that 11 of these patients died, 2 of them were diagnosed with myocardial infarction, and 14 of them were hospitalized.
The biggest limitation in our study was the examination of the data of a small group of patients from a single center, retrospectively. This study was conducted in a tertiary state hospital and receives cardiac patients also at a certain rate. The scientific committee of our hospital allowed us to use 2-year data for this study. So, any patient diagnosed as SVT at the emergency room (ER) admission was evaluated within the specified time interval. However, there is a cardiology center very close to our hospital. Therefore, patients who are aware of their present problem were probably admitted to the other hospital. It is possible that we caught fewer patients than the normal population. Data regarding the onset of symptoms of patients before they were admitted to the hospital were not available. Therefore, the comparative characteristics of patients with troponin values may not be fully met.
Conclusion
The study examined the relationship between troponin levels and the 30- and 90-day mortality rates and the incidence of cardiovascular events in PSVT patients. No significant difference was found between patients with positive troponin values and patients with negative troponin values in this respect. Since the causes of mortality of patients in our study were non-cardiac diseases, we think that the increase in troponin associated with PSVT will not cause permanent myocardial ischemia; however, we believe that prospective observational studies or large-scale retrospective studies will further clarify this subject.
Footnotes
Author contributions
R.A., S.Z.E.K., E.K. contributed to literature search; E.K., R.A., and S.Z.E.K. contributed to study design; R.A., S.P., and S.Z.E.K. contributed to legislative applications; S.P., S.Z.E.K., and E.K. contributed to data collection; E.K. and T.C.O. contributed to supervision and quality control, and statistical advice; E.K., T.C.O., and R.A. contributed to statistical data analysis; R.A., E.K., and T.C.O. contributed to data interpretation; R.A., E.K., S.Z.E.K., S.P., and T.C.O. contributed to drafting the manuscript. All authors were involved in the writing and critical revision of the manuscript and approved the final version. R.A. and E.K. take responsibility for the paper as a whole.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The authors agree to the conditions of publication including the availability of data and materials in our manuscript.
Informed consent
The need for informed consent was waived.
Ethical approval
This study was approved by the Local Ethics Committee.
Human rights
The principles outlined in the Declaration of Helsinki have been followed.