
Abstract
The long-term care system in Spain has been characterised by decentralisation, marketisation, fiscal austerity and its reliance on informal family care and cheap migrant labour. Focusing on home-help services, this article addresses the extent to which the sector’s multi-level system of collective bargaining can be characterised as fragmented and whether this has had a negative effect on employment conditions. The research involved an analysis of the legal and collective bargaining framework, expert interviews and employee focus groups. We argue that the precedence given to sectoral agreements within public procurement processes is one main factor preventing a move towards ‘disorganised decentralisation’ in the aftermath of the 2012 labour market reform. Moderate decentralisation has favoured heterogeneity in pay and working conditions at regional and provincial levels. However, these mid-level collective agreements have improved standards with respect to the national collective agreement, and there has been a minor increase in the number of company-level collective agreements since the reform. The limited professionalisation, the lack of recognition of skills and effort in occupational classifications, and the organisation of working time emerge as key contributors to the sector’s poor employment conditions.
Introduction
The development of the Spanish long-term care system is a paradigmatic example of what Rubery (2011) has called ‘reconstruction amid deconstruction’ – a twofold process whereby the deconstruction of social models to implement neoliberal policies coincides with demands to reconstruct them to meet new social needs. The development of an elder-care system in the 1990s and 2000s was characterised first by decentralisation under the flag of constructing the ‘autonomic state’; and second by marketisation, with expansion going hand in hand with a gradual dismantling and privatisation of public services. The attempt to construct a universal and service-based national system through the ‘Dependency Act’ faced severe limitations, especially as it was implemented in a context of recession and austerity. Reforms have so far not been successful in addressing deep-seated structural problems such as the lack of a clear definition of responsibilities across domains (health care vs. social services) and administrative levels (national, regional, supralocal, local), as reflected in the large differences in service provision, access criteria and pricing across territories.
As in many neighbouring countries, long-term care services are mainly commissioned through public procurement, with external contractors subject to reduced unit costs as a result of tighter public budgets and growing demands. Price tends to prevail as the most important criterion in tender processes in this labour-intensive sector, with negative effects on service and employment quality – a situation made worse by the constraints of so-called fiscal austerity policies. In short, institutional fragmentation, marketisation and insufficient funding shape the contours of employment in the Spanish long-term care sector. Against this background, the article addresses other distinct aspects of the Spanish model as challenges for improving employment conditions in the sector: the intricacies of the multi-level collective bargaining system, the limited professionalisation of employment, the non-recognition of skills and effort, and the organisation of working time.
The Spanish long-term care system: a tale of institutional fragmentation, marketisation and limited funding
For a long time, Spain relied on intrafamily care and residual social assistance care for the dependent elderly. In the 1980s, competences for social services (including elder care) were transferred to regional and local administrations, with public-private collaborations becoming a distinctive trait of the system (Eurofound, 2015). A second wave of reforms occurred in the 2000s following the 2007 entry into force of the ‘Dependency Act’ (LAPAD), a notable attempt to respond to the ‘crisis of care’ by developing a professionalised care sector (Deusdad et al., 2016). Introducing a universal entitlement for people with different degrees of dependence reflecting old age, illness or disability, the reform was intended to establish a service-based universal care system. One of the options established in the LAPAD service catalogue (alongside teleassistance, day and night centres and residential services) was home help, designed to help the elderly continue living at home through assistance with personal care and housekeeping. The LAPAD established a mixed system of service provision in which private, for-profit and non-profit organisations were allowed to operate (Rebollar and Ruiz, 2018).
Implementation of the LAPAD has fallen short of expectations. While private care provision (through service vouchers) was in principle only envisaged as a substitute for public services (or publicly commissioned services) when unavailable, in practice it has become the norm (Aguilar-Hendrickson, 2020). Similarly, although the ‘allowance for family care’ – a cash transfer to beneficiaries being cared for by a family member at home – was conceived as an exception, its use is widespread, accounting for 30.26 per cent of all entitlements in 2019 (IMSERSO, 2020). As a result, a fragmented and market-oriented system has been built around cash transfers instead of coordinated service provision, and it continues to rely heavily on informal family care and directly hired cheap migrant labour (León and Pavolini, 2014; Martínez-Buján, 2014). Two main factors explain the LAPAD’s limited success: the system’s complex and fragmented institutional design and budgetary constraints.
As regards the first factor, despite the formal establishment of a ‘national system’, 17 regional systems coexist. LAPAD’s attempt to consolidate a set of existing decentralised and fragmented structures into a single framework has resulted in a complex multi-level system of governance labelled as a ‘vicious layering’ of responsibilities in the field (Arlotti and Aguilar-Hendrickson, 2018). The national framework establishes minimum eligibility criteria and care standards, while guaranteeing a minimum share of funding. However, the regions are responsible for structuring the system on their respective territories and for topping up benefits, making funding unstable and unequal across territories (Aguilar-Hendrickson, 2020; Spasova et al., 2018). As a result, distinct elder-care regimes coexist within Spain’s regions, characterised by disparate development degrees of the different types of services and varying importance attached to care provided by family members or domestic workers (Martínez-Buján, 2014). Moreover, local authorities also have certain responsibilities for social services, meaning that service provision can at any one time be in the hands of regional and local authorities and of intermediate structures such as provinces or supralocal administrations. Different political agendas mean that stakeholders vary in their commitment to the system, exacerbating underlying inequalities and leading to significant differences between regions and municipalities in care provision, eligibility criteria and pricing in a nationally regulated care system (Spasova et al., 2018).
Second, LAPAD deployment was hindered by the severe budgetary constraints of austerity policies implemented mainly through two royal decrees (20/2011 and 20/2012). These (i) postponed full implementation of the reform by delaying the access of moderately dependent users; (ii) tightened the conditions for entitlement to a family care benefit, reduced its already low maximum amount (from €442.59 to €387.64) and did away with social security contributions for family carers; and (iii) decreased assignable hours for home-help 1 services. The result was a paralysis of the system between 2012 and mid-2015, while its progressive recovery since then has occurred at the expense of the regions and care recipients. Between 2009 and 2019, the level of state funding dropped from 39.2 to 15.6 per cent, while that of recipients and regions increased from 14.7 to 20.7 per cent and 46.2 to 63.7 per cent respectively (Ramírez Navarro et al., 2020). These developments have increased the vulnerability of many recipients and families already enduring financial hardship due to the recession. The ‘rationing’ of care packages has inevitably resulted in an increased reliance on informal family (female) care. Residential care facilities have become unaffordable for many families, with many instead opting to claim the ‘allowance for family care’ to make ends meet (Aguilar-Hendrickson, 2020). This process of ‘re-familialisation’ runs parallel with service marketisation, with citizens increasingly having to pay for care services, and with charities and community organisations attempting to fill the gaps (Deusdad et al., 2016). In short, austerity measures have seen the pendulum swing away from universalism and professionalisation back to ‘assistentialism’, marketisation and familialisation, reinforcing women’s roles as carers (León and Pavolini, 2014).
Data and methodology
Research methods included an analysis of collective bargaining regulations, interviews with key experts and employee focus groups. The fieldwork followed a top-down logic, going from the national level, via the regional and provincial levels, to the level of a company based in the metropolitan area of Barcelona (Table 1). Access to key informants in the field was facilitated by the secretariat for gender equality of a major trade union. The expert interviewees were mainly trade union officials belonging to collective agreement negotiating teams or with in-depth knowledge of the sector. In a snowball strategy, the initial interviewees provided access to other relevant informants in their branches at regional level. Participants in the focus groups were also recruited from among trade union members. At company level, we conducted interviews with worker representatives and human resources managers of a large company providing domiciliary care services. We also interviewed government officials in a large city where this company operated. Interviews and focus group discussions were conducted by the article’s lead author on the premises of either the trade union organisation or the companies involved. Interviews and focus group meetings were audio-recorded, transcribed and content-coded using Atlas.ti (version 8.4.0.).
Fieldwork and collective agreements analysed.
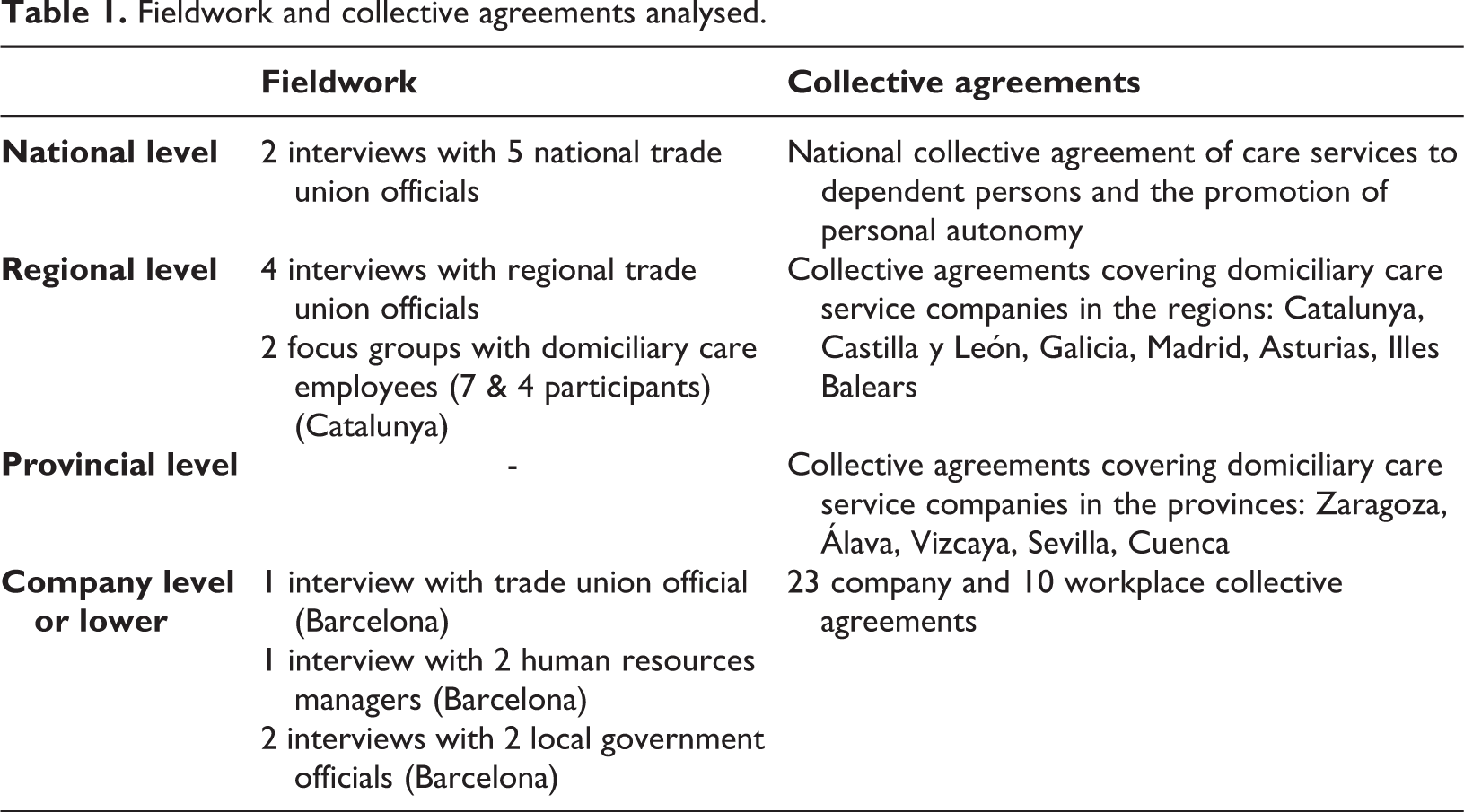
We analysed a total of 12 national, regional or provincial collective agreements covering domiciliary care service activities, and dozens of company and workplace collective agreements. We conducted 10 interviews with 12 informants and held two focus group meetings with 11 participants. Building on theoretically grounded criteria, a first round of collective agreement analysis helped identify critical issues to include in the interview guides. These were tailored to the interviewees at the different levels, though all covered at least the following topics: a) the dynamics of collective bargaining processes; b) occupational classification and job evaluation; c) training and qualifications; d) pay; e) working time. Interview guides were continuously adapted to the information collected in previous interviews, allowing further deepening and concretisation. This knowledge was subsequently used for a second round of collective agreement analysis. Focus group guides addressed employee perceptions on the content of their work, skills, pay and working conditions. The findings presented in the following sections consolidate these different sources.
The multi-level structure of collective bargaining in the long-term care sector: how much fragmentation?
In 2012, Spain underwent a labour market reform (Law 3/2012) giving company-level collective agreements precedence over sectoral collective agreements on such crucial issues as wages, the distribution of working time and adaptations of occupational classifications. It also made it easier for companies to derogate from higher-level agreements. These regulatory changes have been characterised in the literature as a move towards ‘disorganised decentralisation’ (Marginson, 2014). However, such a description does not reflect the reality of Spain’s long-term care sector where collective bargaining decentralisation preceded the 2012 reform, taking shape basically at regional and provincial levels, though structured by the national framework. Regional and provincial collective agreements improve standards with respect to the national collective agreement and there has been only a minor increase in the number of company-level agreements.
Several factors contribute to shaping the sector’s complex multi-level bargaining structure with its moderate degree of decentralisation and to limiting the shifts towards ‘disorganised decentralisation’: a) a legal framework that grants the regional collective bargaining level a specific role (consistent with Spain’s political configuration as an ‘autonomic state’), while attributing a certain centralising and homogenising power to national framework agreements; b) a fragmentation of the institutional framework and stakeholders (particularly on the employer side) of the long-term care system; c) the importance in the sector of public commissioning, which gives sectoral agreements precedence over company-level agreements.
Since the inclusion of night care centres and teleassistance in the fourth collective agreement in 2006, the national framework has covered virtually all the activities that constitute the national long-term care system under the LAPAD. Despite the extension of the national agreement’s functional scope, collective bargaining in the sector is relatively decentralised, taking place at regional and provincial level. Moreover, the regional and provincial collective agreements govern residential and home-help services separately, in contrast to the national framework. By way of example, in home-help services, the national collective agreement coexists with six regional and five provincial collective agreements, as well as 23 company-level and 10 workplace-level collective agreements.
While the 2012 labour market reform gave regional collective bargaining precedence, provincial negotiation units established in the sector before 2012 persist and are acknowledged on the collective bargaining map set forth in the national collective agreement. The extent to which the national collective agreement has exercised the power to centralise sectoral collective bargaining granted to it under the legislation is limited. This is not surprising, given the fragmented institutional framework of the long-term care system and its stakeholders, particularly on the employer side, which favours the multiplicity of negotiation platforms. Interests and strategies may vary significantly depending on the characteristics of the organisation concerned – SMEs/large companies, for-profit/non-profit, religious/non-religious, type of service, type of administration and rural/urban context. The difficulties in aggregating employer interests are illustrated by the fact that the employer side was only made up of the same organisations in the last two national agreements (sixth and seventh). Conflicts over the representativeness of employer organisations have landed in the courts, spilling over to the negotiating table via a questioning of the legitimacy of the national collective agreement. The workers’ side reflects Spain’s union concentration into two main organisations (Comisiones Obreras (CCOO) and Unión General de Trabajadores (UGT)) (Palomeque, 2010). However, differing negotiation priorities and strategies give rise to tensions within the workers’ representation, as illustrated by the fact that only the union with the largest representativeness (CCOO) has signed all agreements, while the UGT was absent from the third, the fifth and the seventh collective agreements.
Overall, the high level of conflict governing the national negotiating platform does not bode well for integration efforts. By way of example, after denouncing the sixth collective agreement, one of the employer organisations (Federación Empresarial de la Dependencia) refused to initiate negotiations for a new collective agreement, and the Interconfederal Service for Mediation and Arbitration had to intervene. 2 By mid-2017, when the fieldwork was conducted, the Joint Commission of the sixth collective agreement had met 88 times in response to 590 requests for interpretation. The seventh collective agreement was only signed in mid-2018, 4.5 years after expiry of the previous agreement (2012–2013) and was the culmination of 42 months of intense and conflictual negotiations. A similar fate seems to have befallen negotiations over the eighth collective agreement, which, at the time of writing, were again deadlocked.
With regard to company-level collective agreements, their increase in the aftermath of the 2012 reform has been of little relevance both in number and in terms of the number of employees affected. Approximately half of the 23 company-level collective agreements for home-help services in effect at the time of writing concerned Extremadura (a region not covered by a regional or provincial agreement) and applied mainly to small companies in rural areas. A key explanation for this limited increase is the importance of public procurement within the sector. The Law 9/2017 on Public Sector Contracts overrides the priority assigned to company-level agreements in Article 84.2 of the Workers’ Statute in the event of a publicly owned service being outsourced via public procurement (Beltrán de Heredia, 2019). In services where labour costs constitute the main share of overall costs, the sectoral collective agreement must be applied for workers’ wages. This constraint may have significantly reduced employer incentives to negotiate company-level agreements. An additional reason may be the large share of small and medium-sized companies operating in the sector (85 per cent 3 ), many of which may not have an elected worker representation and are thus unable to negotiate a company-level collective agreement.
At the same time, several workplace-level agreements are to be found among large multi-utility companies such as Eulen, Valoriza or Clece, whose presence in the sector has gained in importance in recent years. Economies of scale have gradually squeezed out smaller firms and ‘social enterprises’ in favour of larger corporations, as in other European countries (Cunningham and James, 2017). In particular, the downturn in construction, industrial cleaning and security as a consequence of the 2008 crisis encouraged general outsourcing companies to diversify into home-help and other long-term care services (Eurofound, 2015). Overall, large corporate groups appear to feel comfortable with the national collective agreement, with company-level agreements and derogations mainly applying to smaller companies. The few workplace collective agreements signed by these multi-utility companies apply to domiciliary care services in specific municipalities not covered by regional or provincial agreements, and have significantly improved standards compared to those of the national collective agreement.
On the whole, the regional decentralisation of collective bargaining is consistent with the provisions of the legal framework; provincial decentralisation (five collective agreements) may be deemed low considering that Spain is divided into 50 provinces; while the number of company-level or below collective agreements is insignificant, not exceeding 2 per cent of all companies operating in the domiciliary care service sector. 4 Hence, collective bargaining decentralisation in the sector may be considered moderate but not fragmented (to be understood as disaggregated into smaller units of negotiation). These findings are consistent with studies showing that regulatory change in Spain has not fundamentally altered the prevalence of multi-employer agreements or collective bargaining coverage (López-Andreu, 2019).
The heterogeneity of employment conditions in the sector: how detrimental?
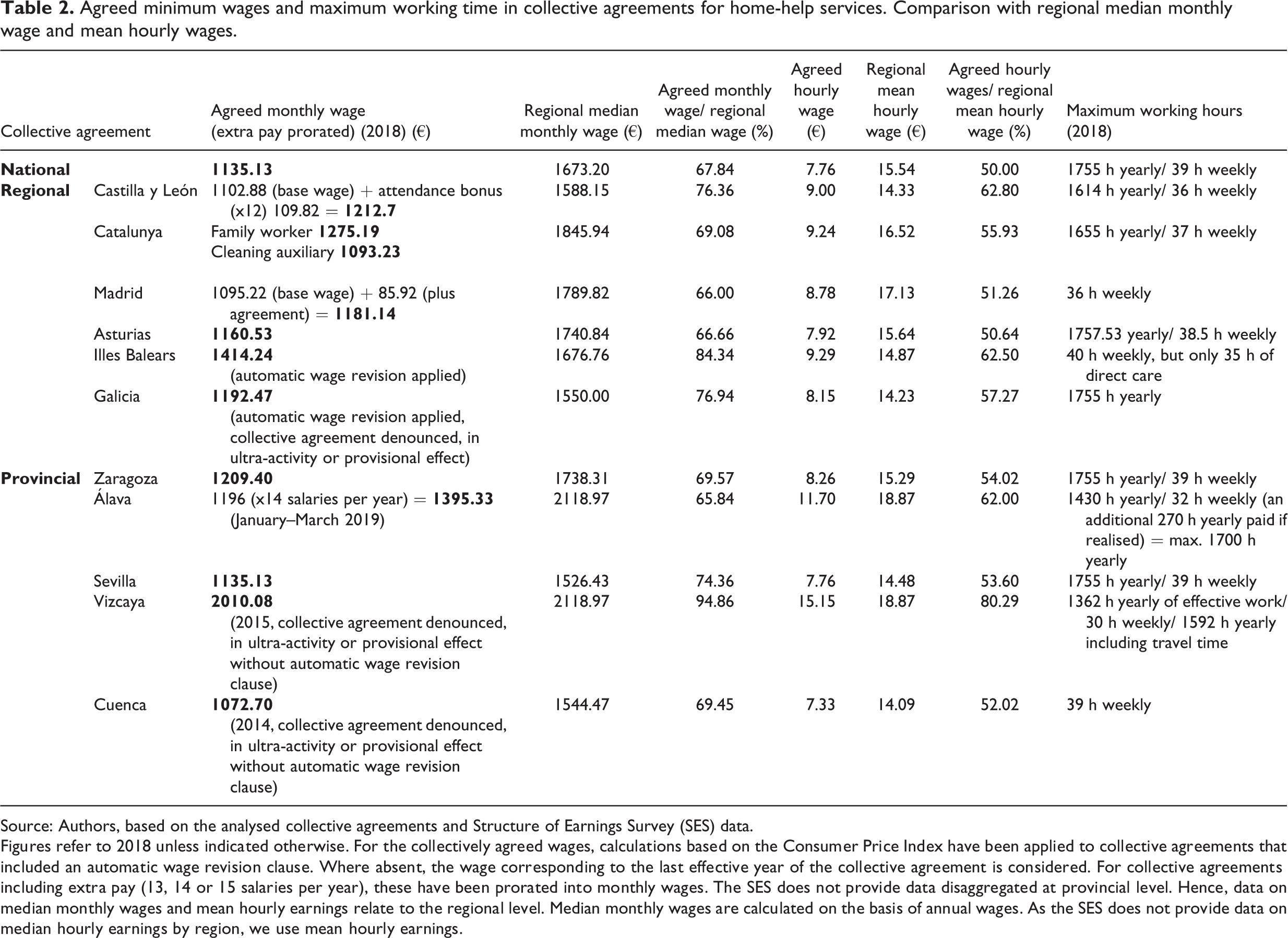
Regional and provincial collective agreements create heterogeneity in employment conditions across territories and types of services and distinguish between public and private employees. They generally constitute an improvement over the terms of the national collective agreement, decreasing incentives for their subsumption within the national framework. Article 84 of the Workers’ Statute offers some protection against any downgrading of annual working hours and occupational classifications (among other aspects) across regions. These conditions are considered non-negotiable unless otherwise specified in the national collective agreement (which is not the case). Moreover, the sector’s national collective agreement sets (inter alia) wages, weekly rest periods and holidays as minimum rights. 5 Therefore, the national collective agreement acts as a baseline for wages and working hours, while most regional and provincial agreements improve these standards, widening the gaps in employment conditions across territories (Table 2).
Agreed minimum wages and maximum working time in collective agreements for home-help services. Comparison with regional median monthly wage and mean hourly wages.
Source: Authors, based on the analysed collective agreements and Structure of Earnings Survey (SES) data.
Figures refer to 2018 unless indicated otherwise. For the collectively agreed wages, calculations based on the Consumer Price Index have been applied to collective agreements that included an automatic wage revision clause. Where absent, the wage corresponding to the last effective year of the collective agreement is considered. For collective agreements including extra pay (13, 14 or 15 salaries per year), these have been prorated into monthly wages. The SES does not provide data disaggregated at provincial level. Hence, data on median monthly wages and mean hourly earnings relate to the regional level. Median monthly wages are calculated on the basis of annual wages. As the SES does not provide data on median hourly earnings by region, we use mean hourly earnings.
In all cases, collectively agreed monthly wages are below the median wage of the corresponding territory. Seven of the 12 collective agreements analysed, including the national framework agreement, set monthly wages at 60 to 70 per cent of the median wage (just above the poverty threshold), and all but one set hourly wages at 50 to 60 per cent of the regional average wage. It should not be forgotten that monthly wages are full-time equivalent (FTE) wages, while take-home pay is in many cases much lower given the widespread use of part-time contracts in the sector. Notably, the collective agreements for the Basque provinces of Álava and Vizcaya have achieved a reduction of the working hours of key professionals at no detriment to their wage levels, resulting in comparatively higher hourly wages. However, when compared with regional pay levels, Vizcaya is the only case where care workers earn near-median wages. Moreover, regions such as Catalunya, despite a higher agreed wage than most territories, fare worse when comparing regional wage levels.
Illustrating the difficulties associated with a complete centralisation of collective bargaining, these territorial differences pose a strategic dilemma for unions. They have to decide whether to concentrate efforts on building collective bargaining power at national level, thereby sacrificing the gains made by regional officials, or whether to allow for territorial variation, thereby compromising the principles of consolidation and unification. While officials at the confederate level argue that the subsumption of regional and provincial agreements would strengthen workers’ bargaining power nationally, regional officials fear that collective agreement extension and harmonisation will lead to employment conditions being downgraded in territories with higher standards.
It is difficult to establish conclusively to what extent the moderate decentralisation of the collective bargaining system has been detrimental to employment conditions in the sector. What seems certain is that the limited ‘disorganised decentralisation’ has contained any deterioration. The few existing company-level agreements all set employment conditions below those of the national agreement, with hourly wages below €6 and 40-hour working weeks. Workplace agreements are a separate issue, as in this case sectoral collective agreements take precedence, meaning that employment conditions cannot be downgraded. Quite the contrary, the few existing agreements of this type significantly improve standards compared to those of the national collective agreement, with hourly wages set at over €12 and a maximum of 35 working hours per week.
Overall, the relatively decentralised collective bargaining system leads to heterogeneous employment conditions in the sector. However, there are other factors more likely to contribute to poor employment and working conditions, namely the sector’s limited professionalisation, the lack of recognition of skills and effort in occupational classifications, and the organisation of working time.
Limited professionalisation and lack of recognition of skills and effort
Although the professionalisation of the long-term care sector has been declared a priority by both the public administration and social partners, progress has been limited in a context of austerity and unmet demand for labour. The LAPAD contains merely vague references to training requirements and qualifications. In 2008, an agreement of the Interterritorial Council (the body responsible for coordinating the long-term care system) set the qualifications required for every worker within the LAPAD framework and defined the procedures through which occupational competences were to be accredited, setting December 2015 as the deadline. However, this initial deadline was never met, and later agreements of the Council successively extended it to 2017 and 2022. ‘Exceptional authorisations’ (Habilitación excepcional) were also introduced to allow workers without the necessary qualifications but with a certain amount of experience or hours of training to work within the system. 6 These successive postponements and relaxation of requirements are mainly the result of the increasingly unmet demand for labour in the sector, overriding concerns over the quality of services and employment. As a consequence, administrations and companies providing these services have in turn relaxed their qualification requirements. Workers are often hired without any training and, even though the procurement authorities may set contractual obligations for companies to train new employees, they rarely monitor their fulfilment (Rebollar and Ruiz, 2018).
Overall, qualification and accreditation processes have not delivered the expected improvements in the recognition of these occupations and pay. In fact, according to the union officials interviewed, they may even have had the perverse effect of devaluing certain qualifications treated as equivalent to those gained via other training programmes involving half the hours. Moreover, by establishing work experience as an alternative to qualifications, they may have helped de-professionalise care work, in contradiction to the stated goal of professionalisation (Roca Escoda, 2017). These developments constitute a sort of vicious circle, whereby low wages and precarious working conditions make care occupations unattractive, resulting in a lack of incentives to stay in the sector and improve one’s skills. As a consequence, there are insufficient workers with the required qualifications, making it harder to improve the social (and monetary) recognition of these occupations.
At collective bargaining level, this limited professionalisation is evidenced in the definition of occupational groups and categories and the lack of training requirements. The national collective agreement – the only collective agreement competent to do so – does not require a given certification for the position of a home-help carer (auxiliar de ayuda a domicilio), the key occupation in direct care provision. Moreover, neither the national nor lower-level collective agreements define specific training programmes for professionalising such roles and/or making it easier to obtain the qualifications or accreditations set by the national qualifications system and the applicable legislation. There is thus a major hiatus between the formal professionalisation model and its implementation in collective agreements.
Moreover, according to the interviewed union officials, employer organisations are against translating the functions and competences assigned by the national qualifications system to the sector’s main roles into the national collective agreement’s occupational classification. The definition of the different occupational roles and the delineation of their tasks constitute a critical collective bargaining issue and were the main reason for the deadlock in the negotiations over the seventh collective agreement. Unions have long fought to handle care staff and cleaning staff in residential services in two distinct occupational groups, a move which employers oppose because it would prevent using care staff for cleaning purposes. In domiciliary care services, the auxiliar de ayuda a domicilio performs both personal care and domestic housekeeping tasks. Although personal care tasks take precedence over cleaning tasks under LAPAD regulations, the latter often account for most of the work performed by care workers. The lack of training of many new-hires favours the orientation of their work towards this type of task. Moreover, as a result of the lack of individualised instructions, care workers often find themselves having to negotiate the work to be performed with care recipients or their families (Rebollar and Ruiz, 2018).
In general, occupational classifications in the collective agreements analysed establish a clear separation between direct care provision and technical and management work, undervaluing the former (Recio Cáceres et al., 2015). This fact is intimately associated with low wages. Occupational classifications ignore the skills, responsibilities and efforts of home-help services staff involved in direct care provision. Moreover, the pay structure in all of the collective agreements analysed is essentially focused on rewarding time availability, disregarding other conditions of work execution that would make it easier to reward care workers’ psychosocial or physical efforts or even their exposure to health hazards. Although not formally recognised, companies informally leverage care workers’ specific skills and abilities. For instance, focus group participants reported that workers with greater experience or particular skills were assigned to care recipients presenting more complex situations, for example involving mental health issues or conflictual environments. However, these capabilities and efforts were not financially rewarded.
The organisation of working time: short, fragmented and irregular hours
Another main factor contributing to low wages is the widespread use of part-time contracts. Take-home pay is thus significantly lower than negotiated wages, making it very hard for these workers to live on their wages. This widespread use of involuntary part-time contracts is intimately linked to a procurement system that sets hourly fees and determines each user’s care package in given time blocks. Part-time contracts have become the preferred form of flexibility for service providers, accounting for 50 to 80 per cent of all employment contracts within the companies studied. Given that the needs and demands of care recipients tend to follow an hourglass pattern (concentrated in morning and evening hours), part-time workers may have extended and fragmented work schedules, with marginal part-time contracts used to cover any gaps. According to one union official, another factor favouring part-time contracts is that they allow employers to circumvent the 15-minute break rule guaranteed by the Workers’ Statute (extended to 20 minutes by the collective agreements of Catalunya and Zaragoza) when a working day exceeds six hours.
Most collective agreements limit the use of part-time work through setting a minimum duration for part-time contracts (between 20 and 25 hours). However, exceptions are envisaged for services whose (unspecified) characteristics may require shorter durations. It is also common to establish a precedence of extending part-time contracts rather than hiring new workers to cover for new services or vacancies, but organisational reasons are often put forward to hinder such extensions. Moreover, the regulation of additional hours (horas complementarias) in part-time contracts – which differ from overtime – provides companies with great flexibility in the management of working time. Collective agreements establish the possibility of agreeing on the performance of additional hours representing up to 30 per cent (40 per cent in Catalunya) of the working hours set in the employment contract. While these agreed additional hours are always optional for companies and are only paid when actually performed, they are always mandatory for part-time employees if the company demands their fulfilment. As a result, part-time workers may find themselves having to cope with major fluctuations in working time and pay. This is very often the case, given that service provision may be affected by such eventualities as a recipient’s death or his/her move to a social or health-care institution.
However, this reality is not commonly acknowledged within collective agreements, with only those of Álava and Illes Balears containing some form of wage guarantee: at least 50 per cent of staff are to work the maximum monthly working hours set in the collective agreement (Álava); or all workers are to work their contractually set hours (Illes Balears). Most collective agreements establish that hours not completed within the reference period must be compensated during the following period, generally within the ordinary working time established in the employment contract but also possibly outside of it, which leads to an irregular distribution of working hours. However, this flexibility is not compensated by availability bonuses, as fluctuations in service are considered part and parcel of normal service provision.
Providers’ efforts to minimise costs within a time-based commissioning system result in heightened work intensity and a lack of rest time, findings consistent with studies in other contexts (Rubery et al., 2015). Re-familialisation processes triggered by the recession and austerity have intensified this reality. According to our focus group participants, the families of dependents with complex health needs and unable to afford residential care combine home-help services and family care in a patchwork-like remedy. Hence, home help has progressively lost its role of supporting the autonomy of mildly dependent users, instead becoming a service increasingly oriented towards persons in need of intensive care. Care staff often do not have the time or adequate means to attend to the needs of care recipients, resulting in increased mental and physical strain. Austerity measures have gnawed away at allotted hours, with the maximum number of home-help hours reduced in each dependency category (Ramírez Navarro et al., 2020). Workers are reluctant to leave their work unfinished when they detect unmet needs and often extend their services at the expense of their rest time or by increasing their (unpaid) hours.
Discussion
The article has looked at the multi-level structure of collective bargaining as a challenge for improving employment conditions in the long-term care sector in Spain, engaging with discussions on ‘disorganised decentralisation’ (Marginson, 2014). We have argued that the system’s level of decentralisation may be considered moderate and largely consistent with the provisions of a legal framework assigning regional negotiation bodies a particular role, and where regional and provincial decentralisation has been shaped by the national framework. We did not observe any shift towards the ‘disorganised decentralisation’ anticipated by the literature. Among other reasons, the contained increase of company-level agreements is attributable to the importance of the public administration as a service procurer and, specifically, to the centrality that the legal framework grants to sectoral agreements within public procurement processes. The poor employment conditions of the sector’s few company-level agreements suggest that their limited increase has prevented working standards from deteriorating. Hence, we argue that the sector’s collective bargaining system is not best characterised as fragmented. However, it is difficult to gauge to what extent the long-term care system’s fragmentation and collective bargaining decentralisation have been detrimental to employment conditions, as they have been inherent to the development of the Spanish model. Collective bargaining decentralisation can be considered a constraint on unions’ capacity to build negotiating power at national level. At the same time, decentralisation opens the door to local processes yielding gains for employment conditions, as illustrated by the Basque example, which may or may not spread to other negotiation units. Overall, while the relative decentralisation leads to heterogeneous conditions between workers across regions and types of services, it is neither the only nor the main factor accounting for the sector’s poor employment conditions. It also does not explain the widespread use of part-time contracts or the low wages, which remain below the median wage in every territory regardless of differences.
In this sense, the article also highlights the relevance of qualifications and the recognition of skills and effort from a gender perspective for raising employment standards, and the importance of addressing the organisation of working time to tackle low wages. While accreditable qualifications are defined through a centralised system, accreditation is organised by the regions, leading to considerable differences in criteria and timelines and possibly hindering the national definition of clear and recognisable occupational roles. However, barriers to professionalisation are not mainly the result of the fragmentation of long-term care or collective bargaining institutions. Collective agreements fail to promote professionalisation at all collective bargaining levels. Low pay and harmful working conditions are features common to all regions, leading to the high staff turnover that favours the vicious circle of under-professionalisation. These dynamics must be situated within the country’s wider institutional and social context. The LAPAD’s declared objectives of fostering professionalisation while promoting the ‘family carer’ constitute contradictory policy orientations. These inconsistencies intersect with a familialistic culture where a majority of the population still prefers to be cared for at home by family members, i.e., by a female relative without specific skills or knowledge. Similarly, no special training requirements are expected of any migrant carer hired informally as an alternative to unaffordable services (Moreno-Colom et al., 2017).
Public intervention contributes to drawing this wider setting shaping work standards in the sector, but has also a more specific role as a commissioner of services. In this sense, there is leeway for public action on low pay through linking (negotiated) wages and prices in procurement processes. According to Spanish administrative law, wages established by the corresponding sectoral collective agreement serve as a reference for pricing services in public tenders. When asked about the factors hindering wage increases in the sector, the ‘blame game’ proved common among the stakeholders interviewed. Employers argued that there could be no increase in agreed wages without the corresponding administration proportionally raising its fees – which is not administratively feasible for ongoing contracts. Conversely, administrations argued that it was up to employers and unions to negotiate wages, as the contracting authority simply applied the reference collective agreement. However, (exceptional) examples show that where the political will exists, tender prices can be aligned with a collective agreement. In the province of Álava, a tripartite agreement was reached following worker mobilisation, under which the administration raised the hourly price by 10 to 13 per cent to reflect the 7.1 per cent increase in wages agreed in the provincial collective agreement. It should however be noted that Álava is one of Spain’s wealthiest provinces and its capital (Vitoria-Gasteiz) a medium-sized city. Issues of scale and budget certainly affect the chances of reaching this kind of agreement. Nonetheless, this example shows that when the necessary bargaining power, favourable political climate and budgetary leeway exist, improving employment conditions is possible. More generally, there is also a need to reconsider a procurement system dictated by hourly fees, and thus likely to transfer any pressure on unit costs onto workers’ shoulders in terms of part-time, extended, fragmented and irregular work schedules and high work intensity, especially within a context of austerity. Any understanding of collective bargaining dynamics and employment conditions in the long-term care sector thus requires consideration of the regulatory set-up and the broader contours of public intervention.
Concluding remarks: COVID-19 and future challenges for the Spanish long-term care system
The weaknesses of the Spanish long-term care system were well and truly uncovered during the COVID-19 pandemic, with major repercussions for care workers and dramatic consequences for care recipients. Excess mortality amounted to 43,938 just between 13 March and 22 May 2020, of which 84 per cent concerned people aged 74 years or older, pointing to an excess mortality of 67.3 per cent (MoMo, 2020). Deaths among care home residents represented 50 to 70 per cent of all fatal cases during the first wave of the pandemic (ECDC, 2020; MSF, 2020). Although a detailed evaluation of the causes of this situation is beyond the scope of this article, preliminary reports point to the critical role of distinct aspects of the Spanish long-term care system.
First, the system’s institutional and territorial complexity, the multiple forms of care provision and the actors involved (public, private, mixed, voluntary, religious) require a high degree of coordination, joint strategies and a clear definition of responsibilities. This was unfortunately not achieved, resulting in bottlenecks, delays and contradictory measures (GTM, 2020; MSF, 2020). Second, with the long-term care system defined as a branch of social services, residential homes are not regarded as health-care centres and do not receive any distinct treatment within the health-care system either. Generally speaking, staff have no medical training. As a consequence, in the earliest days of the pandemic, residential homes received no personal protection equipment. The government response was focused on preventing a collapse of the health-care system, often hampering transfers of dependent elderly to hospitals (GTM, 2020; MSF, 2020). According to Médicos sin Fronteras (MSF, 2020), by the end of May 2020, 56 per cent of all those infected by COVID-19 in residential homes died at home or in hospital, while 44 per cent passed away in the residential home without having been transferred to a hospital. Third, the lack of adequate spaces, high occupancy rates and heavy staff workloads hindered the implementation of proper zoning strategies to prevent contagion among residents (MSF, 2020). While our research shows that pre-pandemic caregiver/care recipient ratios were already too high to ensure proper care (Sánchez-Mira et al., 2020), the public health crisis dramatically worsened this situation due to the absence of those care workers who contracted the illness while working without proper equipment or without training on how to use it (GTM, 2020; MSF, 2020). While we know that health-care workers accounted for 20 per cent of all declared COVID-19 cases by mid-April in Spain – one of the highest ratios in Europe (ECDC, 2020) –, the lack of comparable figures for care staff contributes to the invisibility of the risks these workers were exposed to. Although less dramatically affected than residential home staff, domiciliary care workers also had to put up with a lack of clear instructions, proper equipment and training and with seeing their employment contracts altered following the suspension of services (Moré, 2020). Domestic workers were placed in particularly vulnerable situations as they were not covered by the government’s temporary unemployment scheme. Similarly, workplace health and safety regulations do not apply to them, and some were forcedly confined to their workplace (Moré, 2020).
The COVID-19 pandemic has spotlighted a series of structural deficits in the Spanish long-term care system, largely overlapping those identified in the article. In summary: (i) institutional fragmentation and a lack of coordination and proper definition of responsibilities across fields (health care vs. social services) and administrative levels (national, regional, local); (ii) insufficient funding, aggravated by austerity policies; (iii) underdevelopment of professionalised services (in particular preventive and domiciliary care services); (iv) understaffing and undertraining; and, finally, (v) insufficient quality assurance measures.
From an employment and working conditions perspective, the main challenges for collective bargaining include: (i) the professionalisation of direct-care work, (ii) the revaluation of wages, (iii) the limitation of involuntary part-time contracts and the irregular distribution of working time, (iv) the fair evaluation of skills, effort and the biological and psychosocial risks associated with the main caregiving roles. The moderate degree of collective bargaining decentralisation in the sector does not seem to be an intrinsic obstacle to achieving these goals, despite producing territorial heterogeneity.
From a public intervention perspective, policies that (i) promote the consolidation of a unified professionalisation model for the long-term care system, (ii) guarantee that all regions have adequate funding, and (iii) set common standards for service provision – such as optimal staff ratios to mitigate the high work intensity –, may contribute to improving and harmonising employment conditions in the sector. It remains to be seen whether public authorities will take seriously the lessons learnt at such a high cost during the pandemic.
Footnotes
Acknowledgements
The authors would like to thank the members of the advisory board of the BridgeS project, the national and Catalan secretariat for gender equality of Comisiones Obreras for facilitating the access to the field, the companies who agreed to participate in the study, and all the informants who participated in the interviews and focus groups for their time and invaluable insight. The authors are also grateful to the special issue editors and anonymous reviewers for their helpful comments on the manuscript.
Funding
This study was supported by the Recercaixa grant ‘The Gender Pay Gap: A Multidimensional Phenomenon (BridgeS)’ [Grant number 2015ACUP0179] by ‘la Caixa’ Bank Foundation with the collaboration of the Catalan Association of Public Universities (ACUP).