
Abstract
Objective
To evaluate the feasibility of applying balloon dilation technique in the eggshell procedure via pedicle subtraction osteostomy (PSO) for thoracolumbar kyphosis secondary to ankylosing spondylitis (AS).
Methods
Prospective randomized controlled study. A total of 35 AS patients with thoracolumbar kyphosis admitted to the Department of Spinal Surgery, Changsha Central Hospital from October 2021 to October 2023 were enrolled and divided into two groups: the balloon group (n = 16) and the non-balloon group (n = 19). Both groups underwent spinal wedge osteotomy combined with pedicle screw fixation. The balloon group utilized balloon dilation to remove cancellous bone, while the non-balloon group employed the conventional eggshell technique. Surgical duration, intraoperative blood loss, complications, hospital stay, postoperative functional recovery, and degree of spinal deformity correction were assessed and compared.
Results
Significant differences were observed between the two groups in surgical duration, intraoperative blood loss, and hospital stay (p < 0.001). No complications such as poor wound healing or surgical site infection occurred in either group. All 35 patients were followed up for an average of 18.5 months. Both groups showed significant improvements in VAS and ODI scores at 1 week postoperatively and final follow-up compared to preoperative values (p < 0.05), with statistically significant differences between the two groups at 1 week postoperatively (p < 0.05). Radiographic parameters (TLK, LL, SVA, PT) significantly improved in both groups at 1 week postoperatively and final follow-up (p < 0.05), except for TK, which showed no significant change (p > 0.05). No significant differences were found in radiographic parameters between the two groups at 1 week postoperatively or final follow-up (p > 0.05).
Conclusion
The application of balloon dilation technique in PSO eggshell procedures offers advantages such as reduced intraoperative blood loss, shorter surgical duration, and enhanced safety. It represents a valuable surgical technique worthy of promotion in the correction of thoracolumbar kyphosis secondary to AS.
Keywords
Ankylosing Spondylitis (AS) is a systemic autoimmune disease primarily affecting the axial skeleton, peripheral joints, and soft tissues. It predominantly occurs in young males and is characterized by ossification of spinal ligaments, leading to bony bridging between vertebrae and “bamboo spine” formation. Clinical manifestations include sacroiliac pain, progressive spinal stiffness, thoracolumbar kyphosis, and in advanced stages, difficulty in horizontal gaze and supine positioning.1–3 Severe thoracolumbar kyphotic deformities often require corrective spinal osteotomy.
Pedicle Subtraction Osteotomy (PSO), first proposed by Thomasen in 1985, remains one of the most widely used spinal osteotomy techniques. It offers advantages such as excellent postoperative stability, high fusion rates, and minimal correction loss. 4 In the same year, 5 Heinig C formally introduced the “eggshell technique,” which involves removing cancellous bone through the pedicle to create a cortical shell, facilitating easier closure of the osteotomy site by enhancing middle column compressibility. 6 This innovative concept paved the way for subsequent developments in osteotomy and deformity correction techniques. However, this technique has limitations, including procedural complexity, significant intraoperative blood loss, and high technical demands on surgeons. 7 In the treatment of osteoporosis patients, Percutaneous Kyphoplasty (PKP), utilizing an inflatable balloon to compress cancellous bone and create a cavity, can restore vertebral height while preventing endplate damage.8,9 Building upon this concept, this study aims to evaluate the clinical efficacy of balloon dilation technology when applied to the eggshell procedure during PSO for correcting thoracolumbar kyphosis in AS patients.
Materials and methods
General data
General information of patients between balloon-assisted and conventional groups.
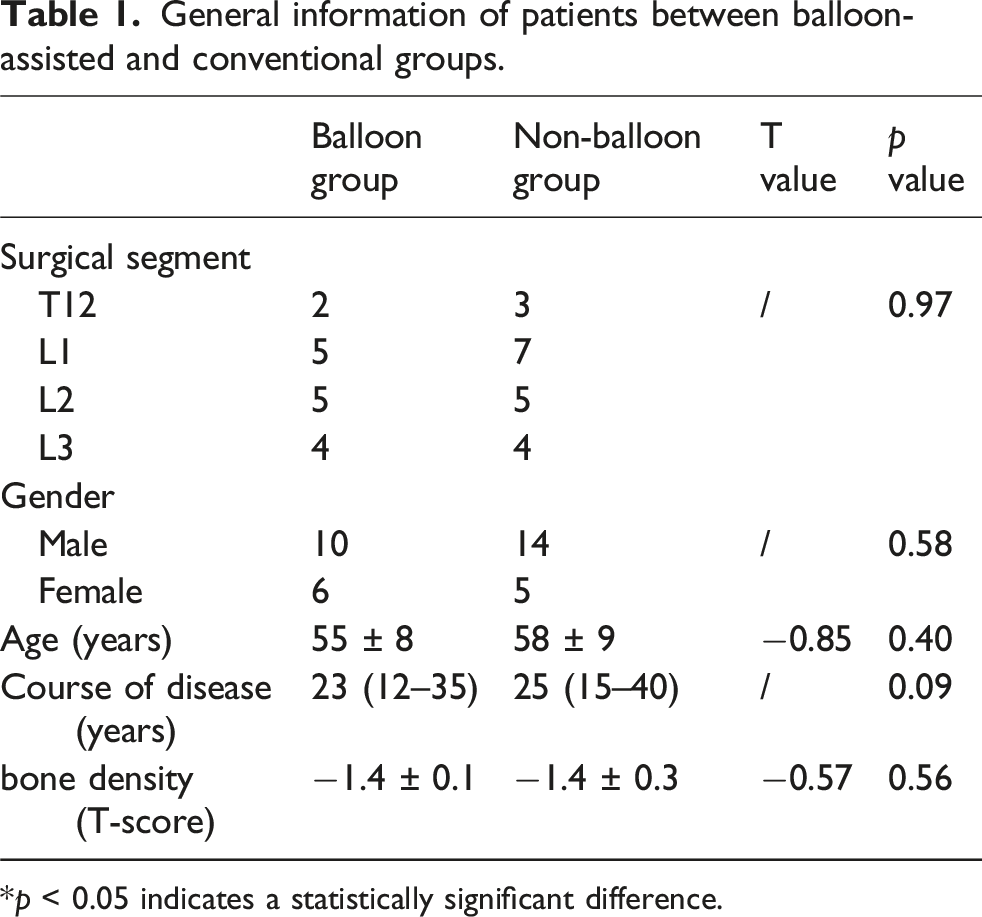
*p < 0.05 indicates a statistically significant difference.
Surgical procedure
Non-balloon group
Following successful induction of general anesthesia, the patient was positioned prone with chest bolsters. After C-arm fluoroscopic confirmation, a midline posterior incision was made centered over the osteotomy vertebra to expose the surgical levels. Pedicle screws were inserted into two vertebrae above and below the osteotomy site. Initial temporary stabilization was achieved by installing a unilateral pedicle screw-rod construct. The contralateral pedicle of the apical vertebra was then identified using a pedicle probe to determine the optimal entry point and trajectory. The pedicle entrance was appropriately enlarged, and conventional eggshell technique was performed using a high-speed burr under continuous saline irrigation. The bilateral transverse processes of the osteotomy vertebra were resected, followed by blunt subperiosteal dissection along their bases to expose the anterolateral vertebral body. The osteotomy length was measured and marked along the spinous process, centered at the target vertebra. Using an ultrasonic bone scalpel, the posterior elements including the spinous process, lamina, facet joints, and bilateral pedicle bases were resected (Figure 1(a) and (b)). The lateral cortex of bilateral pedicles was removed using a high-speed burr to widen the working channel. Subsequently, straight and angled curettes of various sizes were inserted into the vertebral body through the bilateral pedicle channels. During continuous curettage, the cancellous bone was gradually removed based on tactile feedback from the tip of the curette until a wedge-shaped cavity bordered by cortical bone was created. Care was taken to preserve the integrity of the anterior and lateral vertebral wall cortices to avoid injury to the great vessels anteriorly. The posterior vertebral wall was carefully impacted into the cancellous cavity using an L-shaped osteotome. Following completion of the decancellation and posterior wall management on one side, a pre-bent temporary rod was inserted into the screw heads on the same side to maintain temporary stability and prevent displacement during contralateral manipulation. The same steps of pedicle decancellation and posterior wall management were then performed on the contralateral side. After completing the bilateral osteotomy and posterior wall procedures, the temporary rod was removed. In coordination with the anesthesiologist, the surgical table was gradually extended to induce lumbar extension. Concurrently, manual compression was applied by the surgeon to gradually approximate and close the posterior margins of the osteotomy sites until the bilateral pedicle and lamina osteotomy surfaces were in firm contact. Satisfactory correction of the kyphotic deformity was confirmed at this point. After final instrumentation, a wake-up test was conducted. Absent lower extremity response necessitated either waiting or immediate intervention. Upon confirmation of normal motor function, the graft bed was prepared and morselized autogenous bone from the resected vertebra was used for posterolateral fusion. Finally, adequate hemostasis was achieved using absorbable flowable gelatin and gelatin sponge. A drain was placed, and the wound was closed in layers with application of a compressive dressing. Schematic diagram of surgical procedure. (a) Demonstrates the extent of pedicle subtraction osteotomy in the sagittal plane. (b) Illustrates the range of pedicle subtraction osteotomy in the axial plane. (c) Shows balloon dilation placement within the vertebral body following exposure of bilateral pedicle bases at the osteotomy vertebra. (d) Presents balloon dilation positioning within the vertebral body in the axial plane.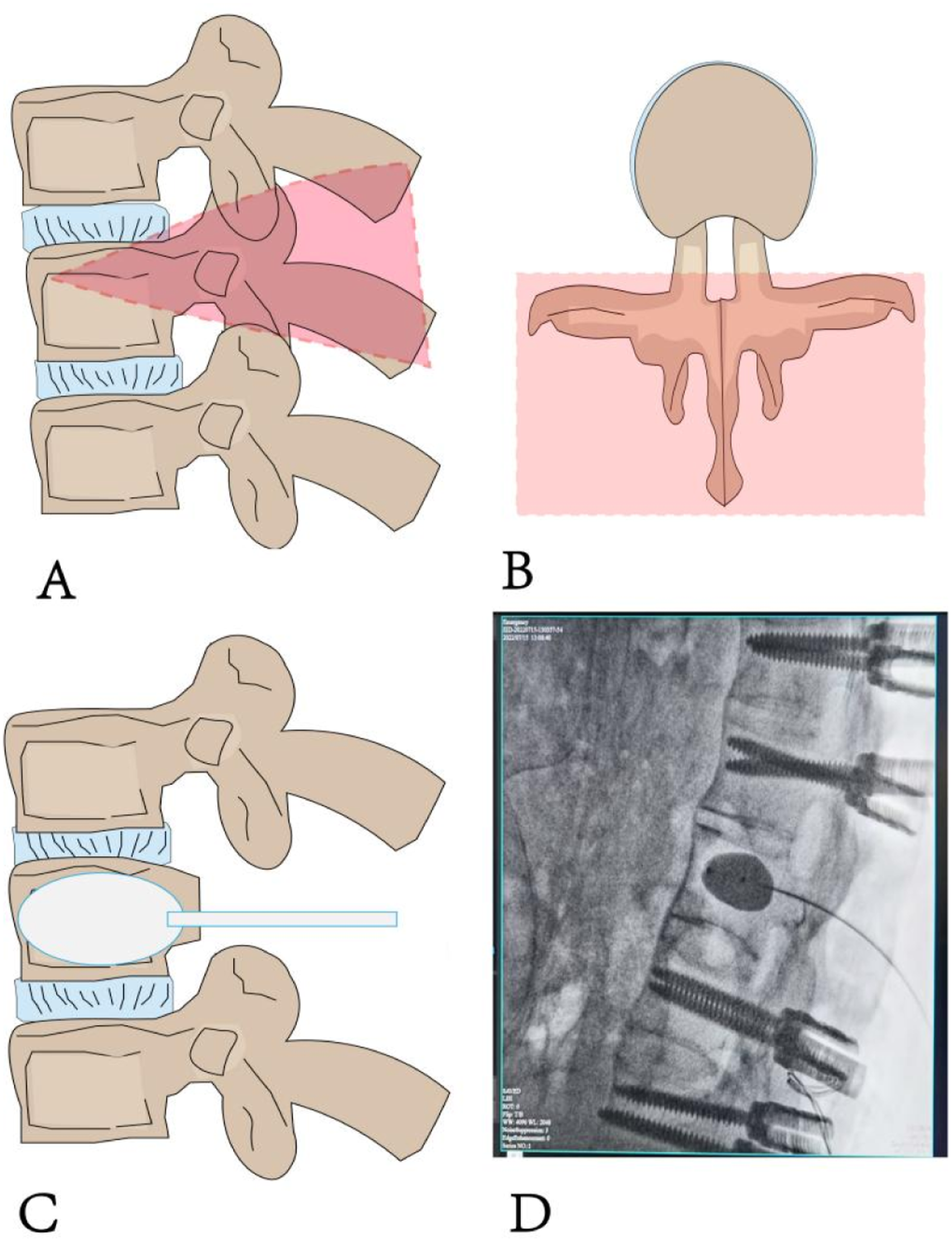
Balloon group
The exposure of the osteotomy vertebra and the resection of the posterior column of the spine, as well as the titanium rod internal fixation for osteotomy correction, are the same steps as those in the non-balloon group described above. Here, we provide a detailed description of the application of the intraoperative balloon expansion technique in the vertebral shellification process of pedicle subtraction osteotomy (PSO). After exposing the bilateral pedicle bases of the osteotomy vertebra, under direct visualization by the surgeon, the balloon is inserted along the osseous channel of one pedicle and positioned in the anteromedial part of the vertebral body, equidistant from the upper and lower endplates. Before inflating the balloon, all air must be evacuated from it. The inflation of the balloon should be carried out slowly. When the pressure reaches 50 psi, the inner core of the balloon is removed to continue the expansion. To avoid balloon rupture, the pressure should not exceed 300 psi in principle. The expandable balloon is deflated and removed when it contacts the cortical bone or endplate of the vertebral body or reaches its maximum volume. The same procedure is then repeated on the contralateral side (Figure 1(c) and (d)).
Postoperative management
All patients were managed postoperatively in accordance with the standardized enhanced recovery after surgery (ERAS) protocol established at our institution. Routine postoperative care included prophylactic antibiotics (typically cefazolin sodium for 24–48 h), nutritional support (e.g., human albumin), and neurotrophic agents (e.g., mecobalamin). Drain management followed a uniform criterion, with removal performed once the 24-h drainage volume was less than 50 mL. One week after surgery, the patient began ambulation and functional training under the protection of a thoracolumbar orthosis. The brace was required to be worn continuously for at least 3 months and was discontinued only after radiographic confirmation of solid bony fusion at the osteotomy site. Patients were advised to avoid strenuous activities and high-intensity physical exercise for at least 1 year postoperatively to prevent implant failure or loss of correction.
Evaluation indicators
Clinical assessment
The surgical time, intraoperative blood loss, perioperative complications, and length of hospital stay were recorded. The clinical symptoms of the patients were assessed using the Visual Analogue Scale (VAS) and the Oswestry Disability Index (ODI) questionnaire before surgery, at 1 week postoperatively, and at the final follow-up.
Imaging evaluation
All patients underwent regular postoperative outpatient follow-up. Standing full-spine posteroanterior and lateral radiographs or sagittal reconstructed CT images of the entire spine were obtained preoperatively, at 1 week postoperatively, and at final follow-up. Using specialized imaging software (Surgimap 2.3.0.1), radiographic parameters of the entire spine and pelvis were measured, including: (1) thoracolumbar kyphosis (TLK), defined as the angle between the superior endplate of T10 and inferior endplate of L2; (2) lumbar lordosis (LL), measured as the angle between the superior endplate of L1 and superior endplate of S1; (3) thoracic kyphosis (TK), calculated as the angle between the superior endplate of T1 and inferior endplate of T12; (4) sagittal vertical axis (SVA), representing the horizontal distance from the C7 plumb line to the posterosuperior corner of S1; and (5) pelvic tilt (PT), determined as the angle between the vertical reference line and the line connecting the midpoint of the S1 endplate to the femoral head axis.
Statistical analysis
Statistical analysis was performed using SPSS software (version 25.0; IBM Corp, Chicago, IL, USA). Continuous variables were expressed as mean ± standard deviation, while categorical data were reported as median values. Comparative analyses included paired t-tests and independent samples t-tests for continuous variables, with ANOVA employed for multiple group comparisons. Non-parametric Kruskal-Wallis H tests were utilized for analyzing categorical data distributions.
Results
Comparison of clinical outcomes between balloon group and non-balloon groups (vas, odi, operative time, intraoperative blood loss, and hospital stay).
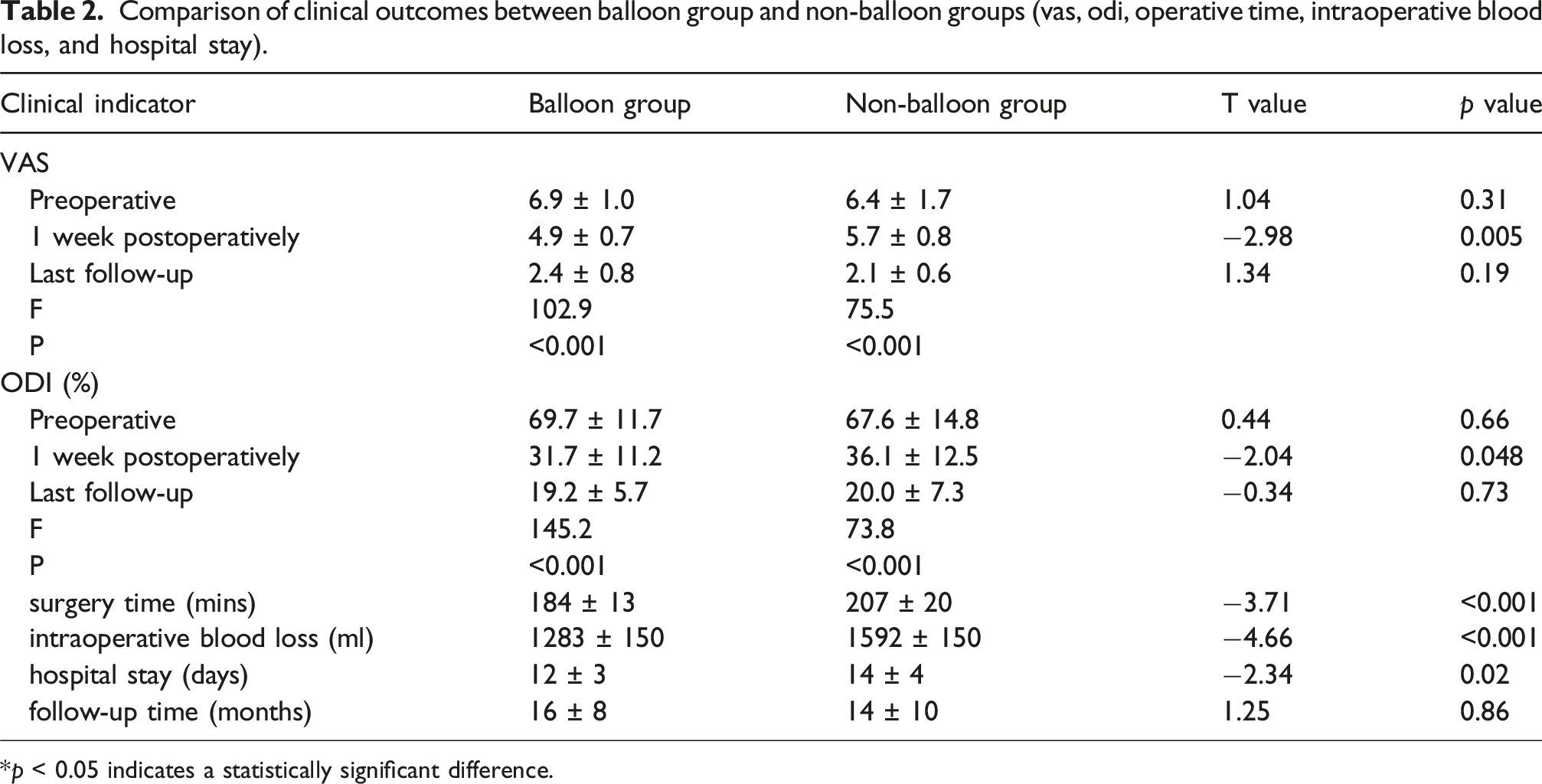
*p < 0.05 indicates a statistically significant difference.

Patient 1, male, 40 years. Recurrent low back pain and stiffness for over 10 years, aggravated with kyphotic deformity for 3 years and limited mobility for 6 months. (a1–a3) Preoperative full-length posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the spine. (b1–b3) Postoperative (1 week) full-length posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the spine. (c1–c3) Final follow-up posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the thoracolumbar spine.

Patient 3, male, 43 years. Recurrent low back pain and stiffness for 8 years, aggravated with kyphotic deformity for 2 years and limited mobility for 1 year. (a1–a3) Preoperative full-length posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the spine. (b1–b3) Postoperative (1 week) full-length posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the spine. (c1–c3) Final follow-up posteroanterior and lateral spinal radiographs, 3D CT reconstruction of the thoracolumbar spine.
Significant clinical improvements were observed in both groups, with VAS and ODI scores showing statistically significant enhancement at 1-week postoperation and final follow-up compared to preoperative values (all p < 0.05) (Table 2). Notably, the balloon-assisted group achieved better early outcomes with superior 1-week postoperative VAS (T = −2.98, p < 0.05) and ODI (T = −2.04, p < 0.05) scores (Table 2).
Comparison of imaging indicators (TLK, LL, TK, SVA, PT) between balloon group and non-balloon group.

*p < 0.05 indicates a statistically significant difference.
Discussion
Ankylosing spondylitis (AS) is characterized by excessive kyphosis of the thoracolumbar spine, which makes it difficult for patients to maintain a horizontal gaze while standing and to lie flat in bed. This condition impairs the patients’ ability to perform daily activities.10,11 Surgical correction should be considered for patients who fail to respond to conservative treatment or experience disease progression. Pedicle subtraction osteotomy (PSO) has become a widely adopted surgical technique for deformity correction. The procedure involves resection of posterior spinal elements followed by wedge-shaped osteotomy through the pedicles, extending to the anterior vertebral cortex. Subsequent posterior compression utilizes the intact anterior cortex as a hinge point to achieve deformity correction. 12 The complete closure of the osteotomy site, coupled with preserved supporting structures above and below, confers several advantages to PSO: enhanced stability, high fusion rates, maintained correction over time, effective restoration of lumbar lordosis, and minimal impact on anterior visceral structures. 13 However, PSO presents considerable technical demands and carries multiple potential complications, including neurological deficits, osteotomy-level dislocation, deep wound infections, and epidural hematoma. 14 In a 10-years follow-up study of 108 patients undergoing lumbar PSO, Buchowski JM reported neurological injuries in 12 cases (11.1%), with 3 patients (2.8%) sustaining permanent deficits. 7 Similarly, Park JS et al. documented osteotomy-level dislocation in 16 out of 53 AS patients (30.2%) following PSO for thoracolumbar kyphosis correction. 15
In patients with advanced ankylosing spondylitis (AS), the ossification of anterior longitudinal ligaments and osteophyte formation at adjacent intervertebral spaces significantly reduce spinal segmental flexibility and limit intervertebral distraction. When inadequate cancellous bone resection is performed at the osteotomy site, sole reliance on cantilever reduction techniques often fails to achieve proper wedge-shaped closure of the osteotomy gap, resulting in insufficient correction of local kyphosis. Excessive compression forces applied to adjacent pedicle screws in such cases may lead to anterior cortical fractures and screw loosening. 16 Conversely, over-resection of cancellous bone causes parallel collapse of the osteotomy vertebra, compromising sagittal plane correction. Due to these anatomical constraints, the correction angle achievable through single-level PSO is typically limited to 30°-40°to minimize neurological complications.6,17 This limitation is supported by clinical evidence from Mao Saihu et al.'s study of 102 AS patients undergoing single-level thoracolumbar PSO, which demonstrated significantly smaller correction angles in the ossified group (36° ± 7°) compared to the non-ossified group (42° ± 7°), with statistically significant differences (p < 0.05). 18
Osteoporosis, a prevalent comorbidity in ankylosing spondylitis (AS) with an incidence ranging from 19% to 62%, results from chronic inflammatory processes, prolonged glucocorticoid (GCs) use, vitamin D deficiency, and reduced physical activity.19,20 During the eggshell osteotomy procedure, the removal of cancellous bone from pedicles and vertebral bodies using curettes or high-speed drills often leads to substantial blood loss (reported between 1516 and 2984 ml across various studies), attributable to the vascular nature of cancellous bone and challenges in achieving hemostasis of the epidural venous plexus.21,22 Such significant hemorrhage may induce hemodynamic instability, potentially causing spinal cord ischemic dysfunction while increasing transfusion requirements and postoperative bleeding risks. 23 In pursuit of reduced operative blood loss and shorter surgical duration without compromising correction outcomes, researchers have developed several PSO modifications. Nicolas Plais et al. introduced a technique involving extensive laminectomy at the osteotomy level for spinal cord decompression, followed by sequential reaming of the pedicle at 25° to the axial plane for complete pedicle decancellation, and subsequent medial reorientation (55–60° to axial plane) to fracture the posterior and lateral walls. Their series of 14 patients demonstrated mean blood loss of 920 ± 350 mL with average kyphosis correction of 32°. 24 Similarly, Yang Yang’s team reported their modified eggshell technique in 17 thoracolumbar kyphosis cases, featuring bilateral transverse process resection with partial lateral vertebral wall splitting to enlarge the pedicular working corridor, facilitating cancellous bone evacuation and posterior element removal. This approach achieved correction from 64° ± 30° to 27° ± 20° at final follow-up, with mean intraoperative blood loss of 1573 mL. 25
Given the osteoporotic bone quality commonly observed in patients with AS, this study innovatively applied the balloon of the PKP technique through the vertebral pedicle into the vertebral body during osteotomy. The expanded balloon compresses the cancellous bone within the osteotomized vertebra, facilitating the formation of a sealed cavity more effectively than traditional eggshell techniques. This approach reduces intraoperative blood loss, partially restores the height of the affected vertebra, and contributes to a greater correction of the lumbar sagittal angle 26 (Figure 1). Compared to the conventional group, the balloon-assisted approach demonstrated several advantages: reduced operative time and intraoperative blood loss by minimizing cancellous bone removal, decreased early postoperative back pain (facilitating earlier rehabilitation), and shorter hospital stays. The radiographic outcomes showed no statistically significant differences between groups at both 1-week postoperative and final follow-up assessments. However, significant intergroup differences were observed in early clinical outcomes, including 1-week VAS scores (T = −2.98, p < 0.05), ODI scores (T = −2.04, p < 0.05), and length of hospitalization (T = −2.34, p < 0.05) (Table 2). These findings align with the results reported by Henri Salle et al. in their retrospective analysis of 102 thoracolumbar fracture cases. Henri Salle 27 conducted a study involving 102 patients with single-level traumatic thoracolumbar fractures treated with percutaneous posterior short-segment fixation (PPSF) combined with balloon kyphoplasty (BK). Radiographic evaluation demonstrated significant improvements in both spinal kyphosis correction and vertebral body height (VBH) restoration. The mean correction rate for kyphotic deformity reached 74.4% (95% CI 72.6% to 76.1%), while VBH restoration averaged 85.5% (95% CI 84.4% to 86.6%), with both parameters showing statistically significant improvement (p < 0.0001). These robust outcomes substantiate the clinical efficacy of balloon expansion technology in vertebral fracture reduction and spinal deformity correction.
The present study has several limitations that should be acknowledged. First,The sample size is relatively small, which may limit the statistical power and generalizability of the findings. Second, The follow-up period of 18.5 months is relatively short, and longer-term outcomes regarding implant integrity, correction maintenance, and functional status remain to be determined.
In conclusion, the application of balloon dilation technology in pedicle subtraction osteotomy for vertebral decancellation demonstrates significant clinical advantages, including reduced intraoperative blood loss, shorter operative duration, and enhanced procedural safety. These benefits position this technique as a valuable surgical approach worthy of broader adoption in the management of ankylosing spondylitis-associated thoracolumbar kyphotic deformities.
Footnotes
Acknowledgments
Thank you for all the support from the Changsha Central Hospital.
Ethical considerations
The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Consent for publication
All authors contributed to the article and approved the submitted version.
Author contributions
JHB,YXX contributed to conception and design of the study. JHB, YZH organized the databases. JHB performed the statistical analysis. JHB, YFW and LY wrote the first draft of the manuscript. JHB,JWS,LYwere involved in article revisions. All authors read and approved the final manuscript.
Funding
This study was supported by the Project of Changsha Central Hospital (grant number YNKY202511), Changsha Science and Technology Fund Project (kq2014023), Hunan Province Health Commission Research Program (D202304076350), Changsha Science and Technology Fund Project (kzd21081).
Declaration of conflicting interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.