
Abstract
Objectives
Closed suction drains are frequently used in the total knee arthroplasty (TKA) procedures for reducing pain, bruising edema and hematoma formation. Recent literature suggested no benefit of setting drains. The purposes of this study are to compare the outcomes between non-drain and drain groups, to identify the efficacy and safety of TKA without closed drainage, and to assess the prognosis of postoperative hematomas after TKA.
Materials and Methods
We retrospectively reviewed 901 patients with 933 knees, which performed primary total knee arthroplasty within 2 years. Ninety-one TKAs with drainage tube and 842 TKAs without setting drainage were enrolled in this study. The TKAs without drain were divided into the hematoma subgroup and the non-aspiration subgroup. Demographics, hematoma formation, anticoagulants use, perioperative hemoglobulin, and postoperative complications, were compared between these two groups.
Results
One knee of the drain group had cellulitis, and none developed hematoma and prosthetic joint infection. Ten TKAs developed prosthetic joint infection and 4 underwent surgical evacuation of a postoperative hematoma in the non-drain group. There was no significant relationship of postoperative complications between non-drain and drain groups. The hematoma subgroup had a significant higher incidence of PJI (p = 0.008) than the no aspiration subgroup.
Conclusions
Primary TKA performed without postoperative suction drain under the combination use of intravenous and intra-articular tranexamic acid can be advocated as a safe procedure. Postoperative hematoma formation after TKA without drainage revealed a significant higher risk of periprosthetic joint infection. Our study demonstrated the drain group revealed lower incidence of hematoma formation, periprosthetic joint infection and cellulitis than the non-drain group, which should be interpreted with caution and may highlight the importance of careful monitoring for adverse outcomes when drainage is not used after TKA.
Introduction
Total knee arthroplasty (TKA) is an effective treatment for end-stage osteoarthritis of knee, and it can achieve excellent functional and clinical outcomes. However, TKA can be associated with early complications, such as allergic reaction, hematoma formation, thromboembolic events, wound infection and intraoperative fractures, and late complications including aseptic loosening, joint instability, and periprosthetic joint infection (PJI).1,2 Closed suction drains are frequently used in the TKA procedures for reducing pain and bruising edema, minimizing hematoma formation, avoiding wound dehiscence, and decreasing the incidence of infection.1–6 The disadvantages of the setting drain were reported to have a greater blood loss, a higher incidence of blood transfusion, the possibility of drain dysfunction and prolonged hospital stay.4,7–11 Many studies have elucidated the relationship between postoperative hematoma formation and wound infections and suggested that reducing postoperative hematoma formation may prevent PJI.1,12–14
In the past decade, some literature suggested no benefit of setting drains following TKA procedures, which indicated that the routine use of closed drainage systems may not significantly impact the incidence of PJI and could potentially increase the risk of infection.1,5,14–17 Intra-articular and intravenous tranexamic acid (TXA) has been wildly used in the TKA procedures for reducing postoperative bleeding and blood transfusion, which made suction drainage unnecessary after TKA surgery.15,18–21 Thus, most of orthopedic surgeons in our institution did not use drains in TKA procedures under the perioperative TXA administration.
The purposes of this study are to identify the efficacy and safety of performing TKA without closed drainage systems, to compare the outcomes between non-drain group and drain group in patients with primary TKA, and to assess the prognosis of postoperative TKA hematoma in non-drain group.
Materials and methods
Study design
This retrospective study was approved by the Ethics Committee and Institutional Review Board of Chang Gung Medical Foundation (202201816B0) and conformed to the Declaration of Helsinki. The patient informed consent was waived by IRB, and all methods were carried out in accordance with relevant guidelines and regulations.
We retrospectively reviewed 901 patients with 933 knees, which were performed primary total knee arthroplasty from January 2021 to December 2022 in Chia-Yi Chang Gung Memorial Hospital. Thirty-two patients performed bilateral TKA, and 869 patients performed unilateral TKA in our institution within 2 years. Ninety-one TKAs with drainage tube and 842 TKAs without setting drainage were enrolled in this study.
All patients underwent cemented TKA based on standardized procedures in a clean laminar-flow environment and quality assurance of operating room with pneumatic tourniquet use prior to the skin incision. All patients received preoperative prophylactic antibiotics and intravenous TXA within half an hour before inflating tourniquet. Intra-articular TXA administrations in TKAs without setting drainage were performed after wound closure through the suprapatellar space before tourniquet release. After applying aseptic compression dressing and an elastic bandage, the tourniquet deflated. In TKA patients with a drainage tube, the tourniquet was deflated after cementing the components, and the bleeders were cauterized by electric coagulation. Then, one drainage tube was placed in the articular cavity and the wound was closed by layers. The TXA application was performed through the drain tube which was clamped off for a period of 3 h after surgery to ensure the effect of TXA. The drainage tube was placed postoperatively and removed within 2 days.
Peri-operative antibiotic prophylaxis consisted of a single intravenous dose of 1 g of cefazolin before skin incision and 3 doses of 1 g of cefazolin after surgery. Hemoglobin levels were assessed on the first day after surgery. Those patients who had preoperative anticoagulants usage, such as aspirin, clopidogrel, rivaroxaban or warfarin, were given the next day after TKA, and the anticoagulants were investigated for the relation with postoperative hematoma. At the postoperative follow-up, if the patient presented discomfortable knee due to moderate swelling and ecchymosis, most surgeons observed by conservative treatment; however, some surgeons perform hematoma aspiration. If the patient complaint severe pain and the knee joint revealed severe swollen with tender, progressive hematoma formation was suspected and emergent arthrotomy was performed.
We used the following inclusion criteria for this study: (1) The TKA patients with setting drainage were classified as the drain group. (2) The TKA patients without setting drain were classified as the non-drain group. (3) When the patient of non-drain group had performed hematoma aspiration or surgical removal of hematoma due to severe swollen and ecchymosis within 30 days after TKA even at ward or outpatient clinic, the patient was enrolled in the postoperative hematoma subgroup. (4) In cases of clinical signs with suspicion of hematoma formation such as redness, ecchymosis and knee swelling, the patient who used ice application with bandage compression and did not received aspiration or surgery finally was included in the non-aspiration subgroup.
Clinical assessment
All patients were reviewed medical records and followed for hematoma and subsequent PJI for at least 1 year after primary TKA. According to the usage of drain tube, the TKAs were divided into non-drain group and drain group. Those TKAs without setting drain tube were divided into the hematoma subgroup and the non-aspiration subgroup.
Demographic data, such as gender, age, usage of anticoagulants, perioperative hemoglobin, hematoma formation, and postoperative complications, were compared between non-drain group and drain groups. Age, gender, anticoagulants use after TKA, doses of intravenous and intra-articular TXA, hemoglobin decrease, hematoma removal, PJI, platelet counts and international normalize ratio (INR) were compared between postoperative hematoma and non-aspiration subgroups. Arthrotomy for hematoma removal and prosthetic joint infection (PJI) were confirmed by surgical intervention. The patients with the diagnosis of cellulitis were admitted for intravenous antibiotics without surgery.
Statistical analysis
Statistical analyses were performed with the use of Statistical Product and Service Solutions (SPSS) Version 18.0 statistical software (SPSS, Chicago, Illinois). We used the Fisher exact test for categorical variables and independent t-tests for continuous variables to examine significant relationships of postoperative complications between non-drain group versus drain group and hematoma versus non-aspiration subgroups. To determine the independent association between those groups and postoperative complications, a multivariable logistic regression model was constructed. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. A post hoc power analysis was performed for the comparison of prosthetic joint infection between groups. A value of p < 0.05 was considered to indicate statistical significance.
Results
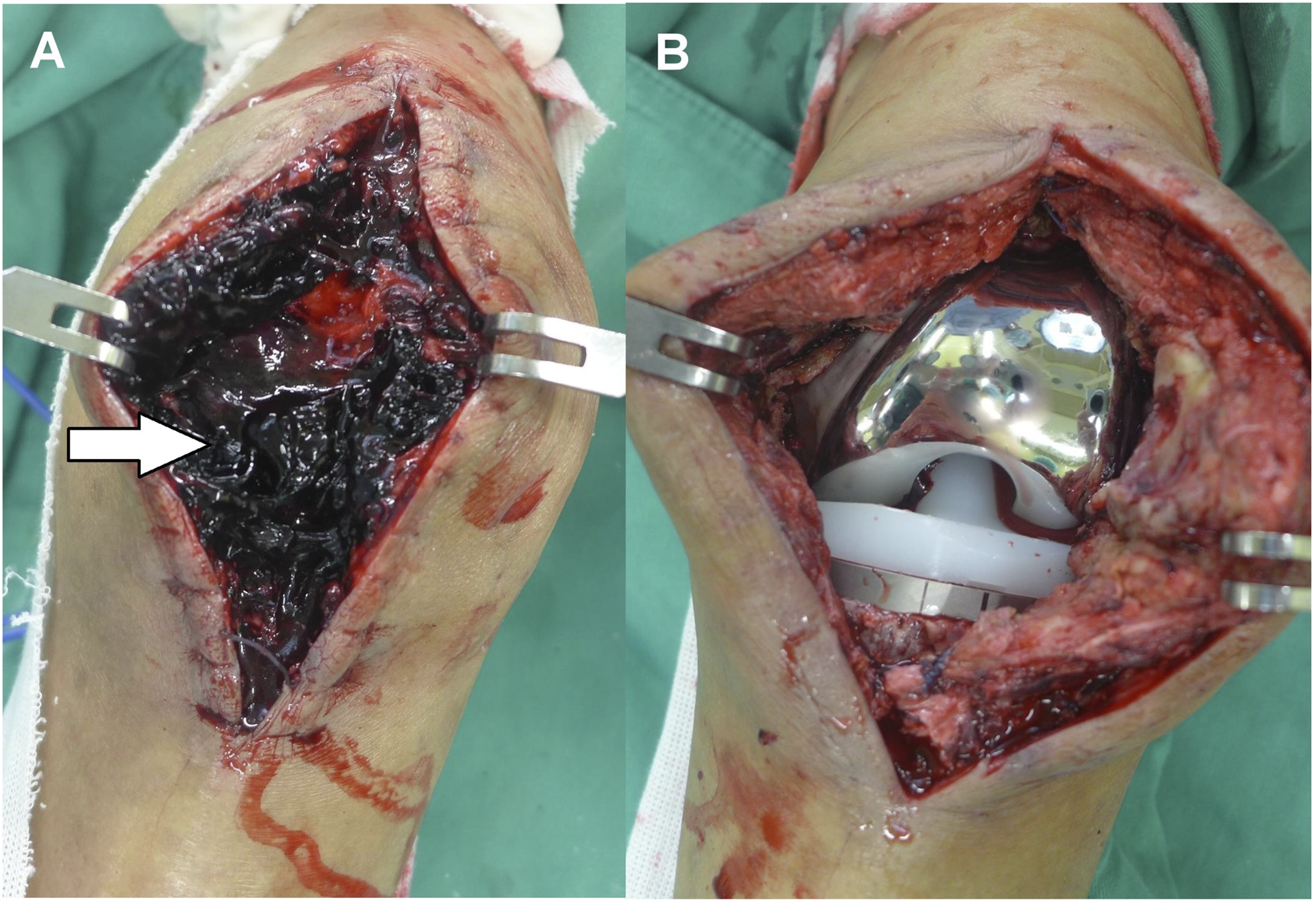
Ninety-one TKAs with a drain tube were included in the drain group and 842 TKAs without setting drain tube were enrolled in the non-drain group (Figure 1). One TKA of the drain group had cellulitis, and none developed hematoma and prosthetic joint infection. In the non-drain group, 10 TKAs developed PJI, 4 performed removal of hematoma (Figures 2 and 3), and 6 were diagnosed as cellulitis. There were no significant relationships of age, gender, anticoagulants use, hemoglobin decrease, and postoperative complications between non-drain group and drain groups (Table 1). Flow chart of the TKA patients. A 64 year-old female with a history of diabete mellitus and hypertension had right knee pain and swelling on the second day after TKA without setting drain. She did not use anticoagulants after TKA; however, she complaint severe knee pain and the skin revealed progressive ecchymosis and swollen on the 2nd day after TKA. (a) She was performed arthrotomy immediately when the severe hematoma formation was diagnosed, and a lot of blood clots were found in the knee joint (white arrow). (b) After removal of hematoma, the suction drain was set. The patient did not present recurrent hematoma and infection after 3-months follow-up. A 72 year-old male with a history of hypertension and fondaparinux use after TKA without drain had performed 3 times of aspirating hematoma in the outpatient clinic. (a) (b) He was observed the patella slip out the groove with severe pain and swelling on the 34th day, and the knee merchant radiographic view showed increased patellar tilt angle (white arrow). He was performed arthrotomy immediately under the impression of hematoma formation. (c) Vastus medialis rupture and hematoma were noted (black arrow). After performing removal of heamtoma and muscle repair, the patient did not have hematoma formation and PJI after 6-months follow-up. Comparison between the non-drain group and drain group for characteristics and laboratory data at the final follow-up.


Comparison Between the hematoma subgroup and non-aspiration subgroup for charcteristics and laboratory data at the final follow-up.
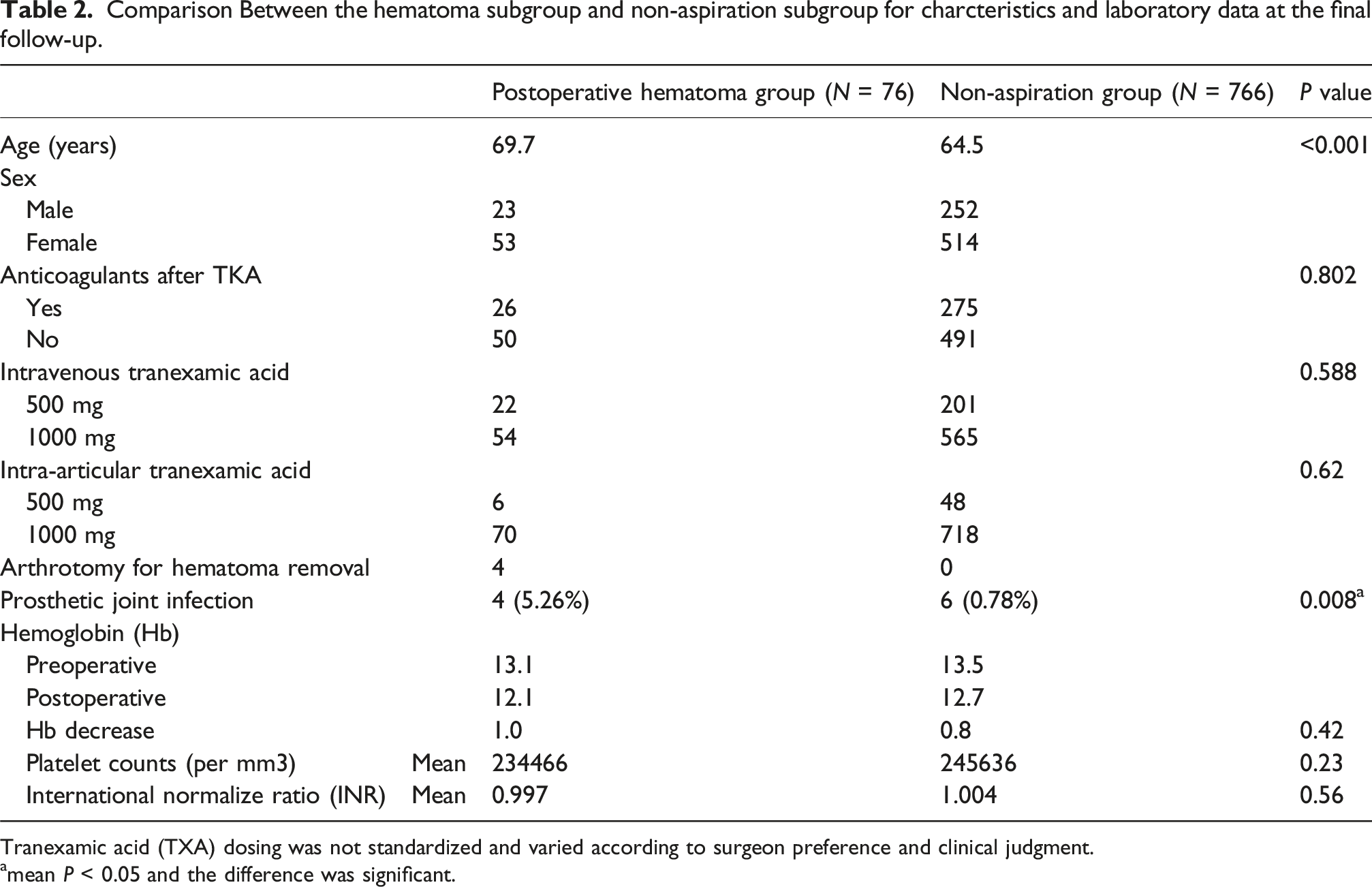
Tranexamic acid (TXA) dosing was not standardized and varied according to surgeon preference and clinical judgment.
amean P < 0.05 and the difference was significant.
Multivariate logistic regression analysis for risk factors associated with postoperative complications after TKA.

ORs, odds ratios; CIs, confidence intervals.
amean P < 0.05 and the difference was significant.
Post-hoc power analysis for prosthetic joint infection.

The identified pathogens of the patients of PJI in the hematoma subgroup were methicillin-sensitive Staphylococcus aureus (MSSA) and coagulase-negative Staphylococcus. The pathogens in non-aspiration subgroup with PJI were MSSA in 2 patients, Bacillus cereus in one, Staphylococcus epidermis in one, and no bacterial growth in two.
Discussion
Many literature have demonstrated that the use of postoperative close suction drainage in patients undergoing primary TKA was associated with higher blood loss and transfusion rates; however, the use of intravenous and intra-articular TXA proved to be effective and safe to prevent blood loss and reduction of transfusion rate.11,18,19,21–24 Several studies revealed no significant differences in blood loss, dressing soakage, swelling, range of motion, or infection rates between the drain and non-drain groups under the TXA administration, and suggested it was not necessary for routine use of closed suction drain.1,3,15,18 Although 20 cases (2.4%) of 842 TKAs without setting drain tube developed complications in this study, we considered that the routine use of intravenous and intra-articular TXA injection without postoperative drain following TKA procedures revealed acceptable safety and favorable clinical outcomes.
In the past decade, numerous literature did not support the routine use of closed suction drainage after TKA which might be associated with blood loss, infection and knee stiffness.4,5 Some studies also found that closed drainage systems may not significantly impact the incidence of PJI; however, it could potentially increase the risk of infection.1,5,14–17 Although the TKA without use of suction drain can be advocated as a safe procedure under the combination use of intravenous and intra-articular TXA, we did not find significant decrease of hemoglobin and prolonged hospital stay in the drain group. In this retrospective cohort, the use of postoperative drains did not demonstrate a meaningful association with postoperative complications. Although the crude complication rate appeared numerically lower in the drain group (1.1% vs 2.4%), the confidence intervals were wide and largely overlapping, indicating no statistically meaningful differences between groups. Otherwise, multivariable regression analysis did not demonstrate an independent association between drain use and postoperative complications, the observed trends should not be interpreted as evidence of a protective effect of drainage. Rather, these findings indicate that drain use was not significantly associated with improved or worsened outcomes after adjustment for confounding factors. Similarly, individual complications such as prosthetic joint infection, surgical removal of hematoma, and cellulitis occurred at very low frequencies. However, we demonstrated the drain group revealed lower incidence of hematoma formation, periprosthetic joint infection and cellulitis than the non-drain group, which may alert the surgeons to pay attention to the adverse effects without use of drain after TKA.
Postoperative hematoma after primary TKA may increase the local pressure to compromise skin viability, cause pain and lead to persistent drainage.12,25 Some studies have shown that hematoma formation was associated with a higher chance of re-operation following TKA, and the hematoma could provide a favorable medium for bacteria to adhere and multiply which may lead to periprosthetic joint infection.12,25,26 In this study, 76 of 842 (9%) TKAs without use of close drainage system developed postoperative hematoma, and eight patient (10.5%) performed surgical intervention: 4 evacuated hematoma and 4 developed PJI. Although no hematoma was formally documented in the remaining 766 TKAs, we observed some surgeons did not perform aspiration even though the knee revealed ecchymosis and moderate swollen (Figure 4). Based on univariate analysis, multivariate logistic regression and post-hoc power analyses, postoperative hematoma was strongly associated with an increased risk of PJI. Therefore, we suggested timely aspiration the hematoma when the knee presented severe ecchymosis and swollen either during hospitalization or in the outpatient clinic which could decrease the discomfort and potentially reduce the risk of infection. Overall, our findings highlight that minimizing postoperative hematoma formation is an important issue in reducing the risk of deep infection and undergoing subsequent major surgery in patients undergoing primary TKA without setting postoperative drainage. (a) (b) The knee revealed ecchymosis and swelling on the secondary day after TKA. (c) After ice packing and use of intravenous TXA, ecchymosis and swelling subsided on the seventh day. This patient did not develop progressive hematoma or infection.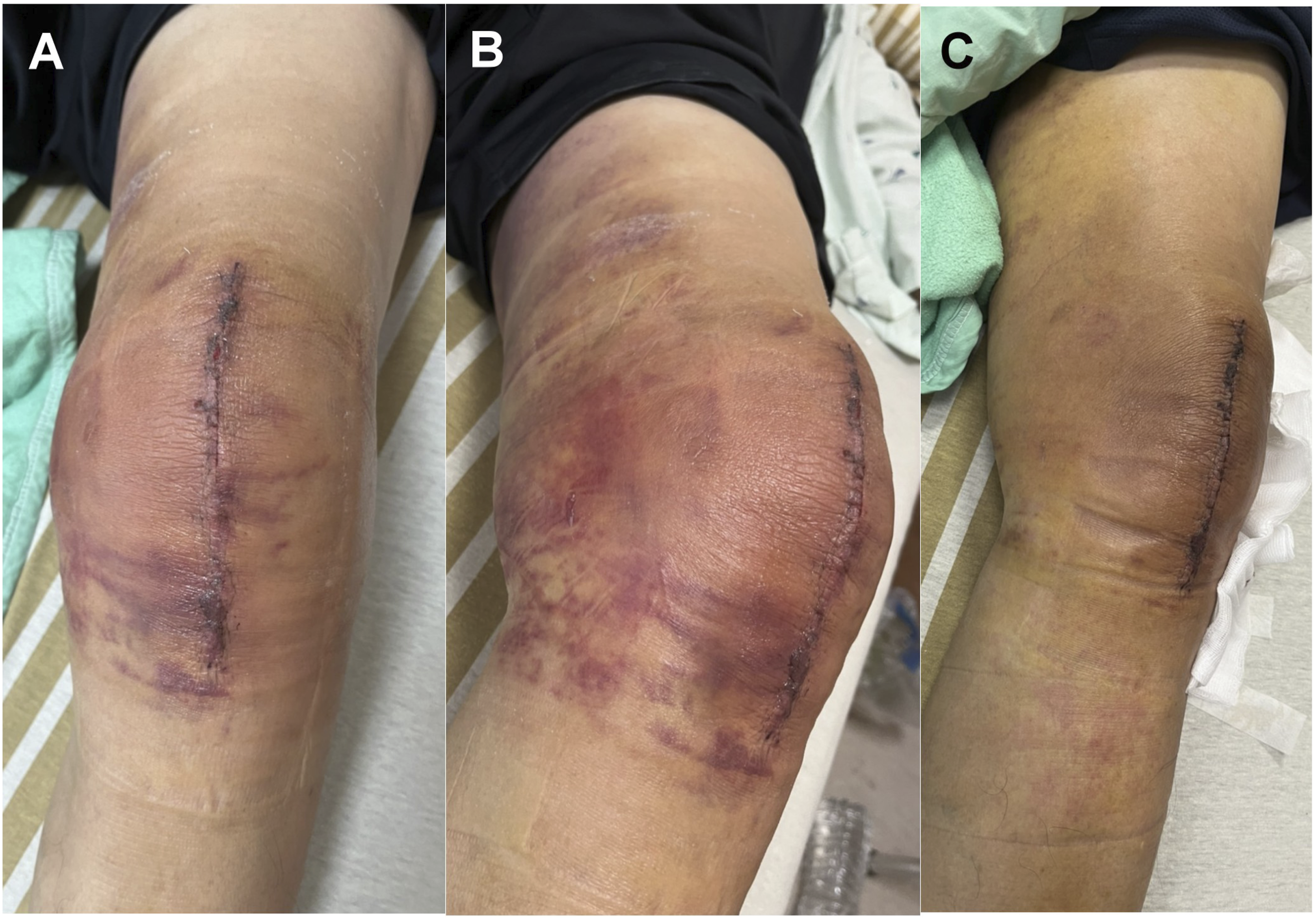
This study has several limitations. First, the retrospective nature of this study is inherently subject to unmeasured confounding. Variations in surgical technique, tranexamic acid dosage, and postoperative management across different surgeons may have influenced clinical outcomes and result in the risk of blood loss and hematoma formation. Although multivariable regression analysis was performed to adjust for measured confounders, residual confounding related to surgeon-specific practices cannot be completely excluded. Therefore, the results should be interpreted with caution, and prospective studies with standardized protocols are warranted to further validate our findings. Second, the doses of intravenous and intra-articular TXA were not standardized and these were given by surgeons’ preference which may may affect the postoperative bleeding. Third, we did not monitor the length of anticoagulants usage after TKA which may induce the recurrent bleeding. Fourth, The drain group was considerably smaller than the non-drain group (91 vs 842 patients), which inevitably limited the statistical power to detect differences in rare outcomes such as prosthetic joint infection. Although post-hoc power analysis was performed and acknowledged, the observed imbalance between groups should be carefully considered when interpreting the infection-related results. Consequently, the absence of statistical significance for certain outcomes does not necessarily indicate equivalence between groups but may reflect insufficient power due to the low event rate. Final important limitation is the heterogeneity in the definition of postoperative hematoma. In this study, hematomas managed with aspiration were grouped together with those requiring surgical arthrotomy, which may represent clinically distinct entities with different severities and risk profiles. Although this approach was chosen to ensure sufficient event numbers for statistical analysis, it may have introduced clinical heterogeneity and potentially diluted outcome-specific associations.
Conclusion
Primary TKA performed without postoperative suction drain under the combination use of intravenous and intra-articular TXA can be advocated as a safe procedure. Postoperative hematoma formation after TKA without drainage revealed a significant higher risk for arthrotomy and periprosthetic joint infection. Based on multivariable analysis, no independent protective or harmful effect of drain use on postoperative complications was identified. Our study demonstrated the drain group revealed lower incidence of hematoma formation, periprosthetic joint infection and cellulitis than the non-drain group, which should be interpreted with caution and may highlight the importance of careful monitoring for adverse outcomes when drainage is not used after TKA.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request