
Abstract
We aimed to systematically compare the clinical and functional outcomes between unicompartmental knee arthroplasty (UKA) and high tibial osteotomy (HTO) for the treatment of medial knee osteoarthritis (KOA). Literatures were searched from PubMed, EMBASE, the Cochrane library, Wanfang DATA, China National Knowledge Infrastructure (CNKI) and SinoMed database until December 2020. Studies comparing postoperative clinical and functional outcomes of UKA versus HTO were included. Totally, 38 studies were included, including 2368 patients with 2393 knees in HTO group and 6536 patients with 6571 knees in UKA group. There was significant difference in postoperative pain, revision rate, complications, and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score between HTO and UKA groups (p < 0.05). No significant difference was found in excellent/good surgical results, Lysholm, Hospital for Special Surgery (HSS) score, Knee Society Knee (KSS) score, knee and function score of Knee Society (KSFS) score and Tegner score between these two groups (p > 0.05). UKA produced less postoperative pain, less complications and superior WOMAC score, whereas HTO offered extended range of motion (ROM) and less revision rate.
Keywords
Introduction
Knee osteoarthritis (KOA) is the common chronic joint disorder, which is generally characterized by the knee articular cartilage degeneration and the subsequent bone-to-bone wearing predominantly in the medial compartment. 1 Medial KOA may result from knee alignment disorders or injuries that damages the cartilage and overloads the medial tibiofemoral compartment. 2 Knee malalignment has been suggested as an important biomechanical risk factor in KOA progression and declines in physical function.3,4 Both high tibial osteotomy (HTO) and unicompartmental knee arthroplasty (UKA) are most frequently used medial KOA joint surgeries. Both types can improve knee function, reduce pain, slow knee deterioration and possibly delay the need for total knee replacement surgery. 5 Classically, the surgical indication of two types operations for medial KOA is well defined. HTO is particularly used in young and active patients, while UKA is the preferred treatment option for older patients with moderate or severe osteoarthritis.6–8 Today, the inclusion criteria have been greatly expanded with improvements in surgical techniques, implant design and modern instruments.9–11
HTO is a surgical procedure providing an offloading of the damaged medial cartilage by realignment of the knee joint and correcting the varus deformity. Patients receiving HTO can benefit from natural knee joint preservation and almost unaffected physical loading, which can delay or prevent the need for a partial or total knee replacement.8,12 Opening-wedge HTO (OWHTO) and closing-wedge HTO (CWHTO) are the two commonly used HTO procedures. 13 The choice of the osteotomy technique depends on the degree and location of knee malalignment and the experience of the surgeon. UKA is an alternative procedure to total knee replacement. In UKA, only the affected degenerative compartment of the knee is resurfaced and replaced with an implant prosthesis, while the nonaffected compartment is preserved. UKA allows knee bone stock and ligaments sparing and offers patients a less invasive procedure with excellent pain relief and faster recovery. 14
To date, several meta-analyses have directly compared HTO and UKA methods in patients with medial KOA.15–19 However, the comparative studies4,20 and meta-analyses have showed conflicting conclusions. The purpose of this study was to compare the clinical and functional outcomes of UKA versus HTO for teh treatment of medial KOA.
Materials and methods
Literature search
According to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline, databases including PubMed, EMBASE, the Cochrane library, Wanfang DATA, China National Knowledge Infrastructure (CNKI) and SinoMed were electronically searched for studies published before December 2020.
All analyses were based on previously published studies, so no ethical approval and patient consent are required.
Eligibility criteria
The inclusion criteria included: (1) patients were diagnosed with medial KOA; (2) original studies directly compared HTO with UKA for the treatment of medial KOA and reported at least one of function results (e.g., knee function score, range of motion [ROM], femorotibial angle [FTA]), revision incidence, complications (e.g., infection, thrombosis, and pain); (3) study type: both randomized controlled trials (RCTs) and nonrandomized controlled trials (non-RCTs) were considered; (4) language was limited to English or Chinese.
Search strategy
We started systematic search from the databases of PubMed, EMBASE, the Cochrane library, Wanfang DATA, CNKI and SinoMed from available papers in literature up to December 2020 for potentially eligible studies.
For the literature search, we used the medical subject heading (MeSH) term of ‘Osteoarthritis,” “Osteoarthritis, Knee,” and “Arthroplasty, Replacement, Knee,” and “High tibial osteotomy” “Unicompartmental,” as well as all key words corresponding to these MeSh terms.
Data extraction and quality assessment
The selection and inclusion of studies were performed in two stages by two independent authors (** and **). This included the screening of titles/abstracts followed by the full texts. Disagreements between the two authors were resolved by a third authors (**). The basic characteristics of the data from included studies consisted of names of authors, publication year, study design, country, sample size, mean age, female percentage, prosthesis properties, outcomes, follow-up time and radiographic outcomes.
We assessed the risk of bias in the RCTs using the Cochrane risk of bias tool to determine whether biases might affect the results. 21 The risk of bias in nonrandomized studies were assessed using the Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I) assessment tool. 22
Statistical analysis
The odds ratio (OR) and the corresponding 95% confidence interval (CI) was used to express the estimates of dichotomous outcomes. The estimates of continuous outcomes were expressed by using mean difference (MD) and the corresponding 95% CI. In all cases, p values <0.05 were considered statistically significant. Sensitivity analysis was conducted to obtain a solid conclusion and to evaluate the stability of the pooled results.
Cochran’s Q statistic 23 and Higgin’s inconsistency index 24 were used to assess the statistical heterogeneity among studies. Significant statistical heterogeneity was considered if I2 >50% and p < 0.1, then a random-effects model was used for meta-analysis. On the contrary, a fixed-effects model was selected if I2 ≤50% and p > 0.1. Naunyn Schmied. Arch. Exp. Pathol. Pharmakol. 5, S38). In addition, sensitivity analyses were performed according to the quality of the included studies by only studies assessed as moderate or high were included and pooled. Further sensitivity analyses were performed to identify individual study effects on pooled results and test the reliability of results by introducing leave-one-out strategy. All of the statistical analyses were performed using statistics and data (STATA) SE 14.0 software (StataCorp, College Station, Texas, USA).
Results
Study selection and characteristics of included studies
Totally, 252 relevant publications were initially retrieved. Duplicated documents, studies on irrelevant disease or intervention, case report or case series, meta or review articles, and documents of comments, protocols, thesis and surveys were subsequently removed. In addition, 16 articles were not published in English or Chinese, and the full text of four articles could not be obtained. After the screening, 51 articles were selected and assessed thoroughly. Among them, 13 articles were excluded because of insufficient data. Finally, 38 articles met the criteria were included for this meta-analysis. The eligible study selection process was shown in Figure 1. The basic characteristics of the selected 38 comparative studies were summarized in Table 1. A total of 2368 medial KOA patients with 2393 knees received HTO and 6516 patients with 6551 knees received UKA. There were six RCT studies, and the rest were all retrospectively observational studies. The mean age of the patients ranged from 43 to 77. The follow-up time ranged from 8.5 ± 1.8 months to 434.4 ± 4.8 months. Flowchart of the search process of our study. Characteristics of the included studies. HTO, high tibial osteotomy; UKA, unicompartmental knee arthroplasty; OWHTO, opening wedge high tibial osteotomy; CWHTO, closing wedge high tibial osteotomy; VAS, Visual Analogue Scale; BOA, British Orthopaedic Association score; PROM, postoperative range of motion; KSS, Knee Society Score; HSS score, the Hospital for Special Surgery score; ROM, range of motion; WOMAC, The Western Ontario and McMaster Universities; KOOS, Knee Osteoarthritis Outcomes Score; UCLA, UCLA Activity Score; KSS, American Knee Society Knee Score; KSFS, The knee and function score of Knee Society; IKDC, The International Knee Documentation Committee; RCS, retrospective comparative study; RCT, randomized controlled trial.

Quality assessment
Quality assessment of included studies.

The other included studies were all retrospective observational studies with inherent bias including confounding factors, selection bias, missing data and other bias in the design and implementation of results. Overall, nine studies had low bias, 20 studies presented moderate bias, and two studies showed serious bias.
Meta-analysis of clinical outcomes
Lysholm score
Twelve studies, including 361 patients with 361 knees in the HTO group and 474 patients with 474 knees in the UKA group, reported Lysholm score. Pooled result revealed no significant difference between the two groups (MD: −1.086, 95% CI: −2.219 to 0.046, p = 0.06; I2 = 69.6%) (Figure 2 and Table 3). Forest plots of functional results. Result of the meta-analysis. VAS, Visual Analogue Scale; HSS, Hospital for Special Surgery; WOMAC, The Western Ontario and McMaster Universities; ROM, range of motion; OR, odds ratio; MD, mean difference; CI, confidence interval.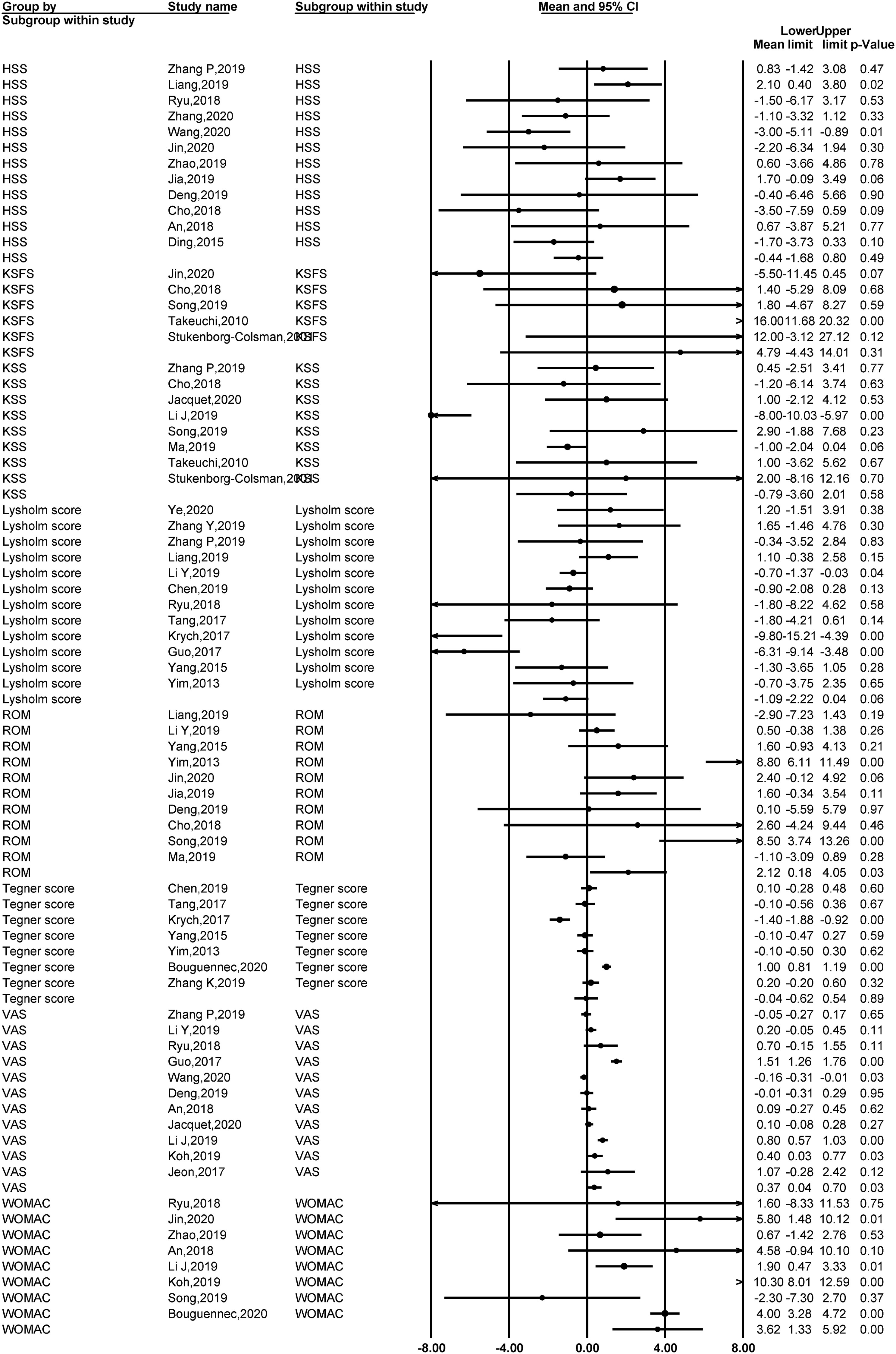

Hospital for special surgery score
Hospital for Special Surgery (HSS) score was assessed in twelve studies, including 462 patients with 467 knees in the HTO group and 441 patients with 446 knees in the UKA group, and pooled result suggested no significant difference between the two groups (MD: −0.433, 95% CI: −1.670 to 0.803), p = 0.492; I2 = 55.9%) (Figure 2 and Table 3).
Visual analogue scale
Eleven studies reported the data on Visual Analogue Scale (VAS), including 378 patients with 378 knees in the HTO group and 409 patients with 409 knees in the UKA group, and pooled result suggested that UKA was significantly associated with less pain compared to HTO (MD: 0.371, 95% CI: 0.04 to 0.702, p = 0.028; I2 = 93.9%) (Figure 2 and Table 3).
Range of motion score
Ten studies analyzed range of motion (ROM) score, including 399 patients with 408 knees in the HTO group and 351 patients with 369 knees in the UKA group. Pooled result revealed better flexion and extended ROM in the HTO group when compared to the UKA group (MD: 2.114, 95% CI: 0.176 to 4.052, p = 0.033; I2 = 82.3%) (Figure 2 and Table 3).
The Western Ontario and McMaster Universities score
Eight studies reported the data on the Western Ontario and McMaster Universities (WOMAC) score, including 827 patients with 827 knees in the HTO group and 624 patients with 624 knees in the UKA group, and the pooled result showed a significantly higher WOMAC score in the UKA group compared to the HTO group (MD: 3.627, 95% CI: 1.333 to 5.921, p = 0.002; I2 = 86.5%) (Figure 2 and Table 3).
American knee society knee score
Totally, eight studies reported the American Knee Society Knee (KSS) score, including 319 patients with 331 knees in the HTO group and 262 patients with 294 knees in the UKA group, and pooled result suggested that there was no significant difference between the two groups (MD: −0.801, 95% CI: −3.606 to 2.004, p = 0.576; I2 = 85.3%) (Figure 2 and Table 3).
Tegner score
Seven studies assessed Tegner score, including 671 patients with 671 knees in the HTO group and 591 patients with 591 knees in the UKA group, and pooled result showed no significant difference between the two groups (MD: −0.042, 95% CI: −0.624 to 0.540), p = 0.887; I2 = 94.6%) (Figure 2 and Table 3).
The knee and function score of knee society
Five studies reported the data on the knee and function score of Knee Society (KSFS), including 200 patients with 206 knees in the HTO group and 180 patients with 197 knees in the UKA group, and pooled result revealed no significant difference between the two groups (MD: 4.787, 95% CI: −4.435 to 14.009, p = 0.309; I2 = 89.5%) (Figure 2 and Table 3).
Rate of excellent and good
The analysis of seven studies including 296 patients with 312 knees in the HTO group and 224 patients with 241 knees in the UKA group yielded no statistically significant difference between the two groups regarding excellent/good results (OR: 0.88, 95% CI: 0.68 to 1.14, p = 0.338; I2 = 0%) (Figure 3 and Table 3). Forest plots of clinical results.
Complications
Generally, more complications were noted after performing HTO with significant difference between the two groups (OR: 1.42, 95% CI: 1.05 to 1.93, p = 0.024; I2 = 0%) based on the analysis on 910 HTO patients with 916 knees and 691 UKA patients with 708 knees (Figure 3 and Table 3).
Revision rate
Nine studies reported revision rates, including 1320 patients with 1323 knees in the HTO group and 5556 patients with 5570 knees in the UKA group, and the pooled data analysis showed no significant difference between the two groups (OR: 0.97, 95% CI: 0.78 to 1.19, p = 0.737; I2 = 70.1%) (Figure 3 and Table 3). Considering the fact that some of the included studies had a short follow-up period, thereby inevitably affecting the reliability of the data in terms of revision rate. Therefore, we further compared the revision rates between the two groups by including only studies with follow-up period of more than 60 months, and pooled result suggested that HTO was associated with significantly lower revision rate as compared with UKA (OR: 0.54, 95% CI: 0.28 to 0.79, p < 0.001, I2 = 0.1%).
Sensitivity analysis
We then conducted sensitivity analyses according to the quality of the included studies. As showed in Supplementary Figures 1 and 2, only studies assessed as moderate or high were included and pooled. The results of clinical outcomes were comparable with the overall analyses of all studies included except for the pooled results of VAS, which was not significant with MD as 0.52 (95% CI: −0.04 to 1.09, p = 0.07, as shown in Supplementary Figure 1.
The sensitivity analysis based on the leave-one-out strategy suggested that the results were robust (Supplementary Figure 3A-K).
Publication bias
There was no significant publication bias when assessing funnel plots of Lysholm, score, HSS score, VAS score, ROM score, and complications (Figure 4(a)–(e), supplementary Table 1). All p values for Begg’s test were greater than 0.05 (supplementary Table 1). Funnel plot of (a) Lysholm score; (b) HSS score; (c) VAS; (d) ROM score; and (e) Complications. HSS, the Hospital for Special Surgery; VAS, Visual Analogue Scale; ROM, range of motion.
Discussion
There was significant difference in VAS score, WOMAC score, postoperative complications, revision rate, and ROM score. Patients receiving UKA showed less postoperative pain, less postoperative complications and superior knee function WOMAC score than patients receiving HTO. However, patients undergoing HTO obtained more ROM and less revision rate than patients undergoing UKA. No significant difference was observed between the two groups in terms of excellent/good surgical results and other knee function scores, including Lysholm, HSS score, KSS score, KSFS score, and Tegner score.
To date, several meta-analysis review articles have been published to summarize the benefits and harms of HTO and UKA surgeries on medial KOA patients. Among them, there were variation in the selection of outcome indicators and assessment system, and the results were inconsistent. Comparing with previous studies, half of the selected articles were from China (19 from 38 studies)27–36 and half of them were updated publications in 2019 and 2020 (19 from 38 studies),27–29,32–36 which were not at all or unfrequently discussed in other systemically quantitative analyses, resulting in obviously different comparison results. In contrast with the meta-analyses by Cao et al. 15 Santoso et al. 16 and Han et al. 17 which observed no significant difference on knee function scores, in this study, higher WOMAC score was found after UKA compared with HTO indicating UKA may produce better functional outcome. Similarly with traditional conclusions regarding VAS pain score, postoperative complications and ROM, UKA could cause less pain and complications while HTO could cause increased flexion and extended ROM.
In the current meta-analysis, many included studies adopted OWHTO. According to recent publications, the OWHTO is increasing its popularity. Compared to CWHTO, the OWHTO has several advantages, e.g., easier and more accurate adjustment of alignment correction, the avoidance of serious complications, and higher survival rate at 10-year follow-up.13,37,38 UKA has one disadvantage of higher revision rate, applying the appropriate patient’s indications, modern prosthetic design and techniques would significantly decrease the revision rate.7,39 There were various techniques in UKA in this study, mainly using Oxford III prothesis which was the preferred method currently. 40 As concluded, the pooled data analysis did not find significant difference in terms of revision rate, excellent/good surgical results, and other knee function scoring system including Lysholm, HSS, KSS, KSFS and Tegner score between HTO and UKA. However, when comparing the individual study by Krych et al. in 2017 41 and Bouguennec et al. in 2020, 42 opposite results of revision rate were illustrated in Figure 3(c), and Krych showed higher treatment failure rate for UKA. According to the demographic data analysis, both studies used O/CWHTO procedures, with similar follow-up timing about 6-7 years. Additionally, the mean age of HTO patients was 43 years, and 49 years for UKA patients in the earlier study, while HTO patients aged 55 years and UKA patients aged 64 years in the recent study, which may explain the difference in the revision rate outcome.
Except for the indicators of excellent and good surgical results and postoperative complications, all the other outcomes pooled analyses had high heterogeneity (p < 0.10) which were probably caused by multiple factors such as patient selection, surgeons performing technique, outcome measures and follow-up time. In this meta-analysis, the proportion of female patients was relatively high. For many recent publications, there were no significant difference in age when undergoing HTO and UKA, and most patients were 55–65 years old. The surgical indications of the included studies are not uniform. For the past meta-analysis, many included articles were published earlier, with older technology and higher indications requirements (HTO: mostly younger patients, UKA: mostly older patients), which may suggest clinical heterogeneity. This could also cause differences in outcome analysis results. Moreover, the follow-up time of the literature collected in this study varied. The clinical effects of follow-up were mainly medium and short-term, while the long-term clinical effects lacked research and needed further exploration.
There were several limitations about this study. First, more than half of the studies on HSS score, Lysholm score, VAS score, Tegner score and ROM score collected the data from Chinese Han population, which might lead to biased result in terms of the study population. Second, the sample size was small for certain outcome indicators including KSFS score. Third, follow-up in many update studies was relatively short, therefore the high heterogeneity resulting from varying follow-up times should significantly affect the reliability of the data in terms of revision rate. In fact, additional analysis based on studies with follow-up of more than 60 months significantly changed the pooled result, indicating a beneficial result to HTO. However, due to the limited number of eligible studies, more studies are required to validate this finding. Fourth, this study did not conduct subgroup analysis according to age and HTO types, etc. Furthermore, significant high heterogeneity was observed among the studies.
Conclusion
Our meta-analysis shows that UKA may be associated with reduced postoperative pain, less postoperative complication and good knee function, while the HTO procedure showed superior ROM and less revision rate. Both surgery options yielded satisfactory results, and the treatment options should be carefully considered based on appropriate clinical indications. Further high-quality and large-scale studies are necessary to confirm these findings.
Supplemental Material
Supplemental Material - Unicompartmental knee arthroplasty versus high tibial osteotomy for medial knee osteoarthritis: A systematic review and meta-analysis
Supplemental Material for Unicompartmental knee arthroplasty versus high tibial osteotomy for medial knee osteoarthritis: A systematic review and meta-analysis by Bin Zhang, Hanguang Qian, Hongfu Wu and Xiaofei Yang in Journal of Orthopaedic Surgery
Footnotes
Author contributions
BZ conceived and coordinated the study, designed, performed and analyzed the experiments, wrote the paper. HGQ, HFW and XFY carried out the data collection, data analysis, and revised the paper. All authors reviewed the results and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
All data generated or analysed during this study are included in this published article [and its supplementary information files].
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.