
Abstract
Background
Rotational alignment of the tibial component is critical for successful total knee arthroplasty (TKA). Akagi’s line is a reliable anteroposterior reference, but its intraoperative applicability may be limited when the posterior cruciate ligament (PCL) is not visible after tibial resection. The extensor hallucis longus (EHL) tendon, as an extra-articular and consistently identifiable structure, may represent a practical distal landmark. This study evaluates the anatomical relationship between Akagi’s line and the EHL tendon on computed tomography (CT) and analyzes its association with tibial morphometric parameters.
Methods
A descriptive correlational study was conducted on CT scans of 100 anatomically normal tibiae. Akagi’s line was defined as the line connecting the center of the PCL to the medial border of the patellar tendon. Its distal projection at the tibial plafond was compared with the center of the EHL tendon. Tibial length, morphology, posterior slope, sagittal distance, and the angle of Akagi’s line relative to the femoral transepicondylar axis (TEA) were measured. Two independent observers performed all measurements. Associations were analyzed using Spearman’s correlation coefficients with 95% confidence intervals.
Results
Akagi’s line projected through the center of the EHL tendon in 60% of cases and medially in 40%, with no lateral deviations. The Akagi–EHL distance correlated strongly with tibial length (ρ = 0.71; p < 0.001) and sagittal distance (ρ = 0.70; p < 0.001), but showed no association with tibial slope. No significant correlation was observed between the Akagi-femoral TEA angle and morphometric parameters.
Conclusion
The distal projection of Akagi’s line consistently aligns with, or lies slightly medial to, the center of the EHL tendon. This predictable relationship supports the EHL as a reliable, extra-articular distal landmark for tibial rotational alignment in TKA when intra-articular references are obscured.
Level of evidence
IV (Descriptive study).
Keywords
Introduction
Rotational alignment of the tibial component is a key determinant of the functional success and long-term durability of total knee arthroplasty (TKA). Improper alignment may lead to imbalanced ligament tension, patellar maltracking, increased polyethylene wear, anterior knee pain, and ultimately early implant failure.12–14 To optimize tibial component positioning, surgeons rely on reproducible anteroposterior (AP) tibial references, because the tibial tray is not aligned parallel to the femoral transepicondylar axis (TEA) but oriented according to validated AP axes that demonstrate predictable perpendicularity to the femoral TEA.2–5
To achieve reliable tibial rotational alignment, several anatomical landmarks have been proposed. Among these, Akagi et al. introduced the reference now known as Akagi’s line, defined as the line connecting the center of the posterior cruciate ligament (PCL) to the medial border of the patellar tendon on axial CT images. 1 Subsequent studies have demonstrated its reproducibility, low variability, and nearly perpendicular orientation to the femoral TEA, establishing it as one of the most dependable guides for tibial rotational alignment.6–8
However, despite its strengths, the intraoperative applicability of Akagi’s line may be limited. After tibial resection, the PCL center may become displaced, obscured, or lie outside the operative field, reducing its visibility and usability during TKA.9–11 This challenge has stimulated interest in alternative anatomical references, particularly extra-articular structures, that remain visible throughout the procedure and preserve a stable relationship with Akagi’s line.
Distal anatomical references extending from the ankle to the proximal tibia have gained particular interest in this context. Among them, the extensor hallucis longus (EHL) tendon has been one of the most studied, as it is anatomically constant, easily identifiable, and closely aligned with the mechanical axis of the ankle in cadaveric and tomographic studies.15–17 Hino et al. demonstrated minimal angular deviation between the EHL tendon and Akagi’s line even in the presence of tibial torsion or deformity, 17 while Besa et al. and Bilgen et al. reported improved accuracy in tibial component rotational alignment when the EHL was used as a distal landmark during TKA.15,16
Nevertheless, prior studies have limitations. Several relied on magnetic resonance imaging (MRI), which offers excellent soft-tissue contrast but inferior cortical bone resolution compared with CT. Sample sizes were modest, and key morphometric variables such as tibial length, morphology, posterior tibial slope, and sagittal distances were not comprehensively analyzed. A larger CT-based study may therefore provide more robust and clinically relevant anatomical insights.
The primary objective of this descriptive study is to analyze, through CT measurements of 100 normal tibiae, the anatomical relationship between the classical definition of Akagi’s line and the center of the EHL tendon at the level of the tibial plafond. A secondary objective is to evaluate the association between this relationship and tibial morphometric parameters, including tibial morphology, tibial length, posterior tibial slope, sagittal distance, angle between Akagi’s line and the femoral transepicondylar axis (TEA), and the length of Akagi’s line.
We hypothesize that the distal projection of Akagi’s line consistently aligns with, or lies slightly medial to, the center of the EHL tendon, supporting its potential use as a reliable extra-articular distal anatomical landmark for guiding tibial rotational alignment in total knee arthroplasty.
Materials and methods
A descriptive, correlational study was designed to analyze the anatomical relationship between Akagi’s line and the center of the extensor hallucis longus (EHL) tendon, as well as its association with tibial morphometric variables, through the evaluation of computed tomography (CT) scans of tibias with anatomically normal morphology.
The study was conducted at a tertiary care, high-complexity academic hospital equipped with a centralized Picture Archiving and Communication System (PACS) and a unified electronic medical record system per patient. A retrospective database of CT images was accessed, and 100 studies that met predetermined inclusion criteria were selected.
Inclusion criteria comprised adult patients with complete skeletal maturity and CT scans demonstrating tibias without structural anatomical alterations. Exclusion criteria included images from patients with a history of lower limb orthopedic surgery, bone fractures, tumors, congenital or acquired deformities, or any condition that could alter native tibial anatomy. Incomplete CT studies or those lacking appropriate multiplanar reconstructions (MPR) for the planned measurements were also excluded. Demographic variables (age and sex) and specific anatomical parameters were collected.
All CT scans were obtained using a standardized lower-limb protocol with patients in the supine position and both lower limbs positioned in neutral rotation. Neutral alignment was verified by ensuring that the patella was oriented anteriorly and that the second metatarsal was aligned vertically relative to the tibial crest, minimizing rotational bias during image acquisition. Slice thickness and reconstruction interval were set at 1.0 mm using a bone reconstruction kernel, with multiplanar reconstructions oriented along the mechanical axis of the tibia.
Tibial morphology was qualitatively classified into four types—straight, varus, valgus, and italic “S” —based on coronal MPR images. Straight morphology was defined as a mechanical axis within ±3° of neutral; varus or valgus morphologies as deviations >3° in the medial or lateral direction, respectively; and the S-shaped configuration as the presence of opposite curvatures proximally and distally. Due to small sample sizes in the valgus (n = 2) and S-shaped (n = 3) groups, these categories were analyzed descriptively only.
Measurements
Using MPR reconstructions, the following measurements were performed: • Tibial length in the coronal plane was measured from the medial proximal tibial plateau to the distal tip of the medial malleolus (Figure 1(a)). • Sagittal distance, defined as the linear distance between the proximal origin of Akagi’s line and its distal projection at the tibial plafond (Figure 1(b)). • Angle between Akagi’s line and the femoral transepicondylar axis (TEA), after establishing the TEA by identifying the medial and lateral femoral epicondylar prominences on axial slices. • Tibial slope angle, defined as the inclination of the medial tibial plateau relative to the longitudinal tibial axis in the sagittal plane (Figure 1(c)). • Total length of Akagi’s line, measured between the center of the posterior cruciate ligament (PCL) footprint and the medial border of the patellar tendon insertion (Figure 2).
Distal projection of Akagi’s line in relation to the EHL tendon at the level of the tibial plafond
At the level of the tibial plafond, the distal projection of Akagi’s line was evaluated in relation to the center of the extensor hallucis longus (EHL) tendon. The tendon was identified on axial CT images as a distinct anterior soft-tissue structure within the anterior compartment, typically located between the tibialis anterior and extensor digitorum longus tendons. Its center was defined geometrically as the midpoint of the tendon cross-sectional area.
Although CT provides lower soft-tissue contrast than MRI, the EHL tendon could be consistently identified at this level due to its characteristic anatomical position and morphology. High-resolution axial reconstructions (1.0 mm slice thickness) were used to optimize visualization.
The distal projection of Akagi’s line was then classified as centered (0 mm), medially displaced (negative values), or laterally displaced (positive values) relative to the geometric center of the EHL tendon. Medial and lateral deviations were defined radiologically and geometrically rather than based on soft-tissue margins. No lateral deviations were observed in this study (Figure 3). Multiplanar CT reconstructions illustrating study measurements: (a) Tibial length from the medial proximal tibial plateau to the distal tip of the medial malleolus. (b) Sagittal distance between the proximal origin of Akagi's line and its distal projection at the tibial plafond. (c) Tibial slope in the sagittal plane. Akagi’s line (solid red line) drawn from the center of the posterior cruciate ligament (PCL) footprint to the medial border of the patellar tendon (PT) on axial CT images. This definition reflects the classical description of Akagi’s line used for tibial rotational alignment. Axial CT image at the level of the tibial plafond demonstrating identification of the extensor hallucis longus (EHL) tendon and the distal projection of Akagi’s line relative to its geometric center. Medial deviations are represented as negative values and lateral deviations as positive values (none observed in this study).


Observer reliability and data management
All measurements were independently performed by two orthopedic surgeons specialized in musculoskeletal imaging using standardized measurement tools within the institutional PACS system. Linear and angular parameters were recorded separately by each observer. When discrepancies greater than 2 mm for linear measurements or 2° for angular measurements were identified, both observers jointly reviewed the images and reached a consensus value through direct reassessment.
Formal inter- and intraobserver reliability coefficients were not calculated and are acknowledged as a methodological limitation of this study.
Data collection and management were performed using the REDCap (Research Electronic Data Capture) platform.
The study protocol was approved by the Institutional Review Board [blinded for peer review] (Approval No. P25-059, 09/18/2025). Due to its retrospective nature and minimal risk, a waiver of informed consent was granted in accordance with national regulations (Laws No. 25.326 and 26.529, Provincial Law No. 15.462).
Statistical analysis
Data were processed and analyzed using descriptive and inferential statistical techniques with Python (version 3.11), along with the pandas (2.0.3), numpy (1.25), and scipy.stats (1.11.0) libraries.
Continuous quantitative variables were described using mean, standard deviation, and range; categorical variables were expressed as frequencies and percentages. To explore associations between the distal orientation of Akagi’s line and tibial morphometric variables, Spearman’s rank correlation coefficient was used, given the non-parametric nature of the data. Correlation strength was categorized as weak (ρ < 0.30), moderate (ρ = 0.30–0.69), or strong (ρ ≥ 0.70), with statistical significance set at p < 0.05. For significant correlations, 95% confidence intervals were calculated. Finally, exploratory contingency tables were constructed to describe the distribution of the distal projection of Akagi’s line according to tibial morphology. Data quality was ensured through double review and cross-validation between observers.
Results
A total of 100 computed tomography (CT) scans of anatomically normal tibiae were analyzed. The mean age of the patients was 38.6 years (SD ± 15.6), with a sex distribution of 58% female and 42% male. The predominant tibial morphology was straight (77%), followed by varus (18%), italic “S” shape (3%), and valgus (2%).
Correspondence between Akagi’s Line and the Extensor Hallucis Longus (EHL)
Distal position of Akagi’s Line relative to the center of the EHL tendon.
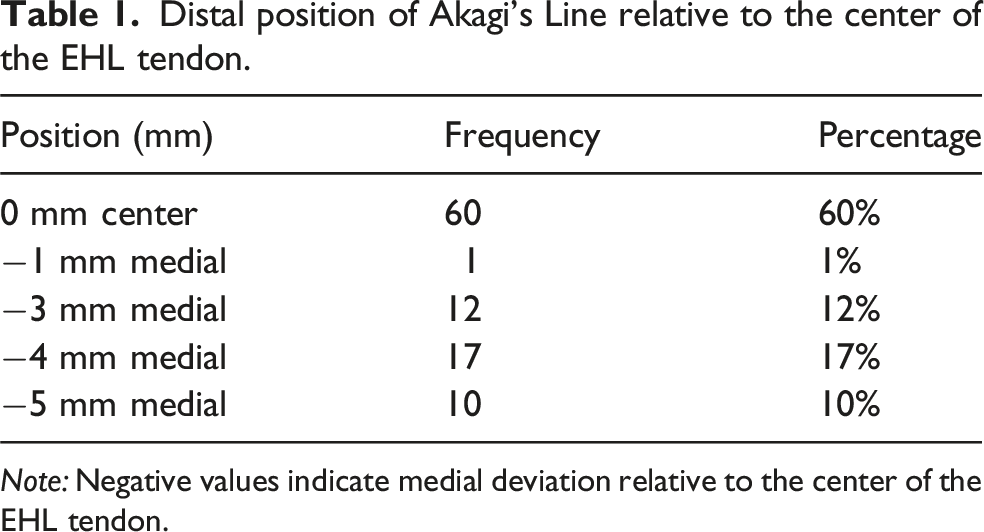
Note: Negative values indicate medial deviation relative to the center of the EHL tendon.
Relationship with tibial morphology
Distal position of Akagi’s line according to tibial morphology (descriptive analysis).

Note: All deviations were medial; no lateral deviations were observed.

Distribution of the distal projection of Akagi’s line relative to the center of the EHL tendon across different tibial morphologies (straight, varus, valgus, italic “S”). Straight tibias showed the highest frequency of alignment with the EHL center.
Correlation between morphometric variables
Spearman’s correlation analysis revealed a strong and statistically significant association between the Akagi–EHL distance and tibial length (ρ = 0.71; 95% CI: 0.60–0.80; p < 0.001), as well as with the sagittal distance between Akagi’s line and the tibial plafond (ρ = 0.70; 95% CI: 0.58–0.79; p < 0.001).
A weak but statistically significant correlation was also identified with the distance to the lateral edge of the EHL (ρ = 0.21; 95% CI: 0.01–0.39; p = 0.033).
Spearman correlation coefficients (ρ) with 95% confidence intervals for tibial morphometric variables.

Note: EHL: Extensor Hallucis Longus; CI: Confidence Interval.
Angular analysis of Akagi’s line
The angle formed by Akagi’s line relative to the femoral transepicondylar axis (TEA) had a mean of 84.0° (SD ± 3.0°), with a range from 76° to 89°, indicating relatively low interindividual variability.
No significant correlation was observed between the Akagi–femoral TEA angle and tibial length (ρ = 0.09; p = 0.35) (Figure 5). Similarly, no significant association was found between the Akagi–femoral TEA angle and sagittal distance to the tibial plafond (ρ = 0.08; p = 0.41) (Figure 6). Scatter plot illustrating the relationship between tibial length and the Akagi–femoral TEA angle. No significant correlation was observed between these variables. Scatter plot demonstrating the relationship between sagittal distance and the Akagi–femoral TEA angle. No significant association was identified.

Due to the limited variability in tibial slope, no valid correlation could be established for this parameter.
Discussion
The present study analyzed the anatomical correlation between Akagi’s line and the extensor hallucis longus (EHL) tendon in 100 anatomically normal tibiae to determine whether this distal, extra-articular, and consistently identifiable landmark may serve as a reliable reference for tibial rotational alignment in total knee arthroplasty (TKA). Our results showed that in 60% of cases, the distal projection of Akagi’s line coincided with the center of the EHL tendon, while in the remaining 40% it was located medially, with no lateral deviations observed. These findings reinforce the notion that the EHL maintains a predictable relationship with Akagi’s line and may therefore serve as a practical alignment guide when intra-articular structures are obscured after tibial resection.9–11
A strong and statistically significant correlation was observed between the Akagi–EHL distance and morphometric parameters such as tibial length and sagittal distance to the tibial plafond. This suggests that larger tibiae tend to exhibit greater longitudinal separation between anatomical landmarks, which in turn affects the distal projection of Akagi’s line. The inclusion of 95% confidence intervals provided greater precision in assessing the strength of these associations. In contrast, no significant relationship was found between the Akagi–EHL distance and tibial slope, likely reflecting the limited variability of slope within our sample. These observations underline that certain, but not all, anatomical features may influence proximal-to-distal anatomical projections and should be considered when planning individualized tibial rotational positioning.
Angular analysis revealed that Akagi’s line formed a mean angle of 84.0° relative to the femoral transepicondylar axis (TEA), with low interindividual variability, confirming the reproducibility of Akagi’s line as an anteroposterior (AP) reference 1. The observed angular relationship between Akagi’s line and the femoral transepicondylar axis is consistent with previous studies demonstrating that Akagi’s line represents a reliable anteroposterior tibial axis that is nearly perpendicular to the femoral TEA. 1 The absence of significant correlations between the Akagi–femoral TEA angle and morphometric parameters, including tibial length and sagittal distance, suggests that the proximal angular orientation of Akagi’s line is largely independent of tibial size and longitudinal morphology.
From a practical standpoint, the use of the EHL tendon as a distal anatomical reference offers several advantages. Its extra-articular location, anatomical consistency, and continuous visibility even after tibial resection make it appealing when classical intra-articular references such as the PCL insertion are altered or obscured during TKA.9–11 Although intraoperative identification of the EHL tendon was not directly evaluated in this CT-based study, its superficial anatomical location and consistent position within the anterior compartment make it readily identifiable through palpation or direct visualization during surgery, as reported in previous clinical series.15,16 In this context, our findings align with the anatomical framework originally described by Akagi et al., who demonstrated that their AP axis is consistently perpendicular to the femoral TEA. 1 By showing that this proximal axis maintains a predictable distal relationship with the EHL tendon, our study suggests that the EHL may serve as a practical extension of Akagi’s concept.
These results are also supported by recent literature. Hino et al. demonstrated using MRI that the EHL maintains a stable orientation relative to Akagi’s line even in the presence of tibial torsion or deformity. 17 Although tibial torsion was not measured as an independent variable in the present study, its potential influence is indirectly reflected in the proximal-to-distal projection of Akagi’s line toward the EHL tendon. Besa et al. reported that using the EHL as a distal reference resulted in adequate rotational alignment in 81% of TKA procedures, 16 while Bilgen et al. showed that the EHL provides greater accuracy than the second metatarsal as a distal landmark. 15 Our findings derived from CT imaging provide higher-resolution bony anatomy while still allowing consistent identification of the extensor hallucis longus (EHL) tendon at the level of the tibial plafond, despite the inherent limitations of soft-tissue contrast compared with MRI. 18
Regarding tibial morphology, tibiae with a straight configuration showed a greater likelihood of alignment between Akagi’s line and the center of the EHL tendon, whereas varus and valgus morphologies tended to exhibit more medial projections. Although formal statistical comparisons were not performed due to the very small size of some subgroups, the observed trend highlights the potential influence of coronal plane deformity on distal anatomical projections, an increasingly relevant factor in the era of personalized alignment strategies.
This study has several limitations. First, it is a retrospective, CT-based analysis conducted exclusively on anatomically normal tibiae, which may limit the generalizability of the findings to populations with osteoarthritis, coronal deformity, or altered mechanical axes. Second, although all measurements were performed independently by two observers and consensus was reached in cases of discrepancy, formal inter- and intraobserver reliability coefficients were not calculated. Third, tibial torsion, which plays an important role in tibial rotational alignment, was not measured as an independent parameter. Although its effect may be partially incorporated through the analysis of the proximal-to-distal projection of Akagi’s line, direct torsional assessment was beyond the scope of this study and should be addressed in future investigations. Finally, while this study provides anatomical and morphometric support for the extensor hallucis longus tendon as a potential distal reference, its intraoperative applicability and clinical impact during total knee arthroplasty were not directly assessed and require further validation through prospective, cadaveric, or navigation-based studies.
Future research should therefore include patients with varying joint pathologies, incorporate formal interobserver reliability assessment, and evaluate the intraoperative performance of the EHL as a rotational guide through navigation or postoperative CT-based accuracy validation.
Conclusion
The extensor hallucis longus (EHL) tendon demonstrates a consistent anatomical relationship with the distal projection of Akagi’s line, particularly in tibiae with straight morphology. In most cases, this projection coincides with the center of the EHL or lies slightly medial to it, and no lateral deviations were observed. This predictable positioning combined with the tendon’s extra-articular location, anatomical stability, and ease of identification even after tibial resection supports the EHL as a useful complementary distal landmark for guiding tibial component rotational alignment in total knee arthroplasty.
These findings, obtained from CT-based measurements of anatomically normal tibiae, provide anatomical and morphometric support for the potential intraoperative use of the EHL; however, clinical validation in pathological knees and intraoperative environments is required before definitive implementation.
Footnotes
Ethical considerations
This study was approved by the Institutional Review Board [blinded for peer review] (Approval No. P25-059). The study protocol was approved by the Institutional Review Board of the Faculty of Biomedical Sciences at Universidad Austral (Approval No. P25-059, 09/18/2025). The study was conducted in accordance with the Declaration of Helsinki and applicable national regulations (Laws No. 25.326 and 26.529, Provincial Law No. 15.462).
Consent to participate
A waiver of individual informed consent was granted due to the retrospective design and the use of anonymized CT data. Informed consent was waived due to the retrospective design and minimal risk to participants.
Authors’ contributions
Gabriel O. Pérez Lloveras: Study conceptualization, methodology design, supervision, and critical revision of the manuscript. Mauricio Chiotta Romano: CT measurements, data curation, and drafting of the manuscript. Carlos Autorino: Statistical analysis, interpretation of results, and manuscript review. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.