
Abstract
Total knee arthroplasty (TKA) is a frequently performed surgery for restoring function in patients with severe knee osteoarthritis. TKA is associated with significant healthcare costs, partly due to complications leading to readmissions. This study aimed to identify biomarkers predictive of readmission after TKA. Data of adult patients who underwent primary TKA between 2014 and 2022 extracted from the Chang Gung Medical Research Database were retrospectively reviewed. Associations between the monocyte-to-albumin ratio (MAR), red cell distribution with (RDW)-to-albumin ratio (RAR), hemoglobin-to-albumin ratio (HAR), leukocyte-to-albumin ratio (LAR), and platelet-to-albumin ratio (PAR) with 14-day readmission were determined using univariate and multivariable regression analyses. A score termed the ‘MAR-LAR-PAR’ score was developed using the combination of these 3 markers, and its prognostic value was assessed. Data from 1,137 patients were included. Elevated MAR (adjusted odds ratio [aOR] = 1.77, 95% confidence interval [CI]: 1.08–2.89, p = 0.022), LAR (aOR = 1.59, 95% CI: 1.02–2.45, p = 0.039), and PAR (aOR = 1.88, 95% CI: 1.12–3.15, p = 0.016) were significantly associated with increased risk of 14-day readmission. The highest MAR-LAR-PAR score (score = 3) was significantly associated with 14-day readmission compared to score = 0 (aOR = 4.24, 95% CI: 1.91–9.44, p < 0.001). This study highlights the potential of MAR, LAR, PAR, and the score based on their combination, as significant predictors of short-term readmission following TKA. Incorporating these biomarkers into preoperative assessment may help determine the risk of readmission, and provide additional care for these patients.
Keywords
Introduction
Total knee arthroplasty (TKA) is the definitive treatment for patients with severe knee osteoarthritis. 1 In the United States (US), there has been a 134% increase in the number of TKAs performed from 2005 to 2018, making it one of the most frequently performed surgeries. 2 While the success rate of TKA is high, the procedure is associated with significant healthcare costs, contributing approximately $2.7 billion annually to US healthcare expenditures, partly due to postoperative complications that can lead to hospital readmission.2,3 Consequently, reducing the frequency of readmissions after TKA is a global priority for healthcare systems, as it indicates improved patient outcomes and optimized resource utilization.
Recent studies have highlighted the potential of various biomarkers in predicting postoperative outcomes in various orthopedic surgeries.4–7 Among these, the ratios of certain blood components, such as the monocyte-to-albumin ratio (MAR), red cell distribution width (RDW)-to-albumin ratio (RAR), hemoglobin-to-albumin ratio (HAR), leukocyte-to-albumin ratio (LAR), and platelet-to-albumin ratio (PAR), have emerged as promising predictors of inflammatory status and nutritional health, both of which are critical in the recovery process after surgery.8,9 Albumin is an important plasma protein and is well known to reflect nutritional status and systemic inflammation. 10 It plays a crucial role in maintaining colloid osmotic pressure and serves as a carrier for drugs, hormones, and other substances. A low albumin level is associated with poor outcomes in various medical conditions, reflecting its role in disease severity and health status. 11 Monocytes, red blood cells (RBCs), hemoglobin, leukocytes, and platelets also play significant roles in the body’s response to surgical stress and injury. 12 For instance, monocytes are key players in the immune response and wound healing, and variations in their concentration can indicate an altered immune status. 13 The RDW is a measure of the variability in RBC size and has been associated with adverse outcomes in cardiovascular and inflammatory diseases. 14 Use of the aforementioned ratios may provide information for risk stratification by incorporating information about immune status, inflammation, and nutritional health.
Importantly, the role of the aforementioned ratios with respect to TKA, and particularly their predictive value for readmission after surgery, has not been thoroughly investigated. Thus, the purpose of this study is to determine if MAR, RAR, HAR, LAR, and PAR can serve as reliable predictors of readmission after TKA. We hypothesize that higher levels of these biomarkers are associated with an increased risk of readmission within 14 days post-TKA. The findings may potentially contribute to the proper integration of these parameters into preoperative risk assessment models, thereby enhancing the precision of patient care strategies in TKA.
Methods
Data source
This population-based retrospective study used data from the Chang Gung Medical Research Database (CGRD) collected from 2014 to 2022. The CGRD was established by Taiwan’s Chang Gung Medical Foundation and is a critical resource for clinical and epidemiological research. The database is compiled from our extensive Hospital network, the largest in Taiwan, and includes patient demographic information, medical history, treatments, and outcomes.15,16
Study design and patients
Data of adults ≥20 years of age who underwent primary TKA performed by a single orthopedic surgeon (W-C Chen) during the period between 2014 and 2022 were retrospectively reviewed. Exclusion criteria included patients with a follow-up of <14 days or missing data for the hematologic biomarkers of interest.
Ethics statement
This study was approved by the institutional review board of our Hospital. We analyzed a pre-collected dataset that had been de-identified to ensure anonymity and protect the privacy of the participants. All patient data were handled in strict compliance with ethical guidelines to maintain confidentiality and ensure that no individual could be identified from the data used in this study.
Biomarker assessment
This study assessed the MAR, RAR, HAR, LAR, and PAR as potential indicators of readmissions following TKA. These markers were chosen based on our review of the medical literature, which highlights their potential prognostic value in surgical settings. To broaden the study population, these markers were derived from blood samples collected from 1 month before to 1 week after surgery, and used values nearest to the day of surgery.
Main outcome
The primary outcome was hospital readmission for any cause within 14 days after TKA, aiming to focus on early post-surgical readmissions.
Other study variables
Covariates included age, sex, body mass index (BMI), comorbid conditions (e.g., diabetes, hypertension, ischemic heart disease, osteoporosis, chronic kidney disease [CKD], chronic pulmonary disease, and rheumatic disease), and the Charlson Comorbidity Index (CCI). Intraoperative factors examined included blood loss and the duration of the surgery. The type of anticoagulant prophylaxis used was also included in the analyses.
Clinical scoring system
We developed a clinical scoring system based on MAR, LAR, and PAR, termed the ‘MAR-LAR-PAR score’. The scoring criteria were as follows: Score 0: all biomarkers are below the optimal threshold; Score 1: one biomarker exceeds the optimal threshold; Score 2: Two biomarkers exceed the optimal threshold; Score 3: Three biomarkers exceed the optimal threshold.
Statistical analysis
Continuous data were presented as the mean ± standard deviation (SD), and the median (minimum-maximum), and categorical data were presented as numbers (%). The receiver operating characteristic (ROC) curve analysis was used to determine the optimal thresholds for the biomarkers studied. The p-value for between-group comparisons was calculated using the logistic regression analysis. Univariate and multiple regression analyses were used to determine the odds ratio (OR) and 95% confidence interval (CI) of 14-day readmission. The multivariable model was adjusted for related variables with a p-value <0.15 in the univariate analysis (except for laboratory data), including age, sex, anticoagulant prophylaxis, intraoperative blood loss, and operative duration. All p-values were 2-sided, and a value of p < 0.05 was considered statistically significant. All statistical analyses were performed using the statistical software package SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Study population selection
The study population selection process is depicted in Figure 1. Data from 1270 patients ≥20 years old who underwent primary TKA from 2014 to 2022 were extracted from the database. Patients with missing information of MAR (n = 66) and RAR (n = 1) were excluded, and 66 patients with a follow-up of <14 days were further excluded. Finally, 1137 patients were included in the analyses (Figure 1). Flow diagram of patient selection.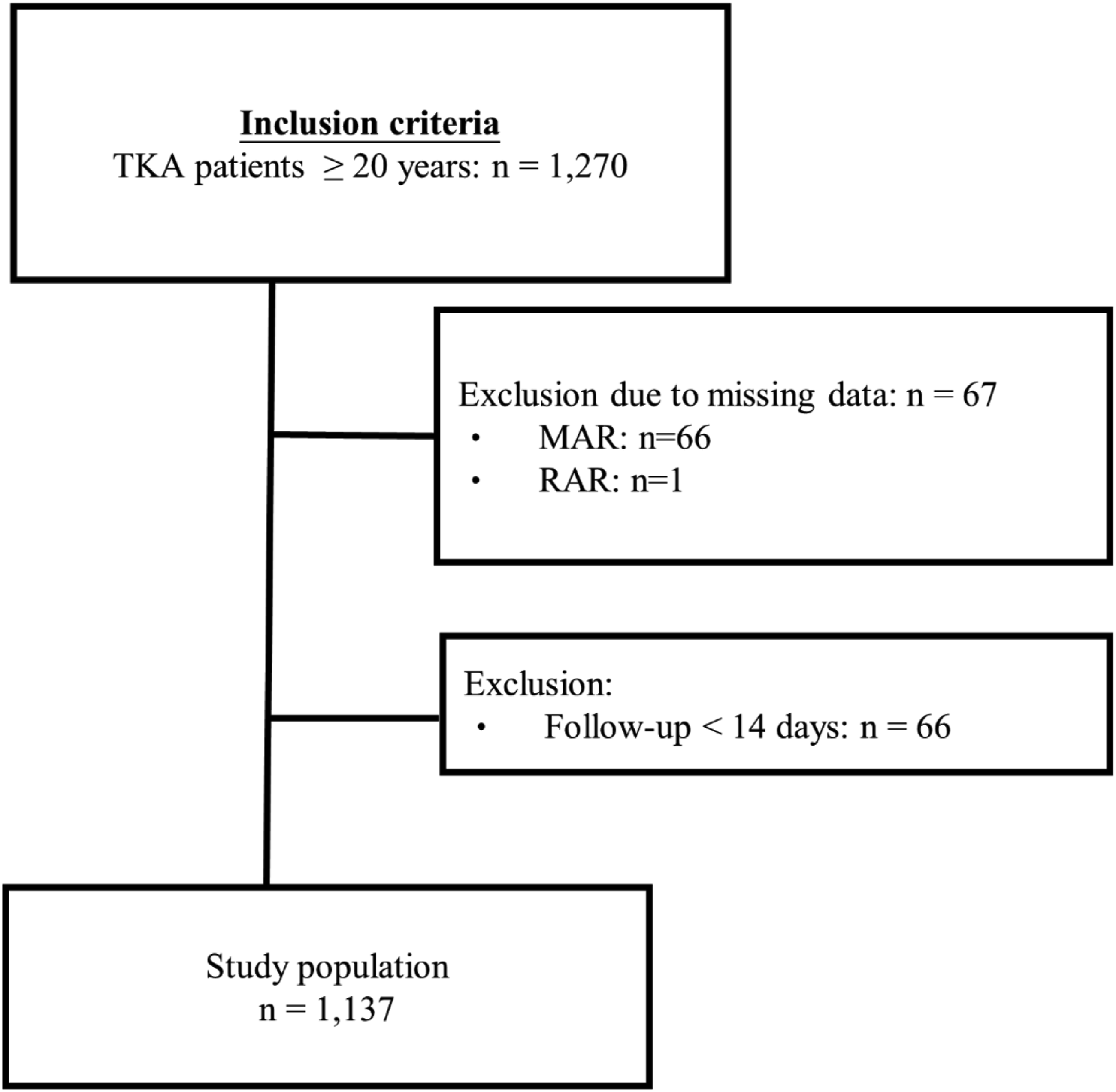
Patient characteristics
Patient characteristics.

ALT, alanine aminotransferase; AST, aspartate aminotransferase; aOR, adjusted odds ratio; BUN, blood urea nitrogen; CCI, Charlson comorbidity index; CI, confidence; CKD, chronic kidney disease; CRP, C-reactive protein; DOACs, direct oral anticoagulants; GOT, glutamic oxaloacetic transaminase; GPT, glutamic-pyruvic transaminase; HAR, hemoglobin-to-albumin ratio; LAR, leukocyte-to-albumin ratio; MAR, monocyte-to-albumin ratio; PAR, platelet-to-albumin ratio; RAR, RDW-to-albumin ratio; RBC, red blood cell; RDW, red cell distribution width; WCB, white blood cell.
Continuous variables are presented as mean ± standard deviation; medium (minimum-maximum).
Categorical variables are presented as count (percentage).
p-value <0.05 are shown in bold.
The optimal thresholds of MAR, RAR, HAR, LAR, and PAR for predicting 14-day readmissions following TKA, established using the ROC curve analysis, are shown in Supplemental Table 1 (Supplemental Table 1).
In the univariate analyses, patients with a MAR greater than the optimal threshold had a significantly higher risk of 14-day readmission (73% vs 60%, crude OR = 1.76, 95% CI: 1.10–2.80, p = 0.018) compared to those with a MAR less than the optimal threshold. Similarly, patients with a PAR greater than the optimal threshold had a significantly higher risk of 14-day readmission (25% vs 16%, crude OR = 1.73, 95% CI: 1.06–2.83, p = 0.028) compared to those with a value less than the optimal threshold (Table 1).
Associations between MAR, RAR, HAR, LAR, PAR, and 14-day readmission by multivariable analyses
Associations between MAR, RAR, HAR, LAR, PAR, and 14-day readmission (n = 1135).
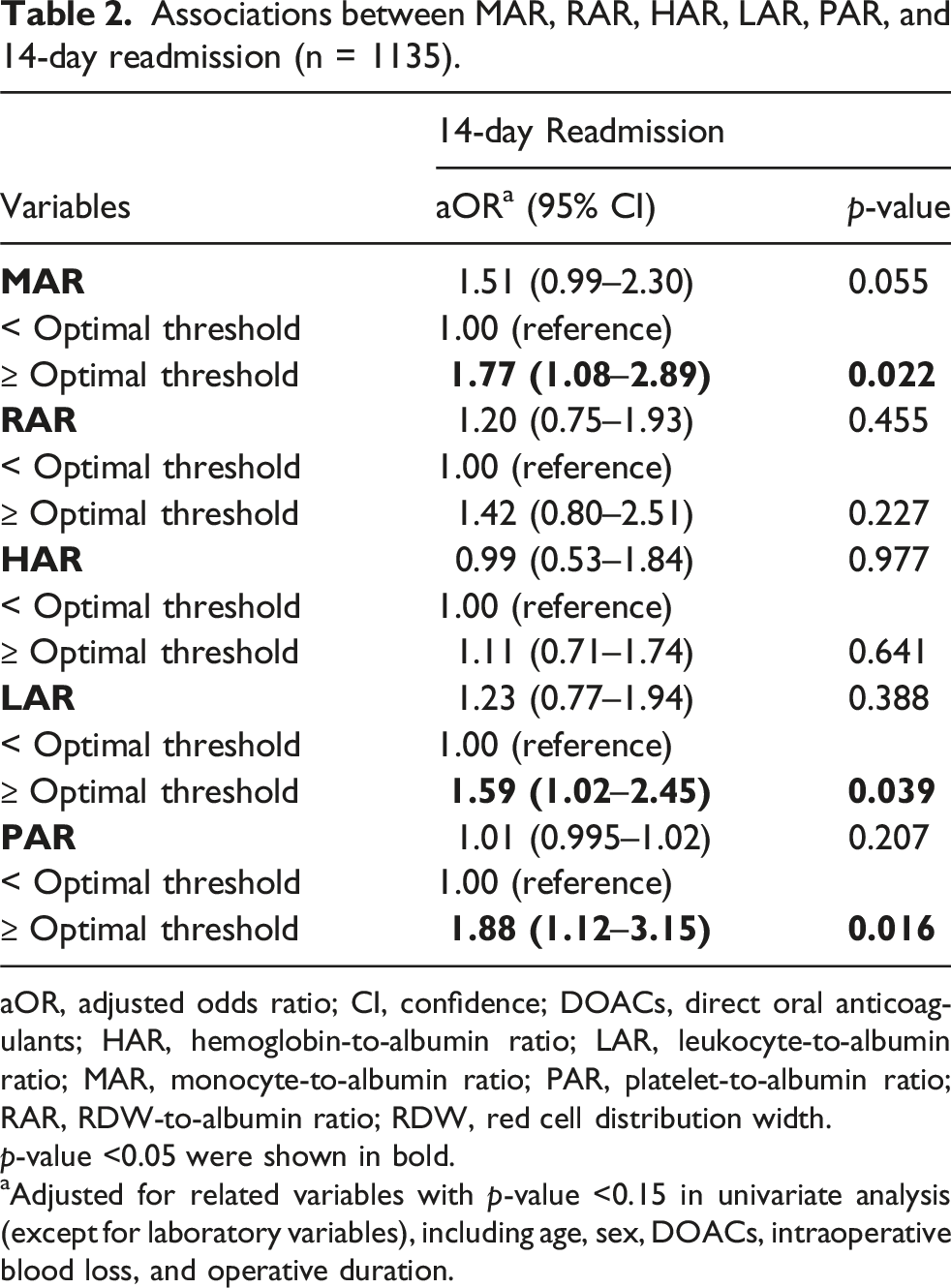
aOR, adjusted odds ratio; CI, confidence; DOACs, direct oral anticoagulants; HAR, hemoglobin-to-albumin ratio; LAR, leukocyte-to-albumin ratio; MAR, monocyte-to-albumin ratio; PAR, platelet-to-albumin ratio; RAR, RDW-to-albumin ratio; RDW, red cell distribution width.
p-value <0.05 were shown in bold.
aAdjusted for related variables with p-value <0.15 in univariate analysis (except for laboratory variables), including age, sex, DOACs, intraoperative blood loss, and operative duration.
Associations between MAR-LAR-PAR score and 14-day readmission
Associations between MAR-LAR-PAR score and 14-day readmission (n = 1135).

aOR, adjusted odds ratio; CI, confidence; DOACs, direct oral anticoagulants; LAR, leukocyte-to-albumin ratio; MAR, monocyte-to-albumin ratio; PAR, platelet-to-albumin ratio.
p-value <0.05 are shown in bold.
aAdjusted for related variables with a p-value <0.15 in univariate analysis (except for laboratory variables), including age, sex, DOACs, intraoperative blood loss, and operative duration.
Discussion
The study evaluated the predictive value of 5 albumin-related markers, MAR, RAR, HAR, LAR, and PAR, for predicting the risk of 14-day readmission following primary TKA. The results demonstrated that values of MAR, LAR, or PAR were associated with a significantly increased risk of readmission within 14 days after TKA. Furthermore, we developed a composite score based on MAR, LAR, and PAR (MAR-LAR-PAR score), and patients with a high MAR-LAR-PAR score had a 4.2-fold increased risk of readmission. This suggests that incorporating these biomarkers and the scoring system into preoperative assessments could improve patient care by identifying individuals at high risk for early readmission, thus enhancing patient outcomes and reducing the overall healthcare burden of TKA.
Risk stratification and determining prognosis is crucial in all fields of medicine as identifying patients at increased risk of complications and mortality can provide more comprehensive care and improve outcomes, as well as provide improved allocation of health care resources. Many studies have sought to determine the value of various indices calculated from routine blood tests for determining risk in various fields of medicine. Our study aligns with this practice, illustrating the clinical utility of MAR, LAR, and PAR in the prognostication of TKA, filling the current knowledge gap. The biological plausibility of these findings further supports their relevance. Elevated albumin-adjusted inflammatory markers such as MAR, LAR, and PAR reflect heightened systemic inflammation, reduced nutritional reserve, and impaired immune function—physiologic states known to increase susceptibility to postoperative complications, including infection, wound problems, uncontrolled pain, and early medical deterioration.7,17 Therefore, although we were unable to correlate these markers with specific readmission etiologies, their utility as global indicators of physiological stress and early postoperative vulnerability remains clinically meaningful.
We found that MAR and LAR could serve as predictors for readmission following TKA. Although not focused on arthroplasty, previous research has indicated the value of MAR and LAR across different fields of medicine. For instance, Zhang et al. 7 reported that a higher MAR value was significantly associated with all-cause mortality and cardiac mortality in patients undergoing percutaneous coronary intervention PCI. Similarly, Lessomo et al. 18 reported that LAR value was significantly associated with the severity of atrial fibrillation, and Peng et al. 19 found that the neutrophil-to-albumin ratio was significantly associated with mortality in patients with cardiogenic shock. A recent study found that MAR was significantly correlated with the presence of non-small cell lung cancer. 20 However, no study has yet examined these two markers in orthopedic surgeries, underscoring the novelty of our approach.
PAR is also a crucial marker with significant clinical relevance identified in our current analysis. It has been demonstrated by studies on conditions ranging from acute coronary syndrome to oncological and renal pathologies, suggesting its broad utility. Hao et al. 21 studied PAR in patients with non-ST-segment elevation acute coronary syndrome undergoing PCI. A higher PAR was significantly associated with higher rates of major cardiovascular adverse events, and the AUC of PAR for 3-year MACE was 0.659. Zhai et al. 22 examined the results of ICU patients to determine if there was an association between PAR and persistent AKI (pAKI). The C-index of PAR for predicting pAKI was 0.744, and PAR exhibited better predictive ability than other indicators of systemic inflammation. Another recent study found that PAR exhibited high sensitivity and specificity for predicting diabetic nephropathy in patients with type 2 diabetes mellitus. 23 In a study of patients with esophageal squamous cell carcinoma receiving definitive radiotherapy. Patients with a high PAR had poorer overall survival (OS) and PFS compared to those with a low PAR. 24
Additionally, although our analysis did not find a predictive value of HAR, Hu et al. 25 indicate its significance in other clinical settings, such as gastric cancer, where a low HAR was linked to poor prognosis. Xu et al. 26 developed a composite indicator called the HALP score, incorporating hemoglobin, albumin, lymphocyte, and platelet levels, which is similar to our approach. A low HALP score was significantly associated with decreased overall survival, cancer-specific survival, and progression-free survival, with consistent results across various malignancy types and stages.
It is important to note that no prior studies have demonstrated the predictive value of MAR, LAR, and PAR in the context of TKA, as evaluated in the current study, precluding direct comparisons. Nevertheless, several reports have documented indicators that may be closely related to our indicators of interest. For example, the CRP-to-albumin ratio, as an indicator of both inflammation and nutrition, was reported to have a greater prognostic capacity than other factors in determining the risk of periprosthetic infection (PJI) for total joint arthroplasty (TJA). 27 Specifically, albumin is the most abundant protein in the body and serves as a crucial indicator of nutritional status and overall health. Multiple studies have shown that a decrease in perioperative albumin levels is associated with unfavorable outcomes following total joint arthroplasty, including delirium. 28 Another study documented that lower preoperative albumin levels are an independent risk factor for acute infection, with a negative dose-response relationship observed among patients undergoing TJA. 29 Additionally, albumin and the fibrinogen-to-albumin ratio, which incorporates both inflammation and nutritional status, can be used to monitor the acute phase response following TKA. 30 A database analysis involving approximately 162,000 TKA patients demonstrated that low albumin levels were significantly linked to postoperative complications such as wound infections and other infections. 31 Intriguingly, Nelson et al. 32 reported that low albumin levels correlated more strongly with postoperative complications, including surgical site infections, renal failure, and pneumonia, than did morbid obesity, a known risk factor for adverse outcomes. On the other hand, abnormal platelet counts have been correlated with adverse outcomes, including readmission following TKA. 33 These observations, despite not being through direct comparisons, partly support our findings on the predictive value of MAR, LAR, and PAR for outcomes after TKA.
While exploring the potential mechanisms behind why blood cells and albumin ratios can serve as prognostic markers of TKA, we find that interactions between platelets and other blood components, particularly leukocytes, play a pivotal role. Platelets, for example, are not only involved in hemostasis but also inflammatory processes, as evidenced by their interaction with lymphocytes in atherosclerotic plaques, highlighting the inflammatory and thrombotic nature of atherosclerosis. 34 Sarma et al. 35 observed increased total binding of platelets to monocytes in the blood of patients with unstable angina and patients who had a myocardial infarction. Similarly, platelet-monocyte aggregates are now believed to play an important role in the pathogenesis of sepsis, and their presence may be an important prognostic indicator. 36 A recent review of the literature by Rolling et al. 37 summarized the available literature on the interactions of platelets and monocytes, and studies that have found platelet-monocyte aggregates play important roles in many diseases, including inflammatory and autoimmune disorders such as cardiovascular disease, systemic lupus erythematosus, and COVID-19. That review highlighted that monocytes in contact with platelets become proinflammatory and procoagulant and that this interaction is now believed to be a central element of thromboinflammation. These interactions provide a biological foundation for the prognostic value of platelet-related ratios like PAR in our study. However, further experimental research and prospective studies are essential to fully understand the underlying mechanistic pathways.
In summary, by searching for effective predictive indicators in TKA patients, our study contributes to a growing body of evidence that supports the role of markers reflecting systemic inflammation, nutritional status, and both in determining clinical outcomes.
Strengths and limitations
One of the primary strengths of this study is the use of a large, nationally representative database that offers comprehensive and reliable data from the largest healthcare network in Taiwan. This extensive dataset enables robust statistical analysis, enhancing the generalizability of our findings. Additionally, the development of the MAR-LAR-PAR score represents an innovative approach to predict readmission risk using easily accessible and low-cost biomarkers, making it a potentially valuable tool for widespread clinical application.
However, this study also has several limitations. First, its retrospective design and the exclusion of patients with incomplete data might introduce selection bias. Second, despite including data from more than 1 center, the study was conducted within a single healthcare system, and thus may not fully represent other populations or settings, potentially limiting the external validity of the results. Importantly, the specific causes of 14-day readmission were not available, and therefore, cause-specific analyses could not be performed. Our findings reflect overall readmission risk rather than associations with particular postoperative complications. Additionally, we focused solely on the rate of readmission rather than reoperation. Moreover, the time window for sampling is within a relatively broad range of time, varied across individual patients, which could influence the outcomes and inferences. Lastly, we did not account for all possible confounding variables that could influence readmission, such as patient mobility or social support systems, which could affect the robustness of our conclusions. In the future, a larger sample would enhance the statistical power and reliability of our findings. Importantly, the clinical applicability of these ratios requires further validation across different cohorts before they can be routinely used in regular practice and laboratory reporting.
Conclusion
In conclusion, this study established that MAR, LAR, and PAR are significant predictors of 14-day readmission following primary TKA, using a large clinical database in Taiwan. The development of the MAR-LAR-PAR score, integrating these biomarkers, was found to have promising predictive value for readmission within 14 days after TKA. Given that such biomarkers are convenient and readily accessible in almost all medical institutions, incorporating the MAR-LAR-PAR score and these markers into clinical practice has good potential to enhance patient management and reduce the incidence of costly readmissions.
Supplemental material
Supplemental material - Predictive value of monocyte-to-albumin ratio, red cell distribution with-to-albumin ratio, hemoglobin-to-albumin ratio, leukocyte-to-albumin ratio, and platelet-to-albumin ratio for 14-day readmission following primary total knee arthroplasty
Supplemental material for Predictive value of monocyte-to-albumin ratio, red cell distribution with-to-albumin ratio, hemoglobin-to-albumin ratio, leukocyte-to-albumin ratio, and platelet-to-albumin ratio for 14-day readmission following primary total knee arthroplasty by Ngi-Chiong Lau, Ching-Wei Hu, Chih-Chien Hu, Yu‐Yi Huang, Pin-Ren Huang and Dave W. Chen in Journal of Orthopaedic Surgery
Footnotes
Acknowledgements
This study is based in part on data from the Chang Gung Research Database provided by Chang Gung Memorial Hospital. The interpretation and conclusions contained herein do not represent the position of Chang Gung Memorial Hospital. The authors thank the statistical assistance and wish to acknowledge the support of the Maintenance Project of the Center of data science and Biostatistics (Grant CLRPG2C0021, CLRPG2C0022, CLRPG2C0023, CLRPG2C0024, CLRPG2G0081, CLRPG2G0082, CLRPG2G0083, CLRPG2L0021, and CLRPG2L0022) at Chang Gung Memorial Hospital for study design and monitor, data analysis and interpretation.
Ethical considerations
This study was in compliance with the Helsinki Declaration and approved by the institutional review board of Chang Gung Memorial Hospital. Written inform consent were waive by the institutional review board of Chang Gung Memorial Hospital. We analyzed a pre-collected dataset that had been de-identified to ensure anonymity and protect the privacy of the participants. All patient data were handled in strict compliance with ethical guidelines to maintain confidentiality and ensure that no individual could be identified from the data used in this study.
Authors contributions
Dave W. Chen: guarantor of integrity of the entire study; study concepts; study design; definition of intellectual content; clinical studies; data analysis; statistical analysis; manuscript preparation; manuscript editing; manuscript review; Chih-Chien Hu: literature research; experimental studies; data acquisition; data analysis; statistical analysis; manuscript preparation; Yu‐Yi Huang: clinical studies; data acquisition; data analysis; statistical analysis; study design; manuscript editing; manuscript review; Pin-Ren Huang: study design; definition of intellectual content; clinical studies; data analysis; Ngi-Chiong Lau and Ching-Wei Hu: clinical studies; data analysis; statistical analysis; manuscript preparation; manuscript review
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All of the data supporting underlying findings are included in the manuscript and its supplemental files.
Supplemental material
Supplemental material is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.