
Abstract
Level of Evidence
Level III – Retrospective Cohort Study.
Background
Musculoskeletal lesions commonly present as pain, masses, or incidental imaging findings. Accurate diagnosis is critical for treatment planning. Although open biopsy was historically considered the gold standard, core needle biopsy (CNB) has emerged as a minimally invasive and reliable diagnostic method with a favorable safety profile. The primary objective was to determine the diagnostic accuracy of image-guided core needle biopsy (CNB) for musculoskeletal lesions.
Methods
We conducted a retrospective analysis of 426 patients who underwent image-guided CNB for musculoskeletal lesions at a single tertiary referral center between January 2014 and December 2020. Patient demographics, biopsy characteristics, and diagnostic outcomes were analyzed. Diagnostic performance was evaluated using sensitivity, specificity, predictive values, and area under the ROC curve (AUC).
Results
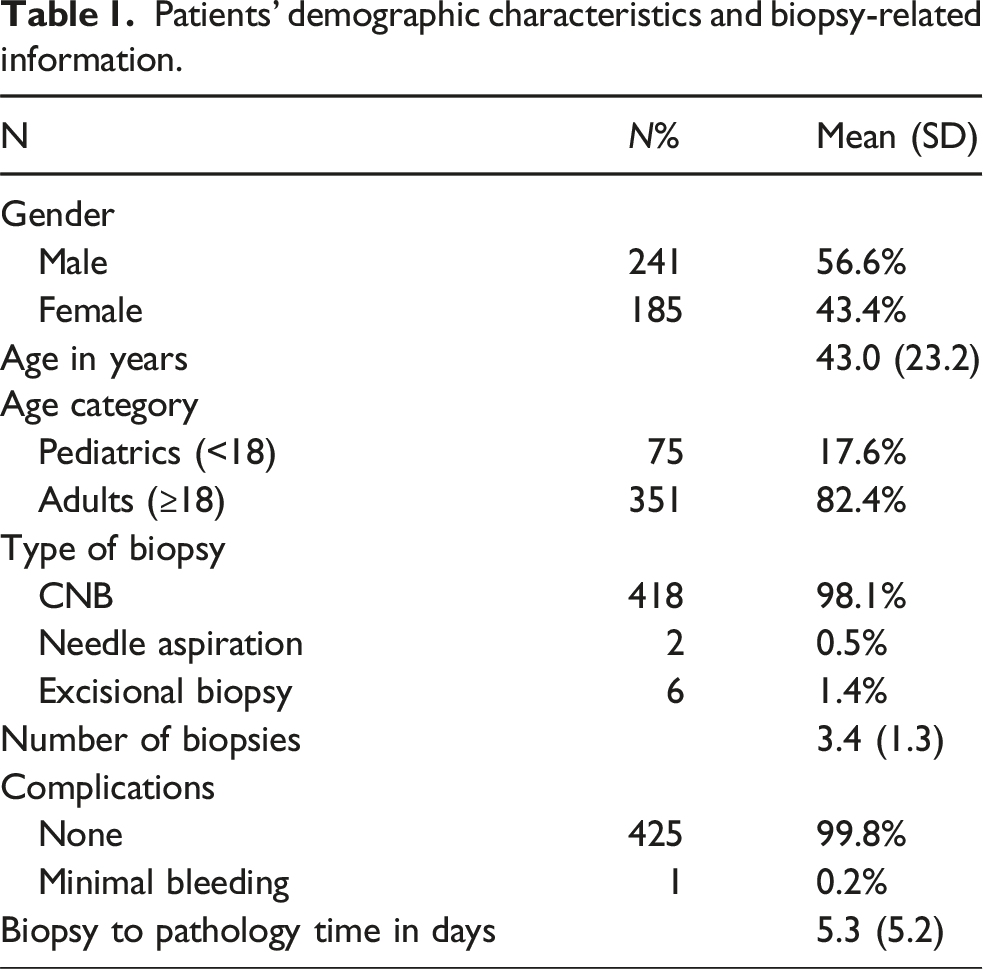
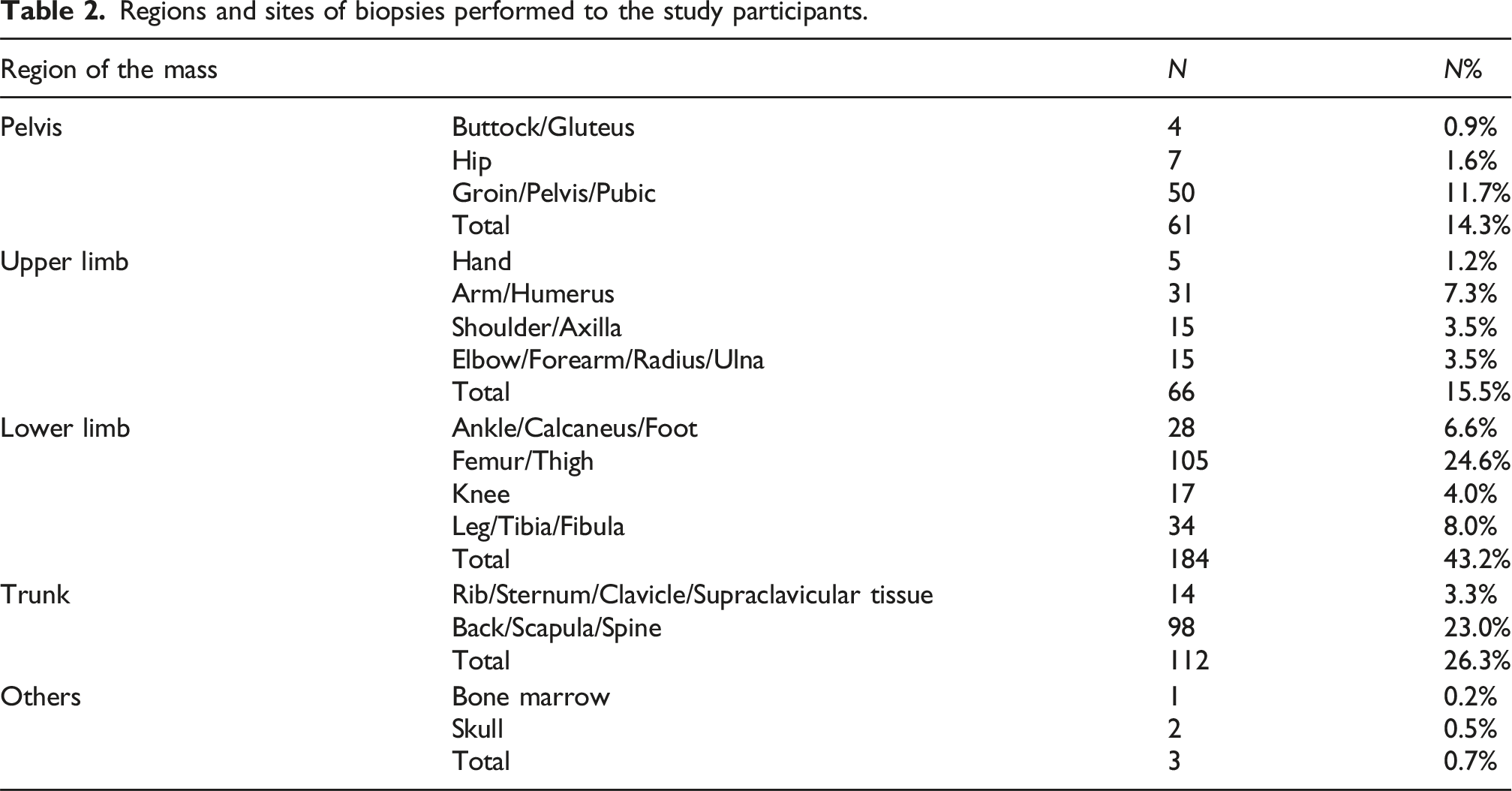
Most patients were adults (82.4%) and male (56.6%). The lower limb was the most common biopsy region (43.2%), with the trunk (26.3%), upper limb (15.5%), and pelvis (14.3%) following in order of frequency. CNB demonstrated a sensitivity of 98.8%, specificity of 72.3%, negative predictive value of 99.0%, and overall accuracy of 82.3% (AUC = 0.855).
Conclusion
Image-guided CNB provides high diagnostic sensitivity and excellent negative predictive value for musculoskeletal lesions, with a very low complication rate. While it is effective as a first-line diagnostic tool, limitations remain in specificity and tumor subtype confirmation, particularly in heterogeneous or necrotic lesions. Standardized protocols and multidisciplinary interpretation are essential to optimize accuracy.
Introduction
Musculoskeletal tumors, including sarcomas, represent a diverse group of rare mesenchymal neoplasms that require accurate and timely diagnosis to guide treatment decisions. While these lesions may present as pain-inducing masses, benign soft tissue abnormalities, or incidental findings on imaging studies, distinguishing between benign and malignant pathologies is critical to avoid overtreatment or delayed management. Proper histopathological diagnosis is particularly crucial in the context of musculoskeletal oncology, where treatment strategies—including surgery, radiation, and systemic therapy—depend heavily on the tumor’s type, grade, and location. 1
Historically, open incisional biopsy was considered the gold standard for diagnosing musculoskeletal tumors. This technique offers high diagnostic accuracy, often reported between 91% and 99%, due to the ability to obtain larger and more representative tissue samples.2–4 However, open biopsy carries several limitations, including the need for general anesthesia, the use of operating room resources, prolonged recovery, and higher risks of complications such as hematoma, infection, or tumor seeding along the biopsy tract.5–9 Furthermore, open biopsy may delay diagnosis and increase healthcare costs, especially when performed inappropriately or in non-specialized centers. In response to these challenges, other methodologies have grown in popularity.6,7 In contrast, image-guided core needle biopsy (CNB) has gained widespread adoption as a minimally invasive diagnostic alternative. CNB can be performed in radiology suites using modalities such as ultrasound, computed tomography (CT), or magnetic resonance imaging (MRI), and often requires only local anesthesia. This allows for outpatient-based procedures with minimal patient burden, reduced complication rates, and lower overall costs.4,6,7,9–13 Importantly, CNB can be used to obtain adequate tissue samples for histopathologic, immunohistochemical, and molecular analysis, providing sufficient diagnostic information in most cases. Nevertheless, certain potential negatives include the possibility of a decline in diagnostic accuracy as well as the possibility of a mistake occurring during the tumor sample. 5
Numerous studies have reported diagnostic accuracy rates of CNB between 66 and 98%, depending on lesion location, imaging modality used, operator experience, and institutional protocols.10,11,14–24 Meta-analyses have demonstrated that CNB yields high diagnostic accuracy and outperforms fine-needle techniques in both benign and malignant bone tumors.12,24 These results have led to CNB being recommended as a first-line biopsy method in many clinical guidelines, especially when performed in specialized musculoskeletal oncology centers. Despite its advantages, CNB is not without limitations. Concerns remain regarding sampling error, non-representative tissue acquisition, or inconclusive results due to necrotic or fibrotic lesions. In particular, certain anatomical locations or tumor subtypes may pose challenges to accurate diagnosis using CNB alone. 10
Another important consideration is the complication profile of CNB compared to open biopsy. Studies have shown that CNB has significantly lower complication rates, often reported as 0–2%, whereas open biopsy complications can reach up to 16%.4,6,7,9 Common minor complications include localized bleeding, hematoma, or transient pain, while major complications such as infection, neurovascular injury, or tumor seeding are exceedingly rare with proper technique. Additionally, the smaller incision used in CNB can often be incorporated into the definitive surgical approach, minimizing the impact on future procedures.4,6,7,25
In clinical practice, the utility of CNB is also evident in its impact on time-to-diagnosis. With reduced need for operating room scheduling and hospital admission, CNB allows for faster turnaround from initial imaging to treatment planning.11,17–21 This is particularly valuable in high-volume tertiary care settings, where resource optimization and patient throughput are priorities.4,6,7
Despite the growing evidence supporting core needle biopsy, several gaps remain in the literature. Many prior studies are limited by small sample sizes or combine bone and soft tissue lesions, which may reduce generalizability. In addition, inconsistent reporting of nondiagnostic or inadequate samples can lead to overestimation of diagnostic accuracy. Regional data, particularly from Middle Eastern populations and healthcare systems that rely on centralized tertiary care models, are also scarce. Therefore, there is a need for large, single-center studies that comprehensively report the diagnostic accuracy and safety profile of image-guided CNB for musculoskeletal lesions.
Given these limitations, this study aims to evaluate the diagnostic accuracy, complication rate, and procedural characteristics of image-guided core needle biopsy for musculoskeletal lesions at a high-volume tertiary referral center. We present a retrospective analysis of 426 consecutive patients who underwent CNB for suspected bone or soft tissue tumors, using standardized radiologic guidance and pathology evaluation. Our primary objective was to determine the diagnostic sensitivity, specificity, and overall accuracy of CNB. Secondary objectives included analysis of complication rates, time to diagnosis, and the impact of factors such as lesion location, patient age, and tissue type (bone vs soft tissue) on diagnostic yield.
We hypothesize that CNB provides a high level of diagnostic accuracy comparable to open biopsy, with significantly lower complication rates and better logistical efficiency. By analyzing a large and diverse patient cohort, we aim to validate the use of image-guided CNB as a reliable diagnostic modality in musculoskeletal oncology and support its integration into diagnostic algorithms in tertiary care environments.
Materials and methods
This study was approved by the Institutional Review Board and conducted in accordance with the Declaration of Helsinki. 26 The potential benefits and risks of CNB were explained to all patients before the procedure, and the study adhered to STROBE guidelines for reporting observational research. 27
Study design
This retrospective study was performed between January 2014 and December 2020. All medical records from all patients who underwent CNB for a musculoskeletal mass were reviewed.
Data collection method
The data were collected retrospectively in a structured electronic data sheet. The data included patients’ demographics, operative-related data, diagnostic accuracy of CNB, and complications. All patients who underwent image-guided core needle biopsy for suspected bone or soft tissue lesions between January 2014 and December 2020 were eligible for inclusion. Patients were included if they had complete demographic, imaging, and histopathological data available. Patients were excluded if they had incomplete medical or pathology records; if they had undergone open or excisional biopsy as the initial diagnostic procedure; or if their CNB samples were nondiagnostic without subsequent confirmatory follow-up. Nondiagnostic CNB samples without a confirmed final diagnosis were excluded from accuracy calculations because diagnostic metrics require comparison against a verified reference standard. The average time from biopsy to pathology was 5.3 days, and there were no significant procedural complications observed. All image-guided core needle biopsies, whether targeting soft tissue or bone lesions, were performed under local anesthesia using standard aseptic technique.
Statistical analysis
Continuous normally distributed data were reported as mean and standard deviation (SD). Receiver operating characteristic (ROC) curve and area under ROC curve (AUC) were used to assess the diagnostic accuracy of core needle biopsy for musculoskeletal lesions. The sensitivity, specificity, positive predictive value (+PV), negative predictive value (-PV), positive likelihood ratio (+LR), and negative likelihood ratio (-LR) were calculated. All tests were considered significant when p < 0.05. Statistical analysis was performed using SPSS software version 25 for Windows (SPSS Inc., Chicago, IL, USA) and MedCalc software version 20.28,29
Results
Patients’ demographic characteristics and biopsy-related information.
Regions and sites of biopsies performed to the study participants.
With a sensitivity of 98.8%, CNB could accurately diagnose 98.8% of patients with the intended ailment. With a specificity of 72.3%, CNB could accurately classify 72.3% of patients as not having the target condition. 68.4% of patients who tested positive for the target ailment had it, according to the positive predictive value of CNB. 99.0% of patients who tested negative for the target condition did not have it, according to the CNB’s negative predictive value of 99.0%. With an accuracy of 82.3%, CNB could properly identify the target condition in 82.3% of the patients. As evidenced by its area under the curve (AUC) of 0.855 (95% CI 0.819-0.892), CNB was a very reliable predictor of the intended condition. Figure 1 and Table 3 present the CNB diagnostic test accuracy metrics. Receiver Operating Characteristics (ROC) curve displaying diagnostic utility and Area Under the Curve (AUC) for CNB (AUC = 0.855). CNB diagnostic test accuracy parameters.

Comparison of CNB diagnostic accuracy according to gender, age, and tissue type.

Specimen adequacy and repeat biopsies
Specimen adequacy was assessed for all CNB cases. A total of 11 biopsies (2.6%) were categorized as nondiagnostic or inconclusive. Among the nondiagnostic or inconclusive CNBs, seven patients (63.6%) required a repeat biopsy. Of these, 5 underwent repeat CNB and 2 proceeded directly to open biopsy. Definitive diagnoses were achieved in 3 of these repeat-biopsy cases.
Discussion
The results of this study provide convincing evidence regarding the diagnostic utility of percutaneous core needle biopsy (CNB) for musculoskeletal lesions. Our comprehensive assessment highlights the advantages of CNB as a minimally invasive and reliable alternative to open biopsy. In our cohort, CNB demonstrated an overall diagnostic accuracy of 82.3%, which is consistent with the literature and supports its clinical value.4,11,17–21,30–32 These findings contribute meaningfully to the growing body of evidence supporting the use of percutaneous techniques for obtaining accurate histopathologic diagnoses in a broad range of musculoskeletal tumors. Nonetheless, the modest specificity and positive predictive value indicate that CNB is more reliable for excluding malignancy than for precisely defining tumor subtype. This study is in alignment with findings by Siddiqi et al., who compared fine-needle aspiration with core needle biopsy and found CNB to be more effective in providing definitive tissue characterization. Similarly, previous studies have demonstrated that CNB provides dependable diagnostic information while minimizing patient morbidity.33–35 However, certain sarcomas with necrosis, fibrosis, or heterogeneous architecture may be challenging to grade accurately using CNB alone. In such cases, an open biopsy or repeat CNB may still be necessary, and CNB findings should ideally be reviewed within a multidisciplinary team setting to support shared decision-making and ensure optimal diagnostic accuracy. Pediatric patients represented a relatively small proportion of our cohort (17.6%); therefore, the findings in children may not fully represent the broader pediatric population. An important aspect of this analysis was the comparison of complication rates between CNB and open biopsy methods. In our cohort, the complication rate associated with CNB was minimal, with only one minor bleeding episode (0.2%). This is substantially lower than the complication rates reported in some open biopsy series, which can range up to 16%.4,6,7 These results reinforce the established notion that percutaneous approaches are safer and less invasive, offering a favorable safety profile that supports broader clinical adoption. Azabdaftari et al. emphasized the growing interest in CNB due to its safety and efficiency in the diagnosis of musculoskeletal lesions. 35 Reduced complication rates not only improve patient safety but also facilitate a smoother and faster recovery. This, in turn, minimizes the burden on healthcare systems and improves the overall patient experience. Another advantage of CNB observed in our study was the significantly shorter hospital stay. Patients undergoing CNB had an average hospital stay of 1.5 days, compared to longer admissions often associated with open biopsy procedures. 32 This reduction in hospitalization enhances patient satisfaction and supports earlier recovery. These practical benefits align with the ongoing shift toward less invasive diagnostic strategies in orthopedic oncology. The quick recovery time associated with CNB also highlights its value in clinical workflows. Faster post-biopsy recovery facilitates earlier treatment planning, reduces delays, and may contribute to improved oncologic outcomes. Moreover, the use of CNB promotes more efficient utilization of operating rooms and inpatient beds, which is particularly beneficial in high-volume tertiary centers. With regard to lesion location, the lower limb was the most commonly biopsied region in our cohort. However, accuracy remained high across all anatomical sites, suggesting that CNB maintains its diagnostic utility regardless of biopsy site when performed in specialized centers. Despite the strengths of this study, some limitations should be acknowledged. Excluding nondiagnostic, unconfirmed biopsies likely increased the measured diagnostic accuracy and may not represent true clinical performance in all cases. The retrospective nature of the study may introduce selection bias, and the single-center design may limit the generalizability of the findings. Additionally, our patient population may not reflect the broader diversity of patients seen in other regions or healthcare systems. Future prospective, multicenter studies are needed to validate our findings and compare CNB directly with open biopsy under standardized protocols.
Conclusion
Image-guided CNB provides high diagnostic sensitivity and excellent negative predictive value for musculoskeletal lesions, with a very low complication rate. While it is effective as a first-line diagnostic tool, limitations remain in specificity and tumor subtype confirmation, particularly in heterogeneous or necrotic lesions. Standardized protocols and multidisciplinary interpretation are essential to optimize accuracy.
Footnotes
Acknowledgment
We would like to thank Suhair Ayman Altramsy for her significant contributions and for drawing the illustrations of the surgical procedure presented in the present study.
Ethical considerations
All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent for publication
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Author contributions
Each author took part in formulating the research idea, plan the study, and collect the data. All authors were responsible for assessing the quality of the included data, doing data analysis, and writing the manuscript. All authors agree to accept equal responsibility for accuracy of this paper and approve the publication of the final manuscript. We have no financial interest linked to this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used in the present study are available from the corresponding author on reasonable request.