
Abstract
Purpose
This study investigates the efficacy of antibiotic-loaded bone cement followed by autogenous iliac bone grafting in managing subacute/chronic phalangeal osteomyelitis (OM), focusing on infection eradication, reconstruction of bone defects, and functional restoration.
Methods
We conducted retrospective analysis involving 14 patients treated between September 2007 and November 2023, with a mean follow-up duration of 18.21 months. The treatment protocol involved staged procedures, beginning with debridement and bone cement insertion, followed by cement extraction and autogenous bone grafting.
Results
Complete infection resolution was achieved for all patients, and radiological evidence of bone union was observed within an average of 46.93 days. Bone defects measured between 10 and 30 mm; most patients received cancellous bone grafts, although cortico-cancellous grafts were utilized in four cases. Functional outcomes, evaluated through the Quick disabilities of the arm, shoulder, and hand questionnaire, demonstrated marked improvement (49.78→10.33). The mean total active motion of the affected digits was 82.14%, with a majority attaining functional use. No cases of recurrent infection were identified, and the staged surgical method demonstrated effectiveness for digit preservation, including those with bone loss exceeding 10 mm.
Conclusion
The authors suggest antibiotic-loaded bone cement insertion followed by autogenous iliac bone grafting can be a highly reliable and reproducible intervention for subacute/chronic phalangeal OM. We advocate this approach as a treatment option for phalangeal OM.
Introduction
Osteomyelitis (OM) is a pyogenic infection affecting bone tissue. It may originate from direct inoculation, contiguous spread from adjacent soft tissues, or via the hematogenous route. In the hand, direct trauma is recognized as the predominant cause of OM. 1 The standard management principles for OM of the hand include extensive, surgical debridement of involved bone and 4 to 6 weeks of culture-directed antibiotic therapy.2,3 If these measures are unsuccessful or OM persists, amputation of the affected digit is routinely considered. Although amputation remains a widely used definitive intervention, it results in irreversible loss of hand function. Reilly et al. 1 noted that extended efforts to salvage digits particularly using staged reconstruction with segmental bone grafts have rarely been successful. They also recommended consideration of early amputation in refractory cases. Thus, achieving digit salvage and reconstruction in OM presents a more technically demanding clinical scenario but represents a substantial therapeutic accomplishment.
To date, even after digit salvage and successful infection control, achieving bone union with a conventional bone graft in a 2nd staged operation remains challenging. As a result, reconstruction utilizing vascularized bone grafts has generally been accepted as the standard procedure.4,5 Recently, more sophisticated, accessible, and technically demanding surgical methods for the management of OM have been introduced. Among these, the Masquelet technique is a straightforward two-stage approach developed for the reconstruction of long bone defects. 6 While its application in hand surgery has been limited, it has demonstrated favorable outcomes in available reports.7–11 Nonetheless, most reports are limited to case descriptions, and comprehensive studies addressing the management of OM are scarce.
We report clinical outcomes and a surgical technique for treating subacute/chronic phalangeal OM in the hand, which involves radical debridement, temporary antibiotic-loaded bone cement placement, staged iliac cancellous autograft transplantation, and non-rigid fixation. The authors’ findings aim to support hand surgeons in optimizing outcomes for phalangeal OM in the hand.
Material and methods
Patients
This study was approved by the institutional review board at Jeonbuk National University Hospital (CUH 2025-07-018-001).
A retrospective analysis was performed on 14 patients diagnosed with phalangeal OM who underwent a staged treatment protocol. This protocol involved initial debridement followed by bone cement insertion, and subsequently, the removal of the cement and autologous iliac bone grafting, all carried out by the first author. The first three cases were treated between September 2007 and January 2009, while the remaining 11 cases were treated from April 2018 to November 2023. Inclusion criteria were as follows: (1) patients with a confirmed diagnosis of subacute or chronic phalangeal OM based on clinical, radiological, and histopathological evaluations; (2) treatment through a staged surgical procedure that began with debridement and bone cement insertion, followed by cement removal and autologous iliac bone grafting; and (3) completion of follow-up until infection eradication was confirmed, as indicated by clinical signs and cultures taken during the second-stage operation. Exclusion criteria included: (1) patients who did not receive staged treatment for phalangeal OM; and (2) patients who did not complete follow-up until infection eradication was confirmed.
Demography of the patients.
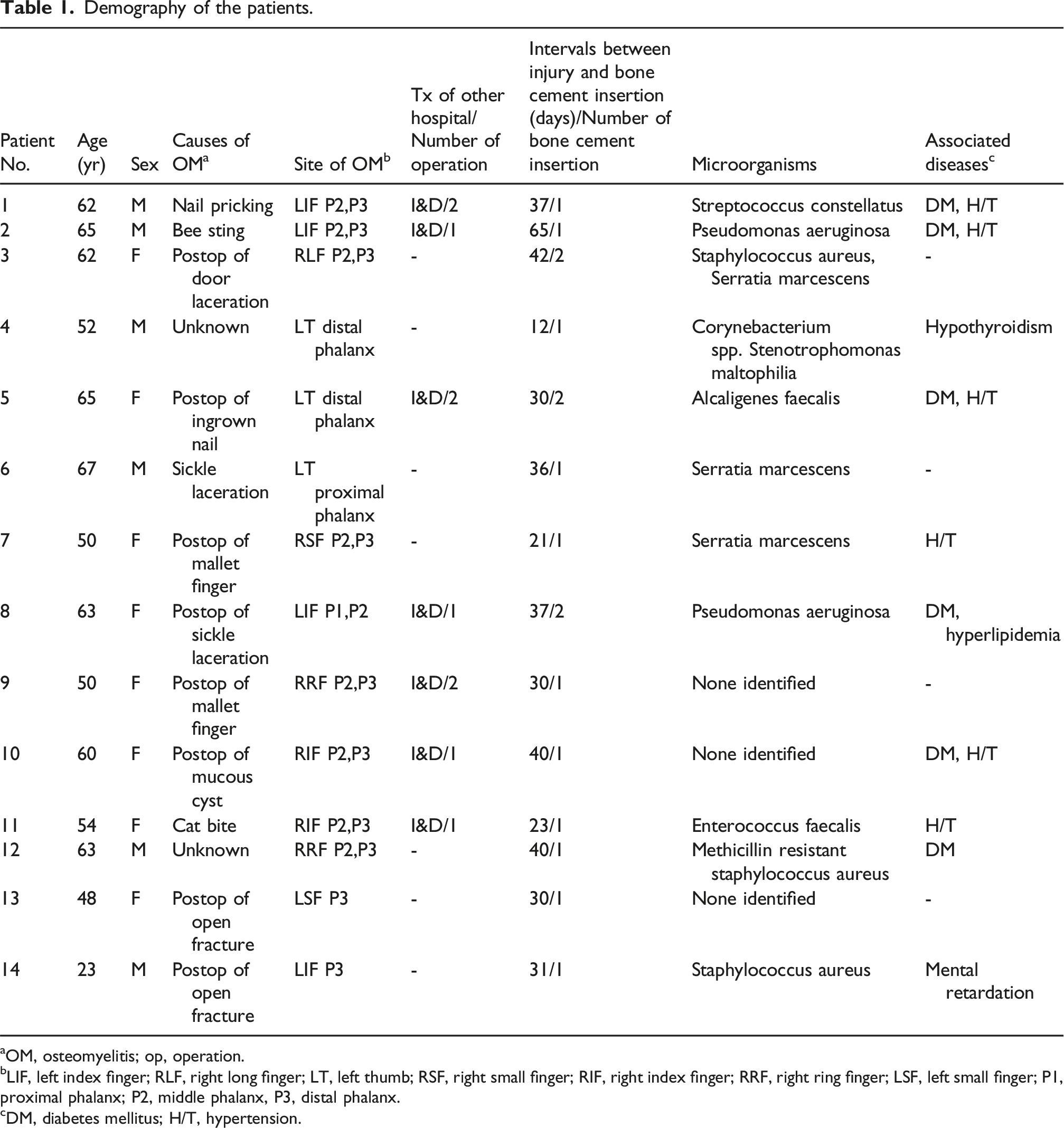
aOM, osteomyelitis; op, operation.
bLIF, left index finger; RLF, right long finger; LT, left thumb; RSF, right small finger; RIF, right index finger; RRF, right ring finger; LSF, left small finger; P1, proximal phalanx; P2, middle phalanx, P3, distal phalanx.
cDM, diabetes mellitus; H/T, hypertension.
Intraoperative findings in the initial bone cement insertion surgery of the patients.

Treatment details and outcomes.
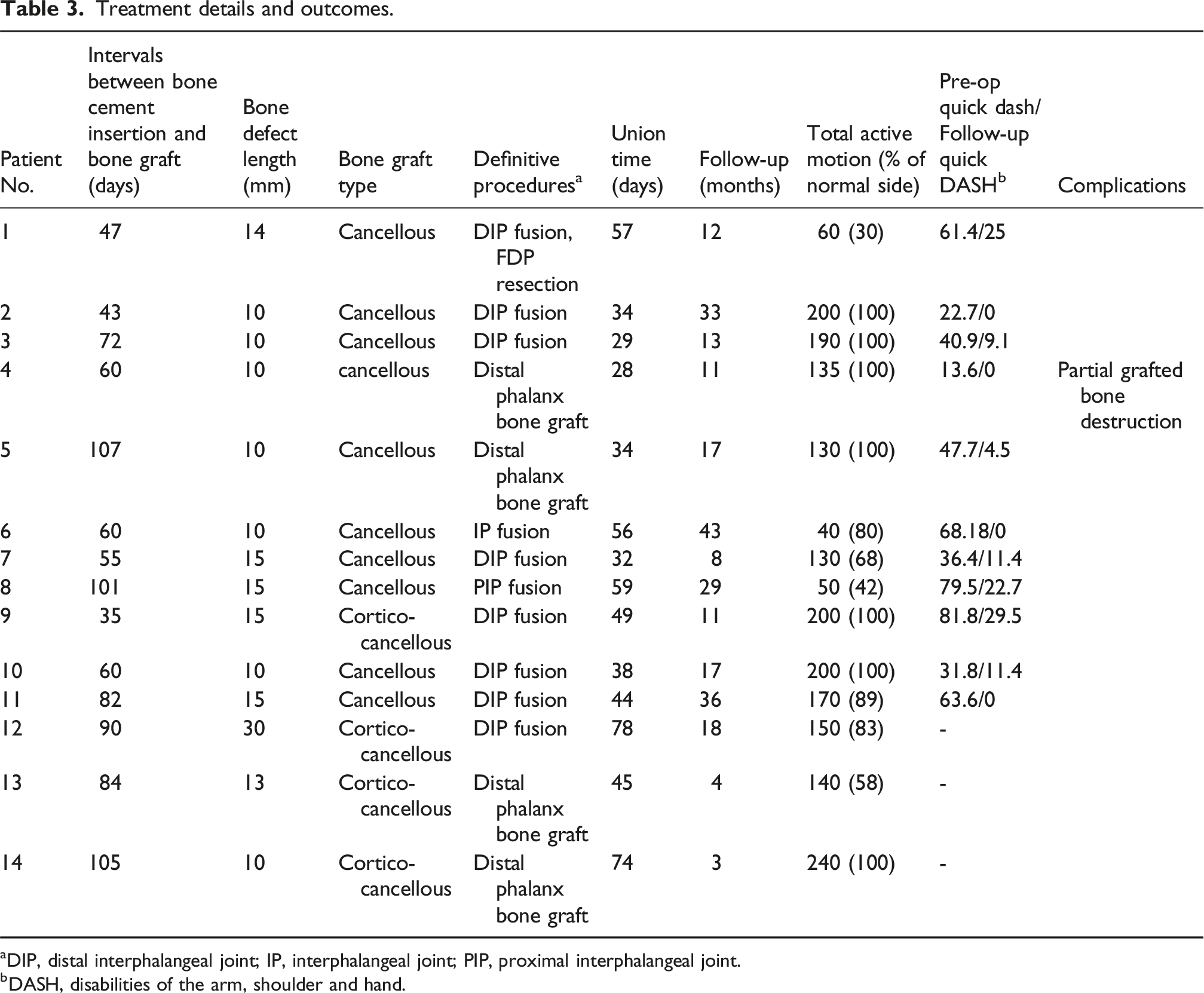
aDIP, distal interphalangeal joint; IP, interphalangeal joint; PIP, proximal interphalangeal joint.
bDASH, disabilities of the arm, shoulder and hand.
Surgical technique
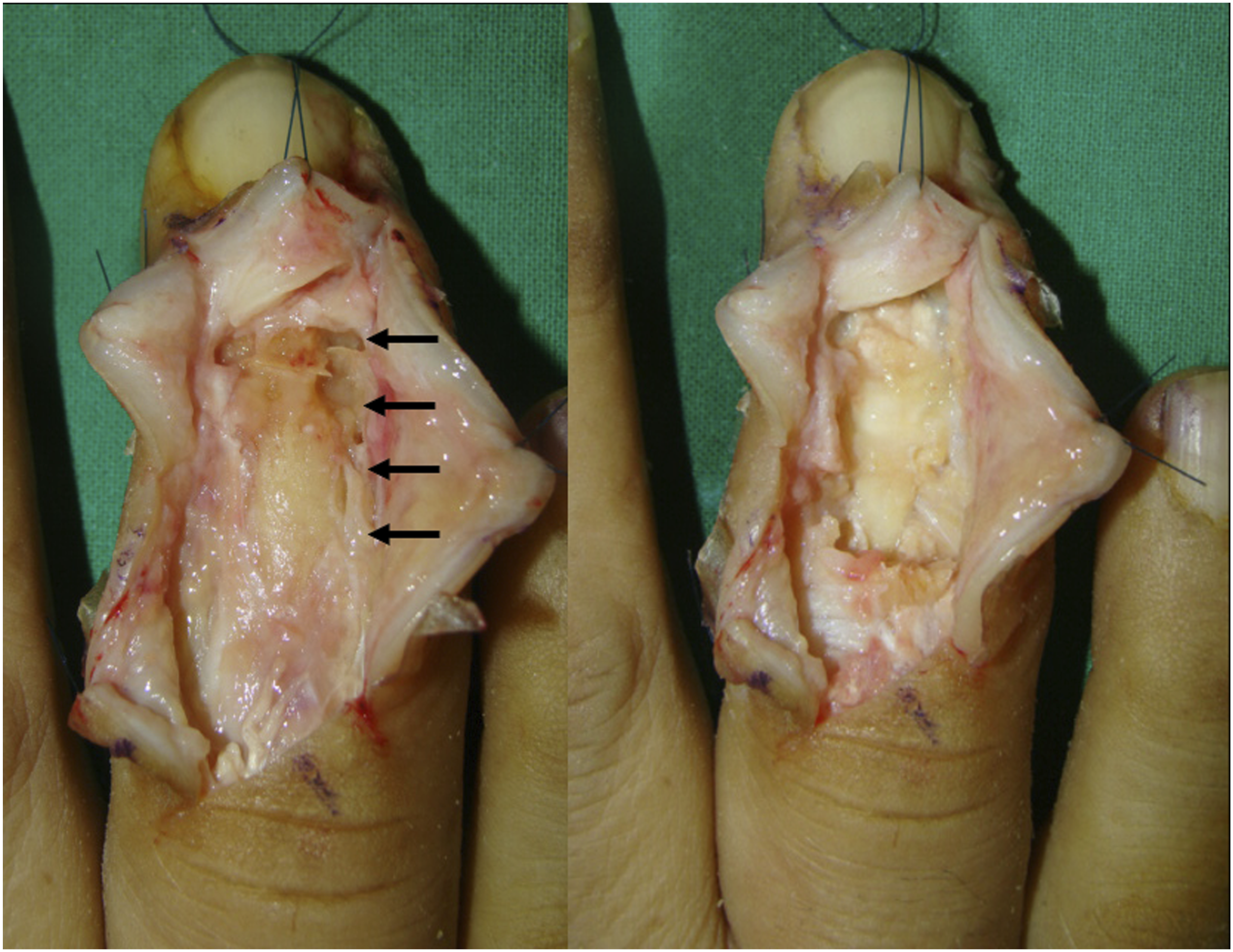
The operation was conducted using regional anesthesia, with patients positioned supine and the operative arm supported on a hand table. A pneumatic tourniquet was placed around the upper arm. The type of skin incision depended on the OM location and any previous incisions from I&D at a different facility. However, a Y-shaped or zig-zag incision was generally utilized on the dorsal side of the finger (Figure 1). Intraoperative assessment indicated that sites exhibiting cortical erosion on preoperative radiographs had experienced progressive bone loss. Active purulent fluid accumulation was identified in five cases. Postoperative OM patients showed additional bone destruction and the presence of infected granulation tissue internally and around the necrotic bone (Table 2). We carried out extensive debridement, excising both the damaged bone and infected soft tissue and obtained cultures (Figure 2). The flexor tendon sheath was preserved in cases where there were no signs of infection. Debridement involving the FDP tendon was required for one patient due to preexisting tendon damage. Four cases of distal phalanx involvement were stabilized without Kirschner (K) wires, while ten cases with phalangeal joint involvement received K-wire fixation prior to cement insertion. The remaining defect was packed with 2 g tobramycin loaded polymethylmethacrylate (DePuy Synthes, New Jersey, USA) combined with 2 g vancomycin (Figure 3). (a) Preoperative RRF images of Patient 12 (left) and a plain posteroanterior (PA) radiograph of the RRF (right) reveal swelling below the middle phalanx and bone destruction near the DIP joint. (b) Preoperative LIF plain PA radiograph (left), and a T2 weighted MRI scan image (right) of Patient 2. There is visible bone destruction at the DIP joint. After excision of the extensor tendon in Patient 12, partial bone destruction of the middle and distal phalanges was observed (arrows, left). Images following debridement are shown (right). (a) Intraoperative image of Patient 12 depicting bone cement used for augmentation of a bony defect (asterisk). (b) Intraoperative photograph of Patient 2 (left) and postoperative plain PA radiograph of LIF (right) displaying bony defect fixation using K-wires in combination with bone cement insertion.

After the initial surgery, a short arm splint was applied. On the first postoperative day, the silicon drain was removed, and the patient received 2 g of first-generation cephalosporin intravenously twice daily. Once the culture results were available, a consultation with the infectious disease department was requested, leading to the administration of additional suitable intravenous antibiotics for 2 weeks based on the identified bacteria. Upon discharge at 2 weeks postoperatively, the intravenous antibiotics were switched to oral antibiotics, which the patient continued for an additional 4 to 6 weeks. One week later, the initial short arm splint was replaced with a finger splint. Sutures were removed 2 weeks after surgery for all patients, and plain radiographs were taken weekly to monitor the condition of the finger. Complete resolution of edema, pain, and redness indicated the eradication of infection, prompting the extraction of the fixed K-wires in the outpatient clinic at 4 weeks postoperatively. Bone grafting was scheduled for 2 weeks after the pin removal, or 6 weeks following the placement of bone cement. In the second stage, the procedure was performed under general anesthesia. Four patients received cortico-cancellous bone grafts, whereas ten patients received cancellous bone grafts harvested from the iliac bone. The surgical incision followed the previous operative scar. Bone cement placed during the initial procedure was excised, and debridement proceeded down to the bone marrow, exposing new bone at the proximal and distal margins of the defect. Intraoperative cultures were also collected. In seven patients with DIP and thumb IP fusion, a single 0.9 mm K-wire was inserted to stabilize the bone prior to the cancellous bone graft procedure (Figure 4(a)). In one patient with PIP joint fusion, two crossed K- wire fixations were performed. For two patients who received distal phalanx cancellous bone grafts, K-wire fixation was omitted, and a finger splint was applied. In four cases with cortico-cancellous bone grafts, stable fixation of the proximal and distal bone ends was achieved with K-wires (Figure 4(b)). (a) Intraoperative image from Patient 2 (left) and a LIF plain PA radiograph (right) demonstrate a cancellous bone graft located at the bone defect site. (b) Intraoperative image from Patient 12 (left) and RRF plain PA radiograph (right) demonstrate cortico-cancellous bone graft placement at the area of bone defect, with fixation using multiple K-wires.
Post-bone grafting, a short arm splint was reapplied, and intravenous antibiotics, identical to those used during the initial surgery, were continued for 1 week. The short arm splint was replaced with a finger splint 1 week postoperatively, allowing for the initiation of metacarpophalangeal joint mobilization. Sutures were removed at 2 weeks, and weekly plain radiographs were obtained to monitor healing. K-wires were removed upon confirmation of bone union. All patients were then instructed to perform active ROM exercise for the involved joint carefully, avoiding excessive passive manipulation.
Clinical evaluation
Postoperative clinical evaluation of OM consisted of physical examination and review of plain radiographs. ESR and CRP levels are typically elevated in acute OM, but they are not commonly elevated in chronic OM. Therefore, ESR and CRP levels do not correlate with the final clinical outcome. 12 Thus, lab tests for ESR and CRP were not used to confirm infection status. Clinical cure of infection was defined as the absence of swelling, pain, and tenderness in the affected finger, along with no bacterial growth in the microbiologic culture performed during the second-stage operation.
Bone union was determined by the absence of tenderness at the bone grafting sites and, radiologically, by assessing finger posteroanterior (PA), lateral, and oblique views. Union was indicated by the disappearance of the fracture line and the presence of trabecular bone across the grafted area on at least two views. 13 We evaluated active ROM of the affected finger by comparing the percentage of total active motion (% TAM) to that of the unaffected side at final follow-up. For cases with PIP or DIP joint fusion, the ROM of these joints was excluded from the %TAM calculation. 14 Functional outcomes were assessed in 11 patients using Quick disabilities of the arm, shoulder and hand (DASH) scores, measured preoperatively and at final follow-up. Quick DASH data were unavailable for three patients. 15
Statistical analysis
For statistical analysis, IBM SPSS version 20.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. The paired t-test was conducted compare preoperative and follow-up Quick DASH scores which follow normal distribution, confirmed with Shaprio-Wilk test. A p- value <0.05 was considered statistically significant. 16 A nonparametric regression analysis using a generalized additive model was conducted to evaluate the relationships between the duration from symptom onset to surgery, the interval from bone cement insertion to bone grafting, and the size of the bone defect with bone union time. Additionally, a subgroup analysis comparing fixation methods and graft types was performed using the Mann-Whitney U test.
Results
The mean duration of follow-up was 18.21 (±12.33) months (range, 3–43 months). Cultures taken during the second stage of the operation showed no bacterial growth in any of the patients. Furthermore, the induced membrane was well matured in all patients at this stage of the operation. All affected fingers were preserved, with no persistent infection or recurrence of OM observed. Radiographic bone union was achieved in all patients at an average of 46.93 (±16.08) days (range, 28–78 days) after bone graft surgery (Figure 5). In the generalized additive model analysis, neither the duration from symptom onset to surgery nor the interval from bone cement insertion to bone grafting showed statistically significant results (p = 0.556 and p = 0.293, respectively). In contrast, bone defect size demonstrated a borderline linear association with bone union time (p = 0.056) (adjusted R2 = 0.326, deviance explained = 50.7%). In subgroup analyses, the comparison between the K-wire fixation subgroup and the non-fixation subgroup yielded no statistically significant difference (p = 0.100). Additionally, the comparison between the cancellous bone grafting subgroup and the cortico-cancellous subgroup yielded borderline but not statistically significant result (p = 0.056). The mean value of %TAM was 82.14 (±23.85) % (range, 30–100) (Figure 6). Although ten patients demonstrated more than 80% TAM, lower values of 42% and 30% were observed in patients who underwent PIP joint fusion and those who underwent both DIP fusion and FDP resection, respectively. The patient who underwent a distal phalanx bone graft and had a TAM value of 58% likely had a short final follow-up period of only 4 months after surgery. The average quick DASH score improved from 49.78 (±22.81) preoperatively to 10.33 (±10.96) at the final follow-up, representing a statistically significant improvement (p = 0.000). One case of complication was noted. In a patient who underwent bone grafting of the distal phalanx of the left thumb, follow-up revealed discharge at the nail bed and partial radiographic destruction of the grafted bone (Table 3). However, treatment with dressings and avoidance of water immersion of the thumb for 2 weeks resulted in healing, with final follow-up confirming bone union (Figure 7). (a) Postoperative RRF AP (left) and lateral (right) plain radiographs of Patient 12 at 18 months (b) Postoperative LIF AP (left) and lateral (right) plain radiographs of Patient 2 at 33 months demonstrate complete and solid bone union. Postoperative clinical photograph of Patient 2 at 33 months illustrating improved functional outcomes. Postoperative Lt. thumb plain PA radiograph of Patient 4 at 2 weeks after bone graft (left); PA radiographs at 6 weeks post-bone graft (middle) reveal partial destruction of the grafted bone, and PA radiographs at 11 months (right) indicate solid bone union.


Discussion
It is established that the forefoot, toes, and lower extremities are the most frequently affected sites of OM. In the hand, OM predominantly arises as a complication subsequent to infection.17,18 Reilly et al., 1 in a cohort study involving 700 patients with hand infections, found that 7% progressed to OM of the hand. The majority of infections, 57% of cases, were attributed to direct trauma, while hematogenous spread accounted for 13% and continuous infection for 9% of patients. In this investigation, open wounds and open fractures were identified as the most prevalent causes of OM, observed in six patients. Four patients developed wound complications after surgical intervention, one patient suffered a cat bite, one patient had a bee sting, and two patients had unidentified causes. Importantly, the recognized etiologies, such as open wounds and fractures, usually resulted from relatively minor injuries. It is noteworthy that more than 70% of the patient cohort had comorbidities such as DM and H/T, with a mean age around 56 years, representing a generally active group. Furthermore, before their referral to our facility, seven patients had already undergone one or more I&D procedures elsewhere, yet infection persistence remained. Patient inattention to timely and adequate initial management of finger wounds was considered a contributing factor to OM development. In addition, even when wound care was initiated, it appears that primary care providers may not have employed an appropriately aggressive approach grounded in a comprehensive understanding of hand infection management and complications. As a result, ongoing and structured educational initiatives for physicians are warranted.
The Masquelet technique has recently received considerable attention as a therapeutic option for OM.6,17,19 Originally developed for managing post-traumatic septic nonunion of the leg, this technique involves a two stage surgical approach. The first stage involves aggressive debridement of infected and necrotic bone and soft tissue, followed by internal fixation of the bone gap. The resulting bone defect is subsequently packed with an antibiotic-loaded bone cement. During the second stage, performed no sooner than 6–8 weeks after insertion of the cement spacer, the spacer is removed and the defect is filled with substantial autogenous cancellous bone graft. Membranes formed around the cement spacer (induced membranes) have been demonstrated to secrete various growth factors that stimulate neovascularization, corticalization, and inhibit graft resorption. The concentrations of these bioactive factors within the membrane are reported to remain elevated for up to 4 weeks postoperatively and then gradually decline. On this basis, bone grafting within the induced membrane is optimally conducted at 4 weeks20,21
This approach was relatively uncommon in procedures involving the hand, as identified during a literature review. The review confirmed that only a small number of reported cases applied this technique in the hand region but presented successful clinical outcomes.7–11 Isenburg et al. 5 reported favorable outcomes from using a hemi-metatarsal vascularized bone graft in cases of OM following phalangeal fractures, particularly when severe bone loss persisted after controlling the infection. They proposed this technique as an efficient solution. Aimé et al. 22 achieved successful digital salvage in all cases of digital OM treated with a single-stage procedure that utilized an antibiotic-eluting, methylmethacrylate joint-spanning spacer. However, one case required a soft tissue flap, and two cases necessitated spacer removal due to malalignment. When comparing the Masquelet technique to other methods for treating phalangeal OM, including vascularized bone grafts and single-stage techniques, the Masquelet technique is noted for its advantages in bone reconstruction and its surgical simplicity, as it does not require microsurgery.4,5,22
The authors did not strictly follow the guidelines of the Masquelet technique during the surgery. In orthopedic practice, antibiotic-loaded bone cement has typically been utilized for infection control. Consequently, the authors selected bone cement for both infection management and to prevent bone defect collapse. Furthermore, we experienced in managing traumatic nonunion in the hand using autogenous iliac cortico-cancellous bone graft in several cases. 23 As a result, cortico-cancellous bone grafts were employed in the initial four patients. A limitation of cortico-cancellous bone graft procedures is the necessity for secure fixation of the graft in contact with the phalangeal bone. Subsequently, during the management of scaphoid nonunion with arthroscopy, we observed that stable bone union could be achieved using cancellous bone graft alone, even in the intra-articular environment of the scaphoid. This observation prompted a transition to utilizing cancellous bone grafting exclusively. 24 In the subsequent ten cases, satisfactory outcomes were achieved by performing cancellous bone grafting while preserving only the length and rotational alignment of the digit, without the need for rigid fixation. Additionally, we have had numerous successful experiences achieving adequate stability and bone union through K-wire fixation in previous studies.23,24 Thus, we standardized the fixation method to K-wire fixation. In two cases involving the distal phalanx and using only cancellous bone grafts, we achieved stability and bone union solely through the application of a finger splint.
In the Masquelet technique, only cancellous bone grafts are utilized. Although the surgical procedure described by the authors does not entirely align with the classic Masquelet technique, both methods share the key feature of bone grafting within the induced membrane. A direct comparison with the Masquelet technique could provide important insights for advancing treatment approaches. Importantly, the Masquelet technique does not specifically address the use of cortical bone grafts within the membrane, and their advantages have not yet been comprehensively investigated. 25 Nevertheless, the authors reported favorable outcomes in four cases using cortico-cancellous grafts and in two additional cases where cortical fragments were incorporated with cancellous bone to support the nail bed. In the subgroup analysis of our study, there was no significant difference in bone union time between the cancellous group and cortico-cancellous group. Proubasta et al. 11 and Pruzansky et al. 9 similarly documented positive results with cortico-cancellous bone grafts. Therefore, cortico-cancellous bone grafts, along with cancellous bone, are deemed effective for use in the hand.
Regarding the bone graft donor site, post-operative pain following iliac bone grafts is indeed reported as a source of morbidity; however, this pain typically resolves during the recovery process. 26 Thus, in hand lesions, grafts are often harvested from the distal radius to reduce donor site morbidity. However, studies have reported that the abundance of fibroblasts in iliac cancellous bone is superior to that in the distal radius. 27 The present authors, having achieved positive outcomes with iliac cancellous bone grafts, have standardized the use of autologous iliac bone graft since confirming above reports on cellularity. To minimize donor site morbidity, the authors created a small, H- shaped opening on the iliac crest using an electrical saw (approximately 1 cm wide and 1 mm thick) and harvested only cancellous bone. Closure was accomplished by approximating the cortical bone and repairing the overlying soft tissues. The authors suggest that further research is needed on the use of bone graft substitutes to reduce donor site morbidity.
In the Masquelet Technique for bone graft fixation, rigid stabilization is usually recommended to prevent the risk of delayed stress fractures.19,25 However, since finger bone defects are typically smaller and the fingers are non-weight-bearing areas, we propose that K-wire fixation is adequate to maintain digital length and alignment while also promoting bone union. In our study, all patients achieved solid bone union: 12 patients using K-wire fixation and 2 patients with only finger splinting. Subgroup analysis revealed no significant difference in bone union time between the K-wire fixation group and the finger splint group. These results support our standardization of the bone graft fixation method as non-rigid K-wire fixation.
In terms of the optimal timing for bone graft placement, most recommendation indicate grafting 6–8 weeks following bone cement application.6,17,19 In the present study, the authors performed bone grafting after a mean interval of 71.50 (±23.66) days (range, 35–107 days), ensuring all infections had fully resolved, yet bone union was achieved in all cases at a mean of 46.93 (±16.08) days (range, 28–78). Also, statistical analysis revealed no significant relationship between the interval from bone cement insertion to bone grafting and the time to bone union. These findings suggest that, while it is important to adhere to the traditional interval of 6–8 weeks between stages, the timing of the second stage operation can be adjusted more flexibly once signs of infection have fully resolved. This flexibility may allow for earlier bone grafting in patients with high functional demands, highlighting the need for further research on this topic.
The authors performed cement insertion twice in three cases. Infection is a frequent complication associated with the Masquelet technique and is primarily attributed to insufficient debridement. 9 We agree with this perspective. Favorable outcomes are possible only after meticulous debridement and infection control, followed by subsequent bone grafting.
The limitations of this study should be noted. First, the sample size was small, and the analysis was retrospective in nature. Thus, further studies with multicenter, large cohorts are warranted. Additionally, two patients were unable to return to the authors’ institution for long-term follow-up. Therefore, functional outcomes were assessed using Quick DASH scores through telephone interviews and photographs provided by these patients were incorporated by comparing them with the previously measured ROM at the latest follow-up. This methodology restricted our capacity to deliver a more thorough evaluation of functional results. Nonetheless, all patients indicated no pain and no notable limitations in hand function. Various bone graft substitutes have been developed and are utilized as alternatives to autogenous bone grafting, particularly when cortical bone grafting is unnecessary or autogenous bone grafting is not feasible. Therefore, given the successful results obtained with non-rigid bone fixation and cancellous bone grafting in this study, further studies are warranted to evaluate radiological outcomes when bone graft substitutes are placed within an induced membrane and to assess whether such substitutes could replace cancellous bone grafting.
Conclusion
It is considered that antibiotic-loaded bone cement insertion followed by autogenous iliac bone grafting to be a highly reliable and reproducible intervention for subacute/chronic phalangeal OM. Even in cases with bone defects exceeding 10 mm, the combination of cancellous bone grafting and non-rigid fixation can achieve excellent outcomes without the necessity for cortico-cancellous grafts. Therefore, we advocate this approach as a treatment option for phalangeal OM.
Footnotes
Ethical considerations
This study received approval from our institutional review board at Jeonbuk National University Hospital (CUH 2025-07-018-001).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.