
Abstract
Purpose
Clinically, metastatic pathological fractures of the humeral shaft remain a challenging issue. Plate osteosynthesis and intramedullary nailing are common fixation methods; however, the optimal strategy remains debated, especially in patients with limited life expectancy where surgical goals include rapid pain relief, functional recovery, and fewer reoperations.
Methods
We retrospectively reviewed 27 patients with metastatic humeral shaft fractures treated surgically during 2009–2019. Patients were grouped by plate osteosynthesis (n = 17) and antegrade intramedullary nailing (n = 10), and operative time, intraoperative blood loss, pain relief (visual analog scale), functional outcomes (Musculoskeletal Tumor Society scoring system), postoperative survival, complications were compared.
Results
Intramedullary nailing was associated with significantly less blood loss (298 ± 61 vs 557 ± 124 mL, p < 0.001) and better MSTS score (22.1 ± 3.34 vs 17.41 ± 6.2, p < 0.05) compared with plating, whereas postoperative pain relief was comparable. Postoperative survival did not differ significantly between the two groups. Complication rates did not different significantly, although implant failure–mediated reoperation occurred only in the plate group.
Conclusions
Both fixation methods achieved pain relief and functional improvement. However, intramedullary nailing demonstrated distinct advantages, reducing surgical morbidity, minimizing reoperation and superior functional outcomes which will benefit metastatic patients with low life expectancy. Overall, these results support intramedullary nailing as a reliable first-line option for most humeral shaft pathological fractures, whereas plate fixation may be reserved for proximal or distal lesions.
Introduction
Breast, lung, prostate, and kidney carcinomas are the most common sources of metastatic bone tumors. In recent years, advances in chemotherapy, targeted therapy, and radiotherapy have extended patient life expectancy. Additionally, radiation therapy, bisphosphonates, and RANKL inhibitors slow bone destruction. Despite these treatment options, pathological fractures of the humeral shaft remain challenging for orthopedic surgeons owing to factors such as tumor origin, available adjuvant therapies, implant selection, and patient-specific considerations.1,2 Conservative treatment often leads to high nonunion rates, poor quality of life due to inadequate pain relief, and severely limited upper arm function, even in cases that are not life-threatening. 3 Surgical procedures typically involve tumor excision with plate osteosynthesis or intramedullary nailing followed bone cement augmentation. Plate osteosynthesis, the traditional method, requires wide wound exposure and longer operative time, with increased intraoperative blood loss and risk of neurovascular injury.4–6 A major concern arises when malignancy recurs at the surgical site or the implant fails, often necessitating reoperation and plate exchange.6,7 Intramedullary locking nail fixation with bone cement offers earlier functional recovery, smaller surgical wounds, and reduced intraoperative blood loss.8,9 Importantly, intramedullary nail fixation more often preserves the existing implant if malignancy occurs.6,10–12
Although several studies and meta-analyses have compared intramedullary nails and plates in traumatic humeral shaft fractures, research focusing on metastatic pathological fractures remains limited, particularly in Asian populations where primary tumor distribution differs from Western series (e.g., hepatocellular and nasopharyngeal carcinomas). Moreover, few studies have directly addressed palliative goals, such as minimizing surgical morbidity and avoiding reoperation in patients with limited life expectancy.
The present study compares the outcomes of plate osteosynthesis and intramedullary nailing in patients with metastatic humeral shaft fractures, focusing on perioperative morbidity, pain relief, functional recovery, and complications.
Materials and methods
This retrospective case-series study was approved by the Institutional Review Board of our hospital. We reviewed the medical records and radiographs of patients with pathological humeral shaft fractures treated with plate fixation or intramedullary nailing at the Tri-Service General Hospital between June 2009 and May 2019.
We included 27 patients who sustained pathological humeral shaft fractures and underwent surgery. The inclusion criteria were as follows: (i) confirmed metastatic pathological fracture of the humeral shaft, (ii) treatment with either plate osteosynthesis or antegrade intramedullary nailing, and (iii) minimum follow-up of 12 months or until death. The exclusion criteria included (i) primary bone tumors or benign lesions, (ii) fractures at the proximal humerus (surgical neck) or distal humerus (supracondylar region), (iii) multiple synchronous humeral lesions requiring combined fixation, (iv) postoperative life expectancy <3 months and (v) insufficient clinical or radiographic follow-up. Anteroposterior and lateral radiographs of the humerus were obtained for diagnostic evaluation. Patients were divided into two groups: plate osteosynthesis (group 1) and intramedullary nailing (group 2). Selection between plate osteosynthesis and intramedullary nailing was individualized by the treating surgeon according to clinical presentation.
In the plating group, a relatively large incision was made, extending beyond the fracture site. An anterolateral or posterior approach was selected based on lesion location and surgeon preference. The tumor was excised, followed by high-speed burring. The locking plate was applied across the fracture site. 13
In the nailing group, a smaller incision was made, equal to or smaller than the fracture site. Patients were positioned in the beach-chair position, and an anterolateral approach was used for all cases. Tumor excision was followed by high-speed burring and 95% alcohol adjuvant therapy.14,15 Antegrade nailing with appropriate nail size and static locking screws was applied in all patients. All intramedullary devices in this study were second-generation curved antegrade humeral nails, inserted via a greater-tuberosity (rotator-cuff footprint) entry portal and secured with standard proximal and distal interlocking screws that engaged the nail via threaded, metal-to-metal locking (no polymer bushings).
In all cases across both groups, bone cement was used to fill the bony defect. The minimum fixation comprised, for the intramedullary nailing group, two proximal and one distal locking screws; for the plate group, three proximal bicortical locking screws (or six unicortical locking screws) and three distal bicortical locking screws.
The following variables were assessed: primary tumor origin; operative time; intraoperative blood loss; implant failure; and postoperative pain relief, functional recovery, survival rate and complications. Subjective pain relief was evaluated at 1 month postoperatively using the visual analog score (VAS; 0–10). Functional recovery was evaluated at 3 months postoperatively using the Musculoskeletal Tumor Society (MSTS) Scoring System for the upper extremity.
Complications included tumor recurrence, implant failure (broken plates, screws, or nails), peri-implant fracture, surgical wound dehiscence.
Results
Clinical data
Demographic data and clinical characteristics.
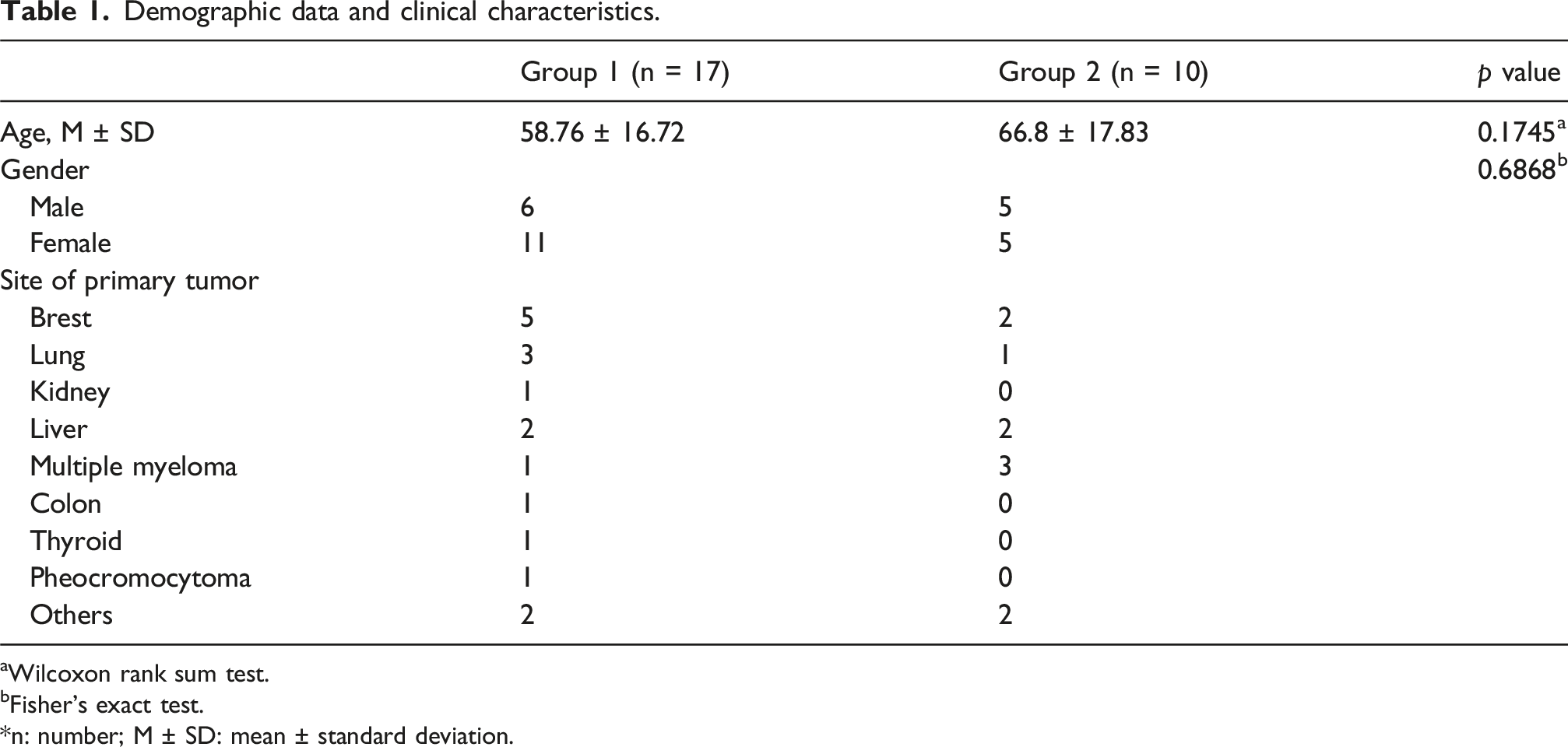
aWilcoxon rank sum test.
bFisher’s exact test.
*n: number; M ± SD: mean ± standard deviation.
Perioperative clinical parameters
Total operative time did not differ between groups, with 200.06 ± 56.30 and 192.4 ± 30.73 min recorded in group 1 and 2, respectively (p = 0.782). However, average blood loss differed significantly (p < 0.01) between group 1 (557.06 ± 124.39 mL) and group 2 (298 ± 61.43 mL).
Postoperative clinical results
Both groups showed significant improvement in VAS pain scores at 1 month after surgery (both p < 0.01, paired t test). Preoperative VAS scores did not differ between groups (group 1: 9.18 ± 0.53; group 2: 9.10 ± 0.58; p = 0.754), nor did postoperative scores (group 1: 3.06 ± 0.90; group 2: 3.00 ± 1.15; p = 1). Postoperative functional outcomes assessed at 3 months after surgery by the MSTS scoring system were significantly better in the intramedullary nailing group (group 1: 17.41 ± 6.2; group 2: 22.1 ± 3.34; p = 0.037). Kaplan-Meier estimates showed no significant difference in postoperative survival between Group 1 and Group 2 (6-months: 64.7% vs 80.0%; 1-year: 47.1% vs 40.0%; log-rank P = 0.1908; Figure 1). Kaplan-Meier survival curve.
Postoperative complications
Clinical outcomes.

*n: number; M ± SD: mean ± standard deviation; VAS: Visual Analog Scale; MSTS: Musculoskeletal Tumor Society.
aWilcoxon rank sum test.
blog-rank test.
cFisher’s exact test.
Discussion
Successful surgical treatment of humeral shaft pathological fractures is important for improving quality of life during the remaining lifespan of affected patients. Because metastatic patients generally have weaker overall condition compared with healthy individuals, major benefits are provided by shorter surgical time, less perioperative blood loss, and smaller incisions. In our study, the intramedullary nailing group exhibited advantages over the plate osteosynthesis group, including shorter operative time, significantly reduced blood loss and incision size, and better functional recovery. Smaller incisions with limited dissection reduced blood loss in the nailing group because the surgical field did not need to extend beyond the fracture region. However, in the plate group, solid fixation required at least three bicortical screws above and below the fracture, 13 necessitating a larger incision to accommodate plate and screw placement.13,16
Meta-analyses by Ma et al. 9 and Ouyang et al. 17 found no significant differences in postoperative infection, radial nerve injury, or iatrogenic fracture comminution but reported increased risk of shoulder impingement and restricted shoulder movement. In our study, no patient reported shoulder problems post-nail surgery. 18
Dai et al. 8 and Zheng et al. 19 reported no significant differences in postoperative functional outcomes or objective and subjective pain relief between nails and plates for humeral shaft fractures. In our study, both groups showed significant VAS improvement postoperatively, a key factor influencing quality of life.
Although prior studies have suggested that intramedullary nailing may increase the risk of systemic metastases,
5
given the short life expectancy of affected patients, this effect is likely minimal. In our study, one patient in the intramedullary nail group experienced tumor recurrence 5 months postoperatively. The recurrent tumor was excised with bone cementation without implant revision (Figure 2), and no further complications were noted until follow-up was lost after 1 year. Because intramedullary nails are load-sharing implants that bypass the diaphyseal lesion to proximal and distal bone, they reduce fixation failure.
6
Unless tumor involvement compromises the static locking screws, the intramedullary nail can stabilize the humeral shaft and protect a long bone segment from new fractures, even after additional surgery for disease progression or metastasis.
4
A 50-year-old male underwent tumor excision and open reduction internal fixation with intramedullary nail for pathological fracture of the humeral shaft. He received revision surgery due to tumor recurrence.
Notably, tumor recurrence after plate osteosynthesis has a high likelihood of affecting adjacent screws, causing fixation loss or instability. Plate exchange to a longer implant may be required, posing risks and severely reducing quality of life in terminal patients.1–3 In our study, one patient that underwent plate osteosynthesis suffered a broken plate 2 months after surgery, requiring revision to a longer plate; this implant subsequently failed after 4 months, necessitating conversion to intramedullary nail fixation. No further implant failure occurred until the patient’s death 2 years later, but the three revision surgeries caused substantial suffering and poor quality of life (Figure 3). A 75-year-old female underwent tumor excision and open reduction internal fixation with plate for pathological fracture of the humeral shaft. She received two revision surgeries due to implant failure.
Unlike normal traumatic humeral shaft fractures, achieving bony union is not the primary goal in metastatic fractures. Meta-analyses have indicated that plate osteosynthesis may achieve similar union rates as nails but with major shoulder complications.8,18,19 Intramedullary nails provide safer, biomechanically effective fixation against angulation and torsion while reducing blood loss, accelerating recovery, shortening hospitalization, lowering infection risk, decreasing revision rates, and potentially facilitating radiotherapy if closed reduction is used.5,12,14
In traumatic humeral shaft fractures, meta-analyses have shown comparable union rates for nails and plates, with nails carrying higher risks of shoulder impingement.8,18,19 In our metastatic cohort, no patient experienced clinically relevant shoulder dysfunction, suggesting that the palliative benefits of nails outweigh potential shoulder complications.
Our findings align with prior reports indicating that intramedullary fixation is less invasive and offers stable constructs capable of bypassing diseased bone segments. The reduction in soft-tissue dissection and intraoperative blood loss, combined with the capacity of nails to facilitate earlier postoperative rehabilitation, likely contributed to the superior MSTS scores observed in the intramedullary nailing group compared with the plate osteosynthesis group in our cohort.
Implant failure and reoperation are particularly devastating in patients with limited life expectancy, as revision surgery substantially compromises quality of life. In our series, reoperations occurred only in the plate group, including one patient requiring multiple revisions before conversion to a nail. In contrast, no nail-related reoperations were needed, highlighting the advantage of a load-sharing device in metastatic bone.
From a practical perspective, intramedullary nailing should be considered the first-line option for most mid-shaft metastatic humeral fractures. It offers shorter surgery time, reduced blood loss, and durable fixation, aligning with palliative treatment goals. Plate fixation remains useful for proximal or distal lesions where nail fixation is suboptimal, although it carries higher risks of extensive surgical exposure, blood loss, and implant failure in recurrent disease. Thus, implant selection should be individualized based on lesion location, patient condition, and surgeon expertise.
This study has several limitations. First, its retrospective, single-center design and small sample size limit generalizability and statistical power. Second, heterogeneity in tumor biology and adjuvant therapy may have influenced outcomes. Despite these limitations, our study provides meaningful data in an Asian population.
Prospective multicenter studies with larger cohorts are needed to confirm this study’s findings and incorporate validated functional outcome measures. Further research should evaluate cost-effectiveness and integration with systemic therapy to better define the role of intramedullary nailing in multidisciplinary cancer care.
Conclusion
Both plate osteosynthesis and intramedullary nailing are effective surgical options for metastatic pathological fractures of the humeral shaft, providing pain relief and functional restoration. Nevertheless, intramedullary nailing demonstrates distinct advantages, including reduced surgical morbidity and lower reoperation rates, which are particularly relevant for patients with limited life expectancy. Moreover, intramedullary fixation not only affords stable constructs capable of bypassing diseased bone but also minimizes perioperative morbidity and facilitates earlier functional recovery, thereby leading to superior functional outcomes compared with plate fixation. Our findings support intramedullary nailing as the preferred fixation method for most mid-shaft lesions, although plate fixation remains valuable for selected proximal or distal fractures where nail stability may be compromised.
Footnotes
Consent for publication
Patient consent was waived due to the observational design of this study, with approval granted by the Institutional Review Board.
Author Contributions
Conceptualization, Yao-Tung Tsai; methodology, Yao-Tung Tsai; Data analysis, Tse-Pu Huang; writing—original draft preparation, Tse-Pu Huang; writing—review and editing, Yao-Tung Tsai. All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study are contained in the article. Requests for further details may be directed to the corresponding author.
Institutional review board statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Tri-Service General Hospital (protocol code B202405173 and date of approval 2024/9/4).