
Abstract
Background
Osteochondral fracture (OCF) often occurs in patellar dislocation and has various treatment methods. The purpose of this study is to ascertain the clinical efficacy of using absorbable cartilage screws to fix OCF.
Methods
We conducted a retrospective analysis of 455 patients who underwent medial patellofemoral ligament reconstruction (MPFLR) from 2020 to 2024, with the aim of identifying patients who underwent simultaneous OCF fixation with bioabsorbable screws. The preoperative and postoperative joint functions were evaluated by ROM (range of motion), VAS (visual analogue scale) score of patellofemoral joint pain during knee deep flexion, Kujala score, Lysholm score, IKDC (international knee documentation committee) score and Tegner score. The MRI was used to evaluate the fracture healing.
Results
There were a total of 31 patients who underwent both MPFLR and OCF fixation simultaneously. The average age was 18.21 years (12.08–36 years) [16.00, 20.41]. The average follow-up time was 33.71 months (10–60 months) [27.54, 39.88]. The ROM (120.81 ± 7.30), VAS score (1.35 ± 0.49), Kujala score (87.00 ± 7.32), Lysholm score (86.32 ± 8.92), IKDC score (85.26 ± 4.49) and Tegner score (5.81 ± 0.75) at the latest follow-up were significantly improved comparing with the preoperative ROM (87.32 ± 8.83), VAS score (8.35 ± 0.55), Kujala score (56.16 ± 18.43), Lysholm score (48.61 ± 10.16), IKDC score (43.58 ± 6.00) and Tegner score (3.52 ± 0.51), the differences were statistically significant (t = −16.273, 53.048, 8.660, 15.535, −30.959, −14.088, respectively. all p < 0.001). MRI showed good healing of OCF. All patients recovered well after surgery.
Conclusion
This study confirms the satisfactory clinical outcomes of using absorbable cartilage screws to fix OCF caused by patellar dislocation.
Keywords
Introduction
Patellar dislocation is a common knee joint injury in adolescents.1–3 During dislocation and reduction, the shear between the patellar articular surface and the lateral femoral condyle usually causes OCF.4,5 It has been reported that the incidence of OCF after patellar dislocation is 5%∼76%. 6 There are various treatment options for OCF in patellar dislocation, including removal of osteochondral fragments, microfracture, internal fixation, and cartilage transplantation.7–11 However, there is still controversy over the ideal treatment method for OCF following patellar dislocation. 12
Multiple surgical procedures for internal fixation of osteochondral fragments have been proposed over the past years, including fibrin glue, sutures, metal screws, and bioabsorbable screws,13–16 but there is currently no consensus on the best method for OCF fixation. Non-surgical treatment is generally recommended for patients with first-time patellar dislocation, while patients with recurrent patellar dislocation typically require patellar stabilization surgery, such as a MPFLR.17–19 There seems to be a consensus that when patellar dislocation leads to OCF, surgeons should address OCF simultaneously while treating patellofemoral instability, with the aim of reducing recurrent patellofemoral instability and protecting articular cartilage.20,21
The clinical results of using bioabsorbable screws to fix OCF following patellar dislocation are still unclear. The aim of this study is to assess the efficacy of using absorbable cartilage screws to fix OCF.
Methods
Study cohort
After approval by the Institutional Review Board, we conducted a retrospective analysis of 455 patients who underwent MPFLR from 2020 to 2024. The inclusion criteria for this study include diagnosis of patellar dislocation and confirmation of OCF present in the patella or femoral condyle through MRI and arthroscopy. The exclusion criteria include the presence of OCF in other areas and a history of knee joint surgery.
Surgical technique
Firstly, it is essential to identify the location of the OCF fragment. After removing it from the knee, we cleaned the fibrous tissue on the fragment. Then, the frayed edges of the parent bone were trimmed. If the fracture site shows a large area of exposed chondral bone, a Kirschner wire was used to drill an appropriate amount of holes. Finally, the OCF fragment was placed into the parent bed and secured with absorbable cartilage screws (Figure 1). OCF fragment was fixed with bioabsorbable poly (L-lactide-co-glycolide) (PLGA) fixation screws (1.5 × 20 mm, 1.5 × 25 mm, 2.0 × 20 mm, 2.0 × 25 mm, Bioretec Ltd, Finland). (a) A lateral femoral condyle defect. (b, c) Size of OCF fragment (2.6 × 4.5 cm). (d) OCF fixation with seven bioabsorbable screws.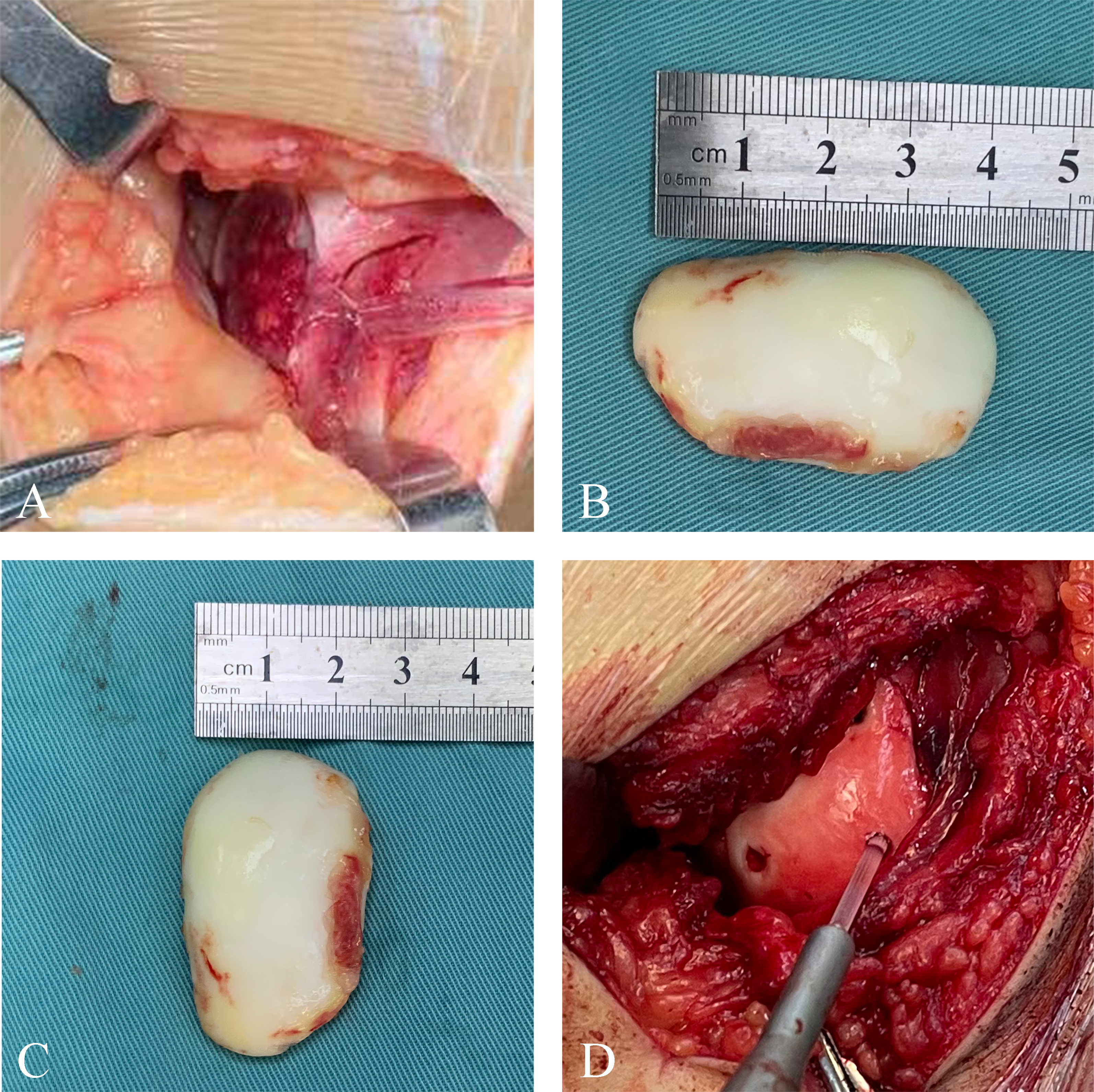
MPFLR surgical procedure was performed in patients with patellar dislocation. We obtained and prepared half of the autologous peroneal longus tendon as the graft tendon. Firstly, two suture anchors were inserting into the midpoint and upper middle one-third section of the medial edge of the patella. Then, we fastened the middle part of the graft tendon to the anchors. Afterwards, we measured the diameter of the graft tendon and used the corresponding trephine to drill along the femoral guide pin into the femoral tunnel. With the knee joint flexed at 30°, the graft tendon was anchored into the femoral tunnel with an interference screw. Finally, we evaluated the patellar stability by flexing and extending the knee joint.
Postoperative rehabilitation
After surgery, patients underwent early rehabilitation exercises, including straight-leg raising and ankle pumps. Patients should actively flex the knee joint and begin partial weight-bearing exercise at 3 weeks after surgery. Subsequently, knee joint flexion was further enhanced and increased by 30° per week, and was expected to reach 90° at 6 weeks after surgery.
Statistical analysis
Data were obtained and analyzed retrospectively. Statistical analysis was performed using IBM SPSS Statistics for Windows (version 24, IBM Corp., Armonk, NY). Continuous variables were reported as means and standard deviations, and discrete variables were reported as frequencies and percentages. Comparing quantitative variables by the independent t test or the Mann-Whitney U test. A p < 0.05 is considered statistically significant.
Results
Demographic data and descriptive statistics.

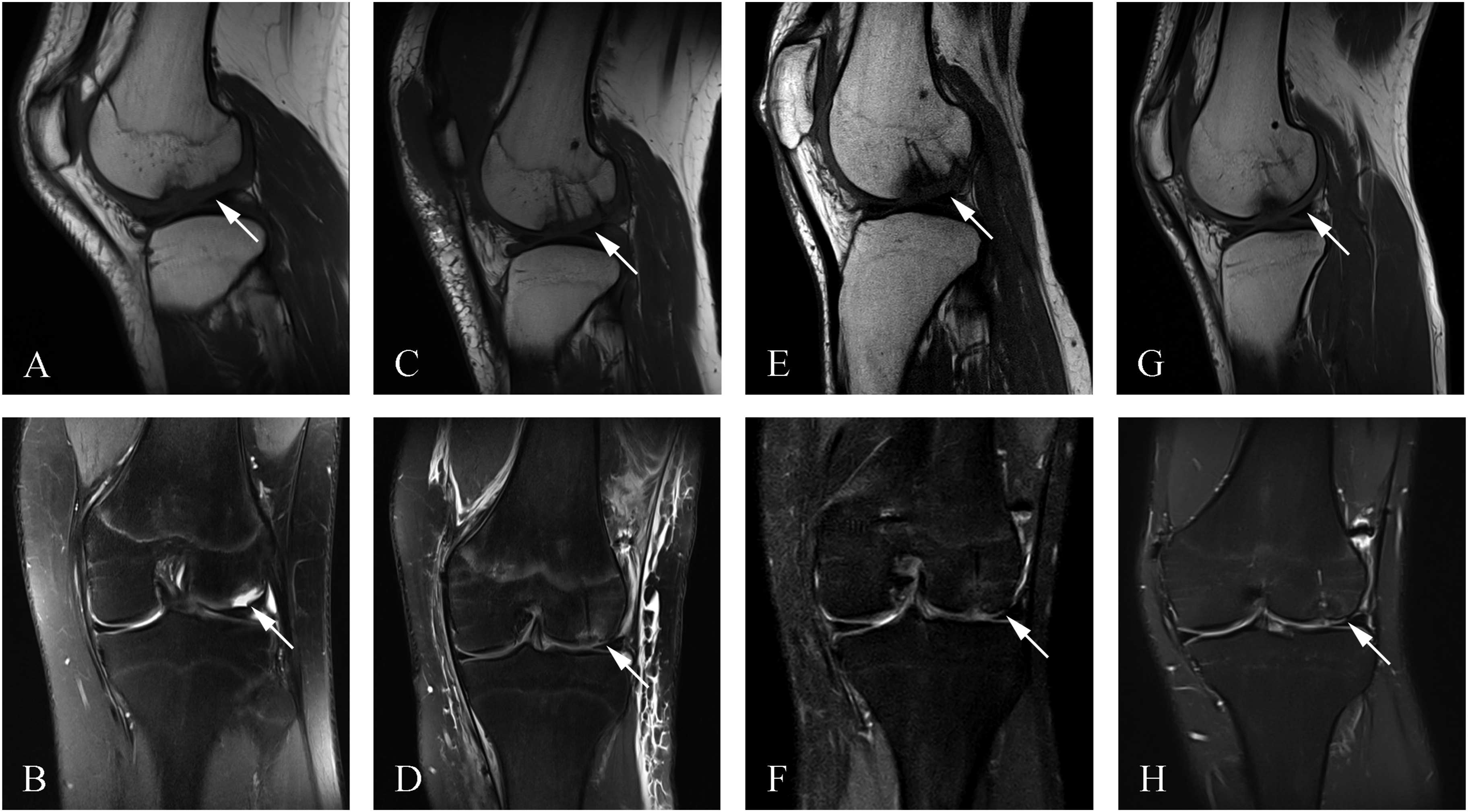
Preoperative MRI showed that the lateral femoral condyle of most patients with patellar dislocation exhibited bone marrow edema. Postoperative follow-up MRI indicated that all 31 knee OCF fragments were well integrated with the parent bone (Figures 2 and 3). (a, b) Preoperative MRI images of an OCF of the lateral femoral condyle. (c, d) Postoperative MRI images of OCF fixed with bioabsorbable screws. (e, f) 1 month postoperative MRI images. (arrows: preoperative and postoperative OCF). (a, b) Preoperative MRI images of an OCF of the lateral femoral condyle. (c, d) Postoperative MRI images of OCF fixed with bioabsorbable screws. (e, f) 6 months postoperative MRI images. (g, h) 16 months postoperative MRI images. (arrows: preoperative and postoperative OCF).
Comparison of preoperative and postoperative knee joint function scores.

Abbreviations: ROM: range of motion; VAS: visual analogue scale; IKDC: international knee documentation committee.
Discussion
This study found that MPFLR and simultaneous OCF fixation with absorbable cartilage screws can achieve satisfactory clinical results for OCF caused by patellar dislocation. The results of MRI examination showed that all OCF fragments successfully integrated with the parent bone without serious complications such as recurrent instability, infection and stiffness.
OCF caused by Patellar dislocation is the main indication for surgical intervention. 22 There are many materials available for fixing OCF fragment including metal needles and headless screws, but the disadvantage of these metal implants is that they need to be removed after the fragment healing. 23 In addition, the microfracture of the lesion area, as well as autologous or allogeneic osteochondral implantation, have been applied to repair such lesions.24–26 Although some studies have reported good short-term effects, more studies with longer follow-up are needed to adequately assess these techniques.27,28
In recent years, the development of biodegradable fixation devices has brought new choices to the field of OCF fixation. The main advantage is that the implanted devices don’t need to be removed. However, as described in the literature, these new devices may lead to some complications, such as synovitis or foreign body reaction.15–17
Previous studies have shown that various fixation methods can achieve satisfactory OCF healing. MPFLR and simultaneous OCF fixation with bioabsorbable screws are reliable methods for treating OCF caused by patellar dislocation. Li et al. 29 demonstrated that using absorbable sutures to fix OCF caused by patellar dislocation can achieve satisfactory clinical results. A recent study showed that during a follow-up period of 2.6 years, 95% of patients who underwent MPFLR and simultaneous OCF fixation with bioabsorbable nails showed patellar stability and did not require cartilage repair surgery. 30 Similar to previous literature reports, in our study, all OCF fragments of the knees were well integrated with the parent bone, indicating that bioabsorbable screws are a feasible method for treating OCF caused by patellar dislocation.
However, this study has several limitations. First, this is a single-center study with a small sample size, which may lead to certain data bias. Furthermore, the follow-up time is relatively short. The low incidence of complications that differs from the current literature may be confounded by patients with limited follow-up. Previous study found that the incidence of postoperative complications such as OCF fixation failure, recurrent patellar dislocation, and osteoarthritis increases with increasing follow-up time. 31 Finally, this is a retrospective study with no control group, which may cause the results to be underpowered. The results of this study should be confirmed by a longer term follow-up and a comparative control study with different fixation methods in the future. Nonetheless, this study suggested that the clinical results of MPFLR and simultaneous using absorbable cartilage screws to fix OCF are promising. For patients with OCF caused by patellar dislocation, surgeons should consider this method.
Conclusion
In this study, during an average follow-up of 33.71 months, all knees that underwent MPFLR and simultaneously used absorbable cartilage screws to fix OCF showed patellar stability and good integration of OCF fragments with the parent bone. Therefore, using absorbable cartilage screws to fix OCF is a feasible method for treating OCF caused by patellar dislocation.
Footnotes
Ethical approval
This study was approved by the Research Ethics Committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital; Grant No: CY2022-QN-B06, CY2022-MS-A19, CY2021-MS-A07, Cuiying Student Research Cultivation Program of Lanzhou University Second Hospital; CYXZPT2025-39, 10.13039/501100004775; Natural Science Foundation of Gansu Province; 22JR5RA943, 22JR5RA956, 23JRRA1500, 24YFFA043, 24JRRA341, 10.13039/501100001809; National Natural Science Foundation of China; 82060405, 82360436, Cuiying Scientific Training Program for Undergraduates of The Second Hospital & Clinical Medical School, Lanzhou University; CYXZ2024-36.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.