
Abstract
Background
To investigate the clinical utility of shear wave elastography (SWE) in the diagnosis and prognostic evaluation of acute anterior talofibular ligament (ATFL) injuries.
Methods
This prospective cohort study enrolled 46 patients with unilateral acute ATFL injuries and 32 age and gender-matched healthy volunteers. All patients underwent B-mode ultrasonography and SWE within 48 h post-injury and at 3 month post-rehabilitation. Quantitative assessments included ATFL thickness, Young’s modulus, shear wave velocity (SWV), vascular perfusion, and echotextural characteristics.
Results
During the acute phase (≤48 h), injured ATFLs exhibited significantly greater thickness compared to contralateral and healthy control ligaments (3.54 ± 0.68 mm vs 2.15 ± 0.22 mm and 2.31 ± 0.16 mm, respectively; p < .05), alongside markedly reduced Young’s modulus and SWV. Biomechanical parameters were consistently elevated in plantarflexion-inversion versus neutral positioning. At 3-month follow-up, elastic parameters normalized substantially, with restoration of ligamentous thickness and vascular perfusion eliminating intergroup differences. The dynamic trajectory of SWE metrics paralleled structural recovery patterns.
Conclusion
SWE quantitatively evaluates biomechanical integrity and recovery progression in acute ATFL injuries. Combined with B-mode ultrasonography, SWE provides a robust imaging framework for diagnosis, longitudinal monitoring, and prognostic stratification, demonstrating significant clinical value in musculoskeletal trauma management.
Keywords
Introduction
Acute ankle sprain represents one of the most prevalent musculoskeletal injuries encountered in sports medicine, demonstrating exceptionally high incidence among adolescents, young adults, and athletic populations. 1 The anterior talofibular ligament (ATFL), as the most frequently compromised structure within the lateral ankle ligamentous complex, accounts for over 70% of all ankle sprain cases. 2 Failure to achieve timely and accurate diagnosis coupled with appropriate intervention in acute ATFL injuries substantially predisposes patients to chronic ankle instability. This sequela profoundly impairs activities of daily living and athletic performance while elevating risks of recurrent injury and premature joint degeneration. 3 Consequently, the establishment of methodologies enabling early and precise assessment of ATFL injury severity and healing progression bears critical significance for optimizing clinical decision-making and enhancing long-term functional outcomes.
Current diagnostic paradigms for ligamentous injuries rely principally upon clinical examination, advanced imaging modalities, 4 and surgical exploration when indicated. Conventional imaging techniques encompass radiography, computed tomography (CT), magnetic resonance imaging (MRI), and ultrasonography.5–7 However, each modality exhibits inherent limitations. Radiography and CT provide suboptimal characterization of ligamentous architecture and functional integrity. Although MRI affords superior soft-tissue resolution for structural delineation, it remains incapable of evaluating biomechanical properties and dynamic functional alterations. Traditional ultrasonography, while enabling real-time assessment, demonstrates substantial operator-dependent variability that compromises objective quantification of injury extent and recovery status. The evolving landscape of biomedical imaging has witnessed revolutionary advances with the integration of shear wave elastography (SWE), representing a transformative breakthrough in sonographic diagnostics. 8 SWE constitutes a novel functional ultrasound technique that quantifies tissue elastic modulus through measurement of shear wave propagation velocity following acoustic radiation force excitation. This noninvasive methodology provides unique insights into tissue stiffness and biomechanical characteristics, having established diagnostic utility across hepatic, breast, tendinous, and some ligamentous pathologies.9–12 Preliminary investigations have explored SWE’s potential in evaluating tendon and ligament injuries, suggesting its capacity for early microstructural damage detection and longitudinal monitoring of tissue repair and remodeling processes [13]. Nevertheless, rigorous evidence regarding SWE’s systematic application for diagnosis, therapeutic monitoring, and prognostic assessment in acute ATFL injuries remains notably deficient. Furthermore, the correlation between SWE-derived parameters and conventional B-mode ultrasonographic metrics warrants comprehensive elucidation.
Building upon this foundation, the present study employs a prospective cohort design to systematically evaluate structural and biomechanical parameters via integrated B-mode ultrasonography and SWE. This dual-modality approach will be implemented during both the acute injury phase and at 3-month post-rehabilitation intervals in patients with unilateral acute ATFL injuries. Our study aims to comprehensively analyze SWE’s clinical value for quantitative diagnosis, dynamic monitoring, and therapeutic efficacy assessment in acute ATFL pathology. The anticipated outcomes will provide scientific rationale for early diagnosis, lesion stratification, objective healing quality evaluation, and evidence-based rehabilitation protocols, thereby advancing standardized implementation and clinical adoption of SWE in sports injury imaging.
Materials and methods
Study design
A prospective cohort study was conducted involving 46 patients with unilateral ATFL injuries (injury group: 25 males, 21 females) admitted to our hospital between June 2022 and October 2023. The contralateral uninjured ankles of these patients served as the ligament-injury control group. Additionally, 32 gender- and age-matched healthy volunteers (healthy control group: 15 males, 17 females) were enrolled, yielding a total of 64 ankles analyzed. All procedures strictly adhered to the principles of the Declaration of Helsinki and received formal approval from the Ethics Committee of our hospital. Written informed consent was obtained from all participants.
For the healthy control group, the inclusion criteria comprised: (1) age ≥18 years; (2) absence of prior ankle trauma; and (3) preserved ankle range of motion with documented mechanical stability. Exclusion criteria were defined as: (1) history of ankle surgery; (2) chronic ankle overuse injuries; (3) acute/chronic inflammatory arthropathies; (4) chronic medication use with potential musculoskeletal effects; (5) systemic comorbidities including diabetes mellitus, gout, or malignancy; and (6) pregnancy or lactation.
For the ATFL injury group: the inclusion criteria required: (1) age ≥18 years; (2) closed unilateral ankle injury; (3) ultrasonographic examination performed within 48 h post-injury; and (4) MRI-confirmed ATFL pathology. Exclusion criteria encompassed: (1) complete ATFL rupture; (2) previous ankle trauma; (3) prior ankle surgery; (4) chronic medication use; (5) pre-existing ligamentous degeneration or osteoarthritis; (6) systemic comorbidities as above; and (7) pregnancy or lactation.
Ankle ultrasonography
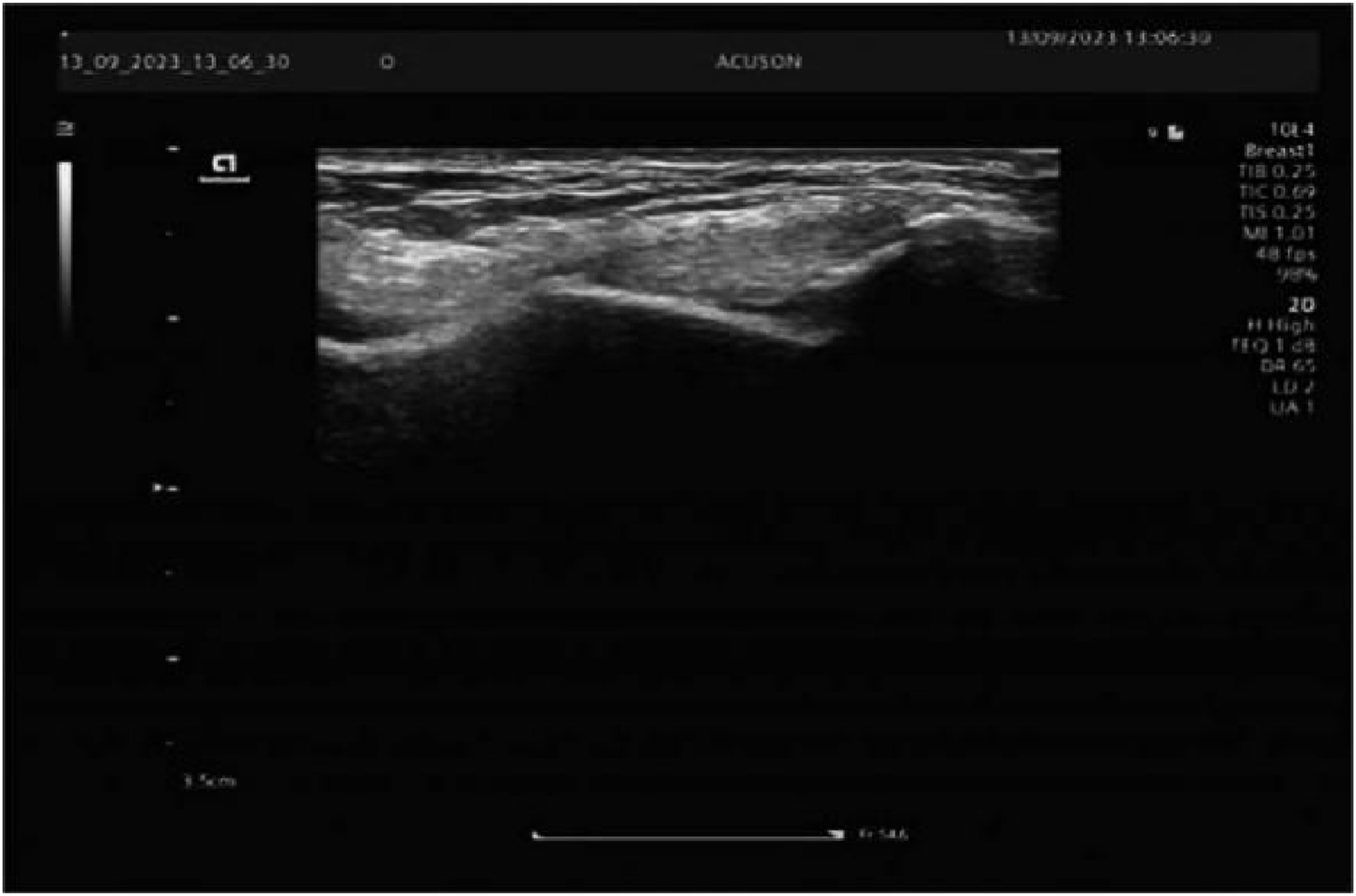
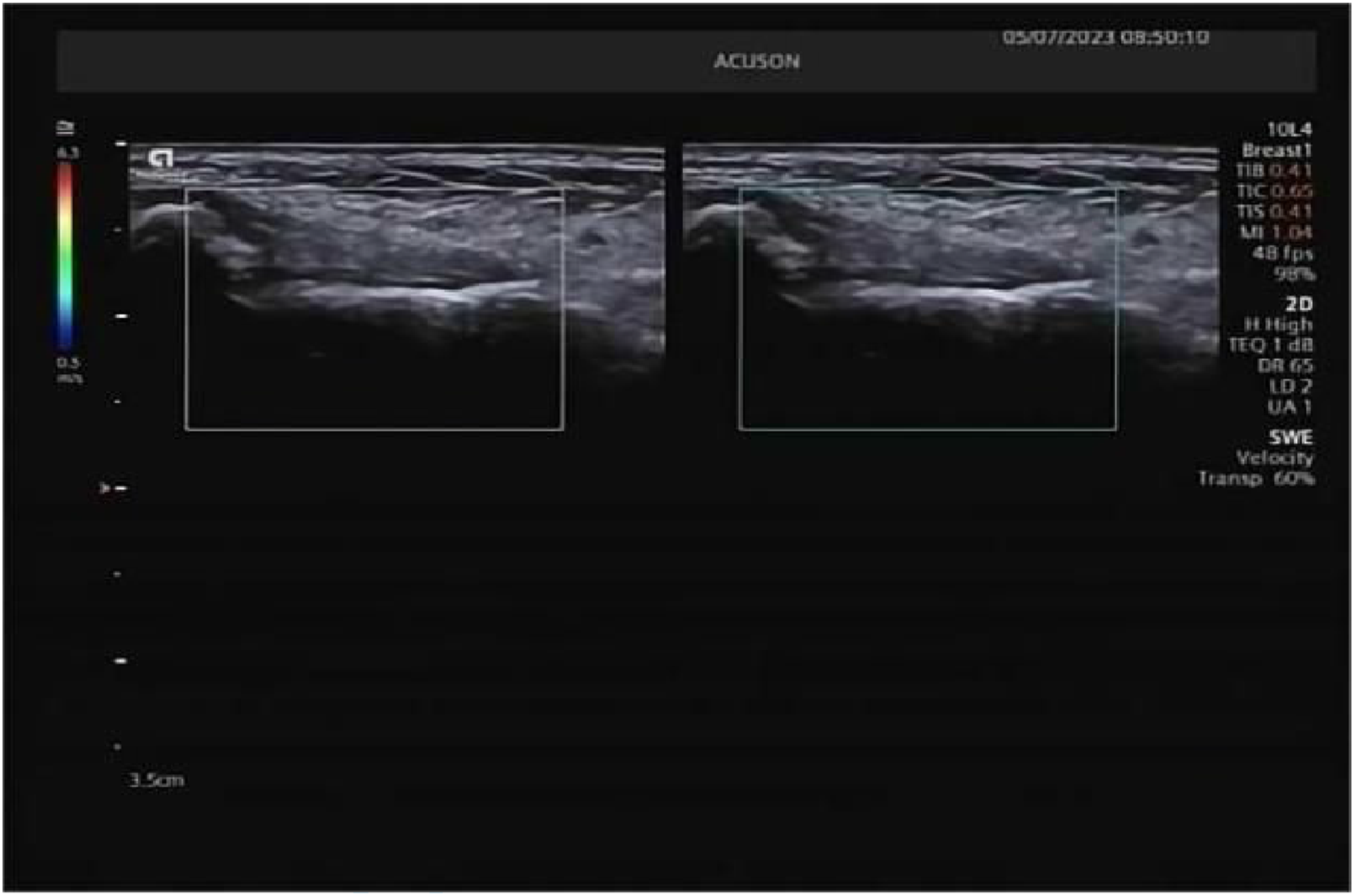
(1) All ultrasonographic examinations were conducted in a temperature-controlled environment (20 °C–25 °C). Participants were positioned seated with the foot resting naturally on the examination table in neutral alignment, ensuring full exposure of the lateral ankle complex. For plantarflexion-inversion positioning, the foot was internally rotated 15–20° while maintaining seated posture to optimize lateral ankle visualization. (2) High-frequency ultrasonography was systematically performed using continuous scanning along the osseous landmarks of the ATFL to delineate internal ligamentous architecture. Bilateral ATFL evaluation included optimization of B-mode parameters [gain, time-gain compensation (TGC), focal zones, depth] with assessment of echotexture, continuity, thickness, vascularity, and peri-ligamentous effusion/hematoma in both neutral and plantarflexion-inversion positions for injury and healthy control groups (Figures 1–5). (3) SWE acquisition was initiated following stabilization of the transducer with minimal preload (avoiding tissue compression). The maximum mid-substance sagittal plane was identified for continuous SWE duplex imaging. Quantitative measurements were obtained only when homogeneous color-coded elasticity mapping demonstrated complete filling without artifacts. Regions of interest (ROIs) were positioned at areas of maximal architectural disruption in injured ligaments, with corresponding sampling in contralateral and healthy ATFLs. Shear wave velocity (SWV) and Young’s modulus (kPa) values were triplicated and averaged (Figures 2–6). (4) All examinations utilized a Siemens ACUSON Redwood color Doppler system (Siemens Healthineers, Erlangen, Germany) equipped with a 10L-4 linear array transducer (frequency range: 2.9–9.9 MHz). A single musculoskeletal radiologist with specialized musculoskeletal sonography training and >5 years’ experience performed all scanning, image acquisition, quantitative measurements, and data recording to ensure procedural consistency. Normal anterior talofibular ligament. Elasticity of the normal anterior talofibular ligament. Partial rupture of the anterior talofibular ligament (within 48 h of injury). Contusion of the anterior talofibular ligament (within 48 h of injury). Anterior talofibular ligament (re-examination after 3 months). Elasticity of the anterior talofibular ligament (re-examination after 3 months).




Quality control
A standardized imaging protocol was maintained throughout the study utilizing a single color Doppler ultrasound system for all participants, with strict adherence to consistent positioning techniques across examinations. To minimize inter-operator variability, both data acquisition and processing were exclusively performed by the same certified sonographer. All datasets underwent blinded assessment by three independent reviewers with specialized expertise in musculoskeletal ultrasonography, each possessing over 10 years of diagnostic experience, to ensure methodological rigor and interpretive consistency.
Therapeutic management of ATFL injuries
All enrolled patients received standardized foundational treatment according to the RICE principle (Rest, Ice, Compression, Elevation) for acute ankle sprains. This protocol included cryotherapy application within 24 h post-injury, strict immobilization of the affected ankle, enforced rest periods, and sustained limb elevation. Oral analgesics were administered contingent upon individual pain tolerance thresholds. Consistent external immobilization was implemented across the cohort, comprising either plaster casting or functional bracing, and the immobilization period was approximately 2 weeks. After this short phase for pain and swelling control, early mobilization was encouraged. Patients began gentle range-of-motion exercises and partial weight-bearing as soon as tolerated (generally after the first 1–2 weeks). A functional brace was used in many cases to allow controlled movement while protecting the ligament, ensuring that patients were not kept in complete immobilization longer than necessary. A structured 3-month follow-up regimen was systematically conducted for all participants to monitor recovery progression and therapeutic outcomes.
Statistical analysis
All statistical analyses were performed utilizing SPSS Statistics version 26.0. After normality assessment, normally distributed continuous data were expressed as mean ± standard deviation (
Results
Comparative analysis of baseline characteristics
Comparison of baseline characteristics [

Quantitative analysis of ATFL thickness dynamics
Comparison of ATFL thickness (

Note. A denotes significant difference versus healthy controls (p < 0.05); b denotes significant difference versus contralateral uninjured ligaments (p < 0.05).
Comparative biomechanical analysis of ATFL across positions and time points
Biomechanical parameters of ATFL across positions and time points [

Comparative biomechanical analysis of injure group across time points
During the acute injury phase (≤48 h), the injured ATFLs demonstrated marked reductions in biomechanical parameters relative to contralateral controls. In neutral position, Young’s modulus (18.78 ± 2.35 kPa) and SWV [2.50 (2.40, 2.60) m/s] were significantly diminished compared to contralateral uninjured ligaments (Young’s modulus 28.16 ± 1.35 kPa; SWV 3.10 (3.00, 3.10) m/s] with statistical significance (p < .001 for both). Similarly, under plantarflexion-inversion loading, injured ligaments exhibited substantially lower Young’s modulus [61.15 (55.95, 77.43) kPa] and SWV [4.55 (4.30, 5.10) m/s] versus contralateral values [Young’s modulus 115.25 (112.08, 119.58) kPa; SWV 6.20 (6.10, 6.30) m/s; p < .001 for all comparisons).
Biomechanical parameters of injure group across time points [

Longitudinal biomechanical restoration in injured ATFLs
In neutral position during the acute phase (≤48 h post-injury), the injured ATFLs exhibited significantly reduced Young’s modulus [8.60 (17.58, 20.63) kPa] and SWV [2.50, (2.40, 2.60) m/s] compared to both contralateral uninjured ligaments [Young’s modulus 28.30 (27.53, 28.93) kPa; SWV 3.10 m/s] and healthy controls [Young’s modulus 28.60 (27.83, 28.98) kPa; SWV 3.10 m/s; all p < .001). Following 3-month rehabilitation, injured ATFLs achieved Young’s modulus of 27.90 (26.28, 29.20) kPa and SWV of 3.10 (2.98, 3.10) m/s, demonstrating statistical parity with both control groups (all p > .05).
Longitudinal biomechanical restoration in injured ATFLs [

Note. A, significant difference versus healthy controls (p < .05); b, significant difference versus contralateral uninjured group (p < .05).
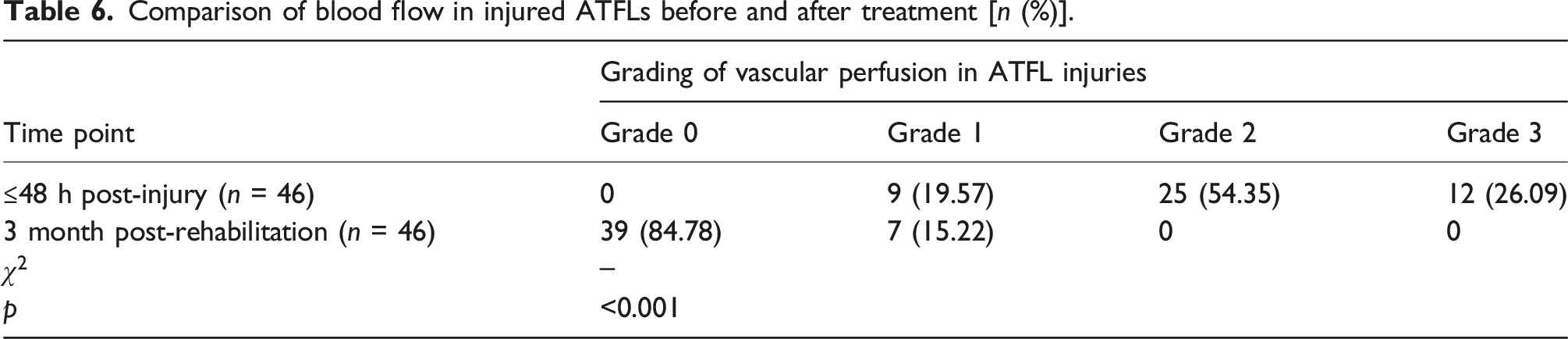
Blood flow analysis in injured ATFLs across time points
Comparison of blood flow in injured ATFLs before and after treatment [n (%)].
Longitudinal B-mode ultrasonographic evolution in injured ATFLs
Comparison of B-mode ultrasonographic data in injured ATFLs before and after treatment [n (%)].

Discussion
The evolving landscape of musculoskeletal imaging has witnessed the progressive integration of SWE as a quantitative, noninvasive ultrasonographic technique for biomechanical assessment of soft tissue structures. Substantial evidence corroborates the heightened sensitivity and reliability of SWE in detecting elasticity alterations associated with soft tissue injuries and rehabilitation processes in tendons and ligaments.13,14 Within the domain of lateral ankle ligament pathology, particularly ATFL injuries, investigations by Gimber et al. 15 and Peng et al. 16 demonstrated significantly elevated Young’s modulus and SWV in intact ATFL compared to injured states, with the most pronounced reductions in elastic parameters observed during acute injury phases. Diverging from these cross-sectional approaches, our longitudinal investigation systematically delineated the dynamic trajectory of elastic parameter evolution in ATFL from acute injury through 3-month rehabilitation. Notably, Young’s modulus and SWV in injured ATFL exhibited substantial diminution within 48 h post-injury, followed by progressive restoration to near-baseline levels approximating healthy controls at the 3-month interval. This temporal pattern not only reinforces SWE’s unique value for quantitative early injury assessment but also expands its clinical utility for monitoring rehabilitation dynamics.
Furthermore, this investigation innovatively integrated patient-matched contralateral controls with healthy control cohorts, enabling precise delineation of elasticity transition trajectories across the entire injury-repair-remodeling continuum of the ATFL. This methodological approach effectively addresses limitations inherent in prior studies that lacked longitudinal monitoring and adequate control groups. Conventional B-mode ultrasonography identified characteristic morphological derangements, such as ligamentous thickening, heterogeneous echotexture, and architectural discontinuity, establishing structural correlates for injury diagnosis. The integration of SWE complemented these findings by quantifying functional impairment severity, thereby enhancing diagnostic objectivity and grading precision.17,18 Contemporary relevant analyses corroborate our results, affirming that combined B-mode/SWE assessment significantly augments comprehensive diagnostic capability for ankle ligament injuries. 19 Consequently, this study provides scientifically rigorous and multidimensional evidence-based substantiation for clinical decision-making in both diagnostic and rehabilitative domains. Systematically evaluating the clinical utility of SWE in acute ATFL trauma, this prospective investigation synergized conventional ultrasonography with elastographic assessment to analyze structural and biomechanical evolution from acute injury through 3-month rehabilitation. Results demonstrate SWE’s capacity to quantitatively characterize ligamentous elasticity dynamics and longitudinally monitor restorative processes, thereby furnishing robust support for clinical diagnosis and prognostic stratification.
Pathophysiologically, SWE-derived parameters reflect tissue elasticity through shear wave propagation velocity measurements. Acute ATFL injury induces collagen fiber disruption, inflammatory edema, vascular hyperemia, and extracellular matrix degradation, collectively increasing tissue hydration and diminishing structural integrity. These alterations manifest as reduced SWV and Young’s modulus, findings congruent with our acute-phase observations. Color Doppler hypervascularity further corroborates regional inflammation and hyperemia.18,20 During subsequent healing, inflammatory resolution, fibroblast proliferation, and collagen realignment drive progressive restoration of biomechanical properties, evidenced by normalized SWE parameters. Crucially, our data revealed consistently higher elasticity values in plantarflexion-inversion versus neutral positioning, irrespective of injury status, highlighting ligamentous biomechanical adaptation under tensile stress. This load-dependent responsiveness underscores SWE’s capacity to dynamically evaluate functional states, establishing a foundation for quantifying biomechanical behaviors across physiological and pathological conditions.
Extant literature substantiates these mechanisms. Gao et al. 21 and Arda et al. 22 established SWE parameter dependency on collagen integrity and fiber alignment. Shinohara et al. 23 confirmed real-time load responsiveness through muscle contraction experiments, aligning with our positional elasticity variations. Similarly, Lacourpaille et al. 24 and Kantarci et al. 25 validated SWE’s predictive capacity for tissue stiffness in muscular and neural contexts. Collectively, SWE elasticity metrics represent integrative biomarkers reflecting synergistic biological processes, such as acute inflammation, fibrotic repair, and physiological load adaptation, offering novel perspectives for precision assessment of ligamentous recovery.
Our study validates the clinical efficacy of combined B-mode/SWE evaluation in acute ATFL injury management. While B-mode ultrasonography provides structural diagnosis, SWE addresses functional quantification limitations, significantly enhancing injury grading accuracy and early detection sensitivity. During rehabilitation surveillance, SWE delivers dynamic, quantitative indices of tissue remodeling, facilitating personalized rehabilitation protocol adjustments and therapeutic optimization. Moreover, multi-positional SWE assessment identifies latent functional impairments, offering objective criteria for athletic populations and high-risk individuals during return-to-activity decision-making.
Notwithstanding these contributions, several limitations warrant consideration. Our cohort focused on acute isolated ATFL injuries, thus extrapolation to chronic or complex ligamentous pathology requires caution. SWE measurements exhibit operator- and equipment-dependent variability, necessitating standardized acquisition protocols. Acute pain/swelling impeded comprehensive positional assessments in select patients, potentially limiting data completeness. Future multi-center studies with larger cohorts and standardized methodologies are essential to corroborate our findings.
Conclusion
This prospective investigation demonstrates that SWE combined with B-mode ultrasonography effectively quantifies elasticity alterations in acute anterior talofibular ligament injuries and dynamically monitors rehabilitation progress. The synergistic application of these modalities not only elevates diagnostic accuracy but also provides a robust foundation for evidence-based rehabilitation planning and personalized therapeutic strategies. SWE emerges as a clinically valuable adjunctive tool for comprehensive management of ankle ligament pathology, with significant potential to advance precision medicine paradigms in sports traumatology and orthopedic practice.
Footnotes
Author contributions
Lin Yang and Xue Xu: research design; data analysis and writing of the manuscript. Lin Yang and Jing Liu: clinical work, manuscript review, and project administration. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
All procedures strictly adhered to the principles of the Declaration of Helsinki and received formal approval from the Ethics Committee of Santai People’s Hospital (Approval No. 2023001).
Consent to participate
Written informed consent was obtained from all participants.