
Abstract
Objective
This study aims to identify and quantify the high-risk factors for deep vein thrombosis (DVT) and pulmonary embolism (PE) in elderly patients undergoing total knee replacement (TKA).
Methods
621 patients who underwent TKA were divided into DVT/PE positive group (N = 52) and a negative group (N = 569).
Result
Statistically significant differences were observed in the following factors: Caprini score (χ2 = 11.385, p < .001), prevalence of chronic obstructive pulmonary disease (COPD) (χ2 = 4.502, p = .034), history of heart failure (χ2 = 4.326, p = .012), duration of surgery (t = 3.723, p = .002), and early postoperative activity (χ2 = 4.014, p = .045). The incidence of DVT/PE was significantly higher in the very high-risk group compared to the high-risk group (9.89% vs 4.84%, χ2 = 2.080, p = .032). Multivariate logistic regression analysis identified the Caprini score as an extremely high-risk factor (adjusted OR = 2.87, 95% CI: 1.53-5.39, p = .001), alongside COPD (OR = 1.94, 95% CI: 1.08-3.48, p = .026), history of heart failure (OR = 1.68, 95% CI: 1.01-2.78, p = .048), and surgical duration exceeding 2 hours (OR = 1.35, 95% CI: 1.08-1.68, p = .008) as independent risk factors. The model, developed using multi-factor regression variables, demonstrates strong predictive performance for the occurrence of DVT/PE, with an area under the receiver operating characteristic curve of 0.842 (95%CI: 0.791-0.894).
Conclusion
In elderly patients undergoing TKA, even with standard anticoagulation prophylaxis, a high Caprini risk score, COPD, a history of heart failure, and prolonged operative time remain independent risk factors for DVT. Early postoperative mobilization has been shown to have a protective effect.
Introduction
Knee osteoarthritis in the elderly is a chronic disease primarily resulting in degenerative changes of articular cartilage. This disease has a notably high incidence rate among the elderly population. Statistics indicate that the prevalence of knee osteoarthritis in individuals over the age of 65 is approximately 10–15%, with a slightly higher prevalence observed in women compared to men. 1 Among people over 80 years old, this proportion is even as high as 40%. 2 As the global population ages, it is expected that the number of patients with osteoarthritis will increase by nearly half by 2040. 3 In advanced stages of knee osteoarthritis, patients may experience severe cartilage deterioration, osteophyte formation, joint space narrowing, and significant joint dysfunction. These changes can lead to debilitating symptoms, such as severe pain, stiffness in the lower limbs, and a substantial reduction in mobility. In such severe cases, surgical intervention, such as total knee replacement (TKA), is usually necessary to alleviate symptoms and enhance the patients’ quality of life.
TKA is the gold standard surgical method for the treatment of advanced knee osteoarthritis in the elderly. TKA provides pain relief and functional improvement in 90–95% of patients. 4 Postoperative outcomes often include a significant enhancement in quality of life and an improvement in the ability to perform daily activities, contributing to the restoration of normal walking ability and increased social participation. Furthermore, TKA has been demonstrated to be cost-effective, particularly for patients with severe osteoarthritis. 5 Although TKA is highly effective in improving patients’ quality of life, it is still associated with significant risks of postoperative venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE). 6 These complications can lead to increased morbidity, mortality, and medical costs. Consequently, while acknowledging the therapeutic benefits of TKA, it is essential to also address and mitigate the potential risks of complications.
The Caprini risk assessment model widely utilized in clinical practice to assess the risk of venous thromboembolism (VTE). This model categorizes patients’ VTE risk into four levels: low, medium, high, and very high, based on factors such as age, BMI, medical history, and type of surgery. 7 However, for elderly patients undergoing total knee replacement (TKA), most are classified as either high-risk or very high-risk due to their age, the nature of the surgery, and common comorbidities, which diminishes the discriminative power of the Caprini score in this population. Existing guidelines recommend routine anticoagulation therapy for these high-risk patients. 8 Despite prophylactic anticoagulation, the incidence of VTE remains relatively high among elderly TKA patients, with reported rates varying widely from 1.5% to 10%. This variability may be attributed to differences in study populations, diagnostic criteria, and follow-up durations. This discrepancy suggests that there may be specific risk factors in elderly TKA patients that are not fully captured by the Caprini score.
Identifying additional risk factors can help to better differentiate extremely high-risk individuals from those in high-risk categories, thereby enabling more precise risk stratification. This is crucial for optimizing VTE prevention strategies in elderly patients undergoing TKA. While previous studies have examined potential predictive factors such as advanced age, obesity, and a history of VTE, 9 the relative significance of these factors in elderly TKA patients receiving routine thromboprophylaxis remains unclear. Furthermore, the impact of factors related to the surgical process, such as duration of surgery, anesthesia methods, and early postoperative activity, also requires further investigation in this specific population.
By analyzing multivariate logistic regression, this study aims to identify and quantify factors associated with postoperative DVT/PE among elderly patients undergoing TKA. By analyzing a large multicenter cohort of patients receiving standard thromboprophylaxis, we sought to elucidate the most significant predictors of VTE events in this high-risk population. The goal is to develop more accurate risk assessment tools and personalized prevention strategies for VTE in elderly TKA patients.
Materials and methods
Study design
This study adopted a multicenter, retrospective cohort study design. Data were collected from patients who underwent TKA at five tertiary hospitals between January 1, 2020 and December 31, 2023. Inclusion criteria included: (1) age ≥ 65 years; (2) primary unilateral or bilateral TKA for knee osteoarthritis; (3) preoperative Caprini score ≥ 3 points. Exclusion criteria included: (1) preoperative DVT or PE; (2) severe coagulopathy; (3) perioperative use of non-standard anticoagulation prophylaxis; (4) incomplete clinical data. Each participating hospital’s ethics committee approved the study protocol, and patients did not have to provide informed consent.
Sample size calculation
Based on the VTE incidence reported in previous studies (approximately 8%) and the expected number of predictors to be included (6-8), we estimated that at least 600 patients were needed to ensure adequate statistical power. Considering the possible missing data, we planned to include 650 patients. After excluding the patients who were eventually lost to follow-up, 621 patients were finally included. The screening diagram of the study cohort is shown in Figure 1. Study cohort screening.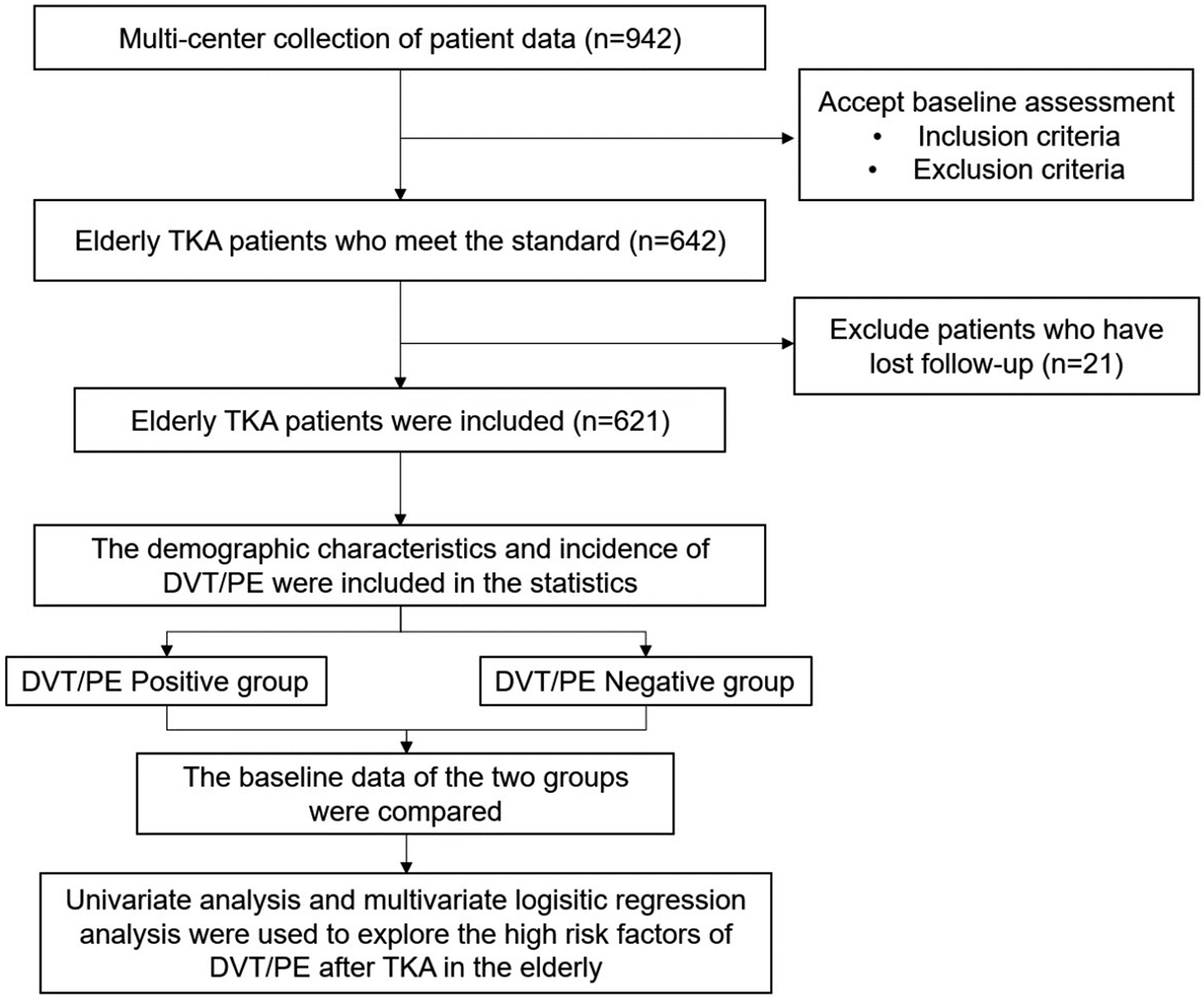
Data collection
Electronic medical records allowed us to collect the following information: (1) demographic characteristics, including age, sex, and body mass index (BMI); (2) medical history: diabetes, chronic obstructive pulmonary disease (COPD), heart failure, and other relevant conditions; (3) surgery-related parameters, specifically the duration of surgery; (4) postoperative management, defined by early mobilization (i.e., getting out of bed within 24 hours after surgery); and (5) Caprini score.
Primary outcome
This study looked at symptomatic PE or DVT within 90 days after surgery as its primary outcome. All suspected VTE cases were independently evaluated by two experienced physicians, and in case of disagreement, a third senior physician made the decision.
Deep vein thrombosis (DVT) diagnosis
In order to diagnose DVT, a combination of clinical symptoms and imaging examinations is necessary. Clinical symptoms mainly include: (1) unilateral lower limb swelling (circumference difference ≥ 3 cm); (2) local tenderness or pain; (3) positive Homan’s sign; (4) increased skin temperature and/or changes in skin color. Imaging examinations: (1) Compression Ultrasonography (CUS); venography.
Diagnosis of PE
The diagnosis of PE is also based on clinical symptoms and imaging examinations. The main clinical symptoms include: (1) sudden dyspnea; (2) chest pain (especially worse during inspiration); (3) hemoptysis; (4) syncope or presyncope.
For patients with suspected pulmonary embolism (PE), the following diagnostic algorithm is used: (1) Initially, conduct a D-dimer test. The PE can be excluded if the D-dimer results are negative and the clinical probability is low. (2) If the D-dimer is positive or the clinical probability is high, proceed with chest CT pulmonary angiography (CTPA). (3) For patients who are not suitable for CTPA (e.g., those with renal insufficiency or contrast agent allergies), ventilation/perfusion scanning (V/Q scan) is utilized as an alternative diagnostic method.
Statistical analysis
A statistical analysis was conducted using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation, and categorical variables as frequency (percentage). A t-test or Mann-Whitney U test was used for comparison of continuous variables, and a Fisher’s exact or χ2 test was used for comparison of categorical variables. Variables with a p value < .05 in univariate analysis were included in the multivariate logistic regression model, from which odds ratios (OR) and 95% confidence intervals (CI) were derived. The final model was refined through stepwise regression. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC-ROC), and model calibration was evaluated with the Hosmer-Lemeshow test. Statistical significance was defined as a p value < .05.
Results
Study population characteristics
Baseline characteristics of the study population (N = 621).

Incidence of deep vein thrombosis/pulmonary embolism
Incidence of deep vein thrombosis/pulmonary embolism by various Caprini risks.

Univariate analysis
Univariate analysis of risk factors for DVT/PE.

Multiple logistic regression analysis
Multi-factor logistic regression analysis of DVT/PE risk factors.

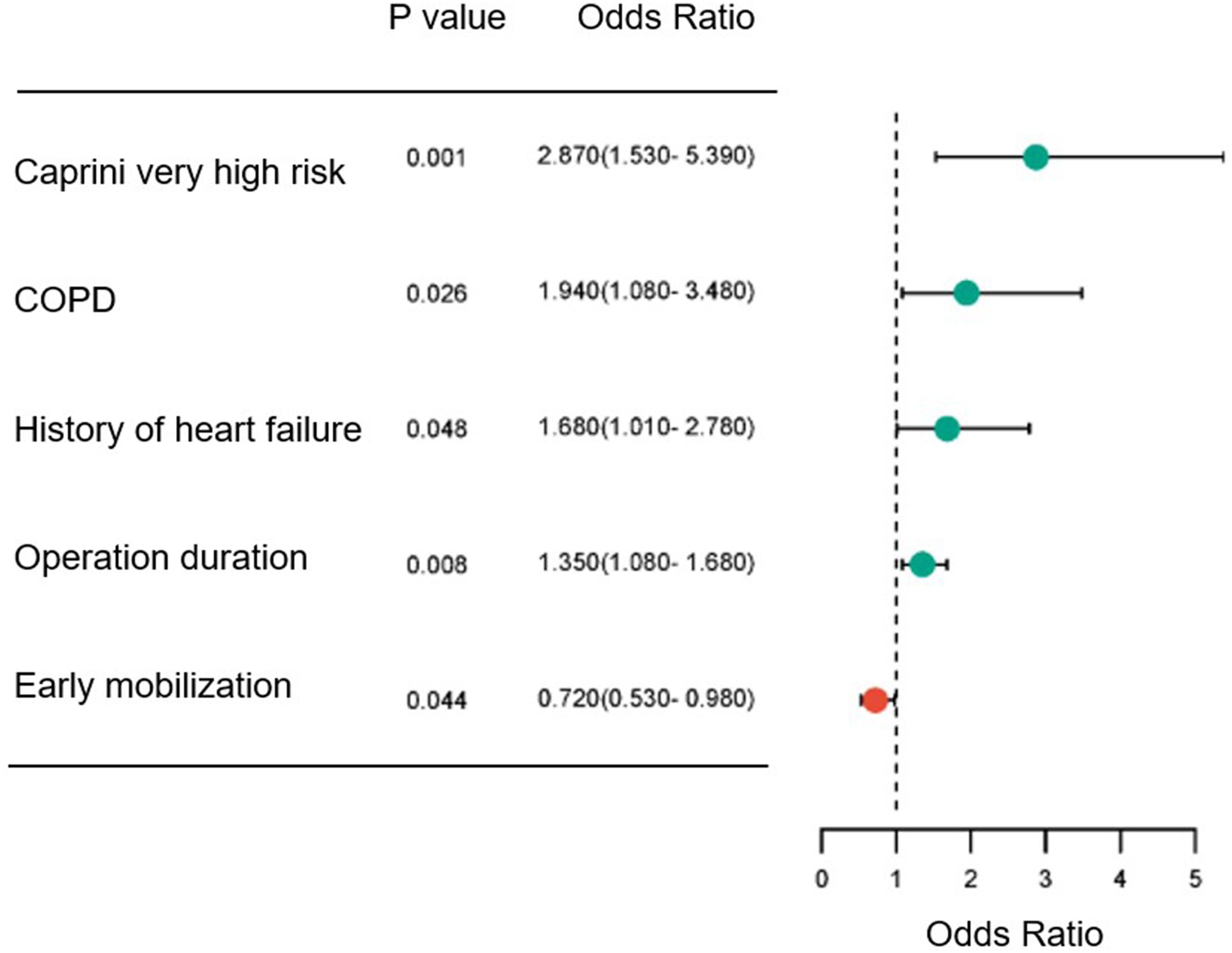
Forest plot of DVT/PE risk factors.
Predictive performance of risk factors
Predictive performance of the multi-factor logistic regression model and independent risk factors for DVT/PE

Abbreivations: AUC: area under the curve; COPD: chronic obstructive pulmonary disease; TP: true positive; FP: false positive; TN: true negative; FN: false negative.

ROC curves of the multi-factor logistic regression model and independent risk factors. Note: predicted: predict value from multi-factor logistic regression model; Caprinl: Caprinl very high risk; COPD: chronic obstructive pulmonary disease; HHF: History of heart failure; OD2: operation duration >2h, EM: early mobilization.
Discussion
As the global population ages, knee osteoarthritis has emerged as a significant health issue impacting the quality of life in the elderly. TKA is an effective treatment for advanced knee osteoarthritis, offering substantial improvements in pain relief and functional status. However, VTE complications, including DVT and PE, continue to pose a major clinical challenge following TKA. Despite the routine use of anticoagulant prophylaxis, the incidence of VTE remains elevated among elderly TKA patients. This underscores the critical need to identify high-risk factors and refine prevention strategies to enhance patient outcomes.
This study explored the high-risk factors for DVT and PE in elderly patients after TKA by multivariate logistic regression analysis. Our results indicated that the total incidence of VTE in the study population was 8.4% (95% CI: 6.3–10.5%) when receiving standard anticoagulation prevention. This incidence aligns with the previously reported range of 1.5% to 10%,10,11 but remains a significant concern. Our findings indicate that a very high Caprini score, comorbid COPD, a history of heart failure, and longer surgical duration are independent risk factors for postoperative VTE. Conversely, early mobilization within 24 hours after surgery serves as a protective factor. These results are crucial for enhancing risk assessment and developing more effective prevention strategies for postoperative VTE in elderly patients undergoing TKA.
This study found that the Caprini score was still an important predictor of VTE even in elderly TKA patients who received routine anticoagulation prophylaxis. This result is consistent with previous studies,12,13 further validating the applicability of the Caprini score in this population. However, it is noteworthy that 70.1% of the patients in this study were classified as extremely high risk, indicating a potential need for more nuanced stratification within the high-risk group. Future research should consider exploring the optimal cutoff value for the Caprini score or developing a specialized scoring system for elderly TKA patients, incorporating additional risk factors for more precise risk assessment.
Our results indicate that COPD is an independent risk factor for VTE in elderly patients undergoing TKA, which aligns with some previous research findings. 14 COPD may elevate VTE risk through various mechanisms, including systemic inflammation, blood hypercoagulability, and vascular endothelial dysfunction. 15 For elderly TKA patients with COPD, more proactive preventive strategies may be warranted, such as extending the duration of anticoagulation or intensifying anticoagulation therapy. Additionally, optimizing COPD management is crucial to mitigate postoperative complications. A previous history of heart failure has also been identified as an independent risk factor for VTE, potentially due to factors like blood flow stasis and altered coagulation function associated with heart failure. 16 For patients with a history of heart failure, a thorough cardiac function assessment and optimization prior to surgery are essential, and closer postoperative monitoring with individualized anticoagulation regimens may be necessary. Moreover, longer operative times were significantly associated with an increased risk of VTE, possibly due to venous stasis, tissue damage, and heightened inflammatory response resulting from prolonged surgery. Therefore, while maintaining surgical quality, efforts to minimize operative time may help reduce VTE risk. For procedures that are inevitably lengthy, additional precautions, such as intraoperative intermittent pneumatic compression devices, should be considered.
This study found that early mobilization within 24 hours after surgery is a protective factor for VTE. This is consistent with the results of multiple studies, 17 which emphasizes the importance of early functional training in VTE prevention. However, the implementation of early mobilization needs to be weighed against the patient’s pain management and other complications. Future studies can explore the optimal time and intensity of activity initiation, as well as how to safely and effectively implement early mobilization in high-risk patients.
Although statistical significance was not achieved in the multivariate analysis, our univariate analysis suggested that age, BMI, and diabetes may be associated with an increased risk of VTE. These factors have also been highlighted in other studies.18–20 Although age did not emerge as an independent risk factor in this study (p = .063), the average age of the VTE-positive group was slightly higher compared to the negative group (75.81 years vs 72.23 years). This difference may reflect cumulative risks associated with aging, such as decreased vascular elasticity and alterations in coagulation factor levels. Similarly, while BMI did not achieve statistical significance (p = .187), the mean BMI was slightly higher in the VTE-positive group (29.72 kg/m2 vs 28.25 kg/m2). The link between obesity and increased VTE risk is well-documented, 21 potentially due to pro-inflammatory factors released by adipose tissue and endothelial dysfunction. Additionally, diabetes was close to significance (p = .068) and may elevate VTE risk through effects on vascular endothelial function, the coagulation system, and the fibrinolytic system. Despite not reaching statistical significance in the multivariate analysis, these factors warrant attention in clinical practice, particularly when patients present with multiple potential risk factors concurrently.
This study utilized a large, multicenter design, focusing on elderly patients undergoing TKA who received standard anticoagulation prophylaxis. By considering multiple potential risk factors, it provides a comprehensive perspective on VTE risk assessment. However, the retrospective design may introduce bias, and the 90-day follow-up period may not capture the long-term risk of VTE. Additionally, specific types of DVT and PE were not differentiated. Future research should involve prospective validation, development of tailored risk assessment tools, exploration of individualized prevention strategies and early mobilization programs, and evaluation of new oral anticoagulants in this population.
Conclusion
This study identified several key risk factors for postoperative VTE in elderly patients undergoing TKA through multivariate analysis, including a very high Caprini score, COPD, a history of heart failure, and prolonged operation time. Additionally, the study highlighted the protective effect of early mobilization. These findings offer a crucial foundation for risk assessment and the optimization of prevention strategies in clinical practice. However, due to the complexity and potential severity of VTE, further high-quality research is necessary to enhance prevention and management strategies for this vulnerable population.
Footnotes
Author contributions
guarantor of integrity of the entire study:Zhanwen Zhou,Xiaohu Ma
study concepts:Yanbin Tian
study design:Xiaohu Ma,Jinguo Ma
definition of intellectual content:Xiaohu Ma,Jinguo Ma,Zhanwen Zhou
literature research:Binghan Chen,Yanbin Tian
clinical studies:Xiaohu Ma,Jinguo Ma; experimental studies:Xiaojin Wu,Binghan Chen,Yanbin Tian
data acquisition:Binghan Chen,Yanbin Tian
data analysis:Ming liu,Binghan Chen,Yanbin Tian
statistical analysis:Binghan Chen,Yanbin Tian
manuscript preparation:Ming liu
manuscript editing:Ming liu
manuscript review:Ming liu
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The simulation experiment data used to support the findings of this study are available from the corresponding author upon request.