
Abstract
Ankle fracture surgeries are common orthopaedic procedures. Fibular fixation is often an important component in restoring ankle stability. Fibular intramedullary nailing (fIMN) has gained recent interest as an alternative technique to fibular plating. This systematic review and meta-analysis was performed to compare the outcomes of fibular nailing versus fibular plating for all current available literature. A PRISMA-compliant systematic review was conducted across MEDLINE/Pubmed, Cochrane, and Embase databases for cohort and clinical trial studies comparing outcomes of fibular nailing and fibular plating of ankle fractures. Demographics and results of the studies were extracted from the articles. Outcomes of interest extracted included operative time, functional outcomes scores, hardware/loss of reduction, malunion/nonunion, re-operations, and wound complications. Meta-analysis of included studies used odds ratios and standardized mean difference when appropriate. Nine studies were included in this systematic review. Eight studies were then used for meta-analysis comparison. fIMN showed equivalent operating times to fibular plating. fIMN had equivalent outcomes when compared with fibular plating for hardware failure/loss of reduction, Olerud and Molander Ankle Score, malunion/nonunion, and re-operations. Fibular nailing showed a decrease in wound complications (OR: 0.35 [0.18, 0.66] (p = .001)) when compared with fibular plating. fIMN showed equivalent outcomes and decreased wound complications compared to fibular plating. fIMN is a safe and effective alternative treatment method that can be used by surgeons to treat distal fibula fractures.
Level of Evidence
3.
Introduction
Ankle fractures are one of the most common orthopaedic injuries, with thousands undergoing surgical fixation annually.1,2 These fractures often involve (in isolation or in some combination of) the medial and posterior malleoli of the tibia, the distal aspect of the fibula, and the distal tibia-fibula syndesmosis.1,3,4 These structures are all crucial in providing stability to the ankle joint, which is essential for weight bearing, ambulation, and basic daily function.1,3,4 Many ankle fractures meet indications for surgical repair due to instability of the ankle mortise caused by the fracture.5,6 Accurate restoration of these critical structures is crucial for preventing loss of ambulation and potential future complications, such as post-traumatic arthritis.5,7,8
Distal fibula fracture fixation strategies are of particular interest when treating ankle fractures.5,6 Fixation of fibula fractures has commonly been completed with open reduction and internal fixation (ORIF) through a lag screw and neutralization plating, bridge plating, antiglide plating, or other plating constructs.9,10 Some authors contend that fibular plating remains the gold standard for fixation of distal fibula fractures. 11 Another treatment is intramedullary screw fixation of the distal fibula, which yields comparable outcomes to traditional plating, along with the advantage of fewer delayed implant removals (with its own unique set of downsides such as decreased ability to perform syndesmotic fixation). 12 All of these treatments have shown overall high rates of union, positive outcome scores, and low complication rates.9–12 Another highly successful treatment in ankle fracture fixation is fibular intramedullary nailing (fIMN).5,9,13
fIMN is theorized to have several advantages over other treatment modalities, including smaller incisions, overall cost benefits, and endosteal fixation.14,15 These potential advantages have led to a rapid expansion in the use of fIMN. In the event of a concomitant syndesmotic injury, current fIMN systems allow for the placement of syndesmotic screws or suture buttons to achieve syndesmotic fixation. 9 The purpose of this systematic review and meta-analysis was to evaluate all available current literature on fIMN and to compare outcomes with traditional plating techniques. To our knowledge, this is the first systematic review to evaluate all literature, and not strictly randomized trials. Evaluating the non-inferiority of fIMN compared to fibular plating is important in demonstrating safety and justification for its use. The authors of this study hypothesize that fIMN will have equivalent outcomes when compared with fibular plating techniques.
Methods
Study design
This research activity was determined to be exempt or excluded from Institutional Review Board oversight in accordance with current regulations and institutional policy. This systematic review followed the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) statement standards. 16
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: (1) Cohort study or clinical trial comparing fibular plating vs fibular intramedullary nailing for ankle fractures (2) Was not a cadaveric study, (3) Manuscript was completed in English, (4) Studies were completed on or after January 1, 2000. Reviews, commentaries, letters to the editor, technique papers, and surveys were excluded.
Search strategy
PubMed/MEDLINE, Cochrane, and Embase databases were systematically searched for publications from January 1, 2000 to June 18, 2024. Comprehensive search strategies were developed using a combination of keywords, MeSH terms, and synonymous terms. The PubMed/Medline search was adapted to the Cochrane and Embase databases. See supplemental table 1 for a complete Pubmed Search.
One author (T.B.P.) performed the search. Three authors (T.B.P., C.R.M, A.D.L.) excluded irrelevant articles and duplicates based on title and abstract. The remaining articles underwent an independent full-text review by three authors (T.B.P., C.R.M., A.D.L.) and were assessed for eligibility based on established criteria. Any conflicts were resolved by discussion among the three authors.
Data extraction
Study demographic information was collected including the following: Patients, age, sex, implant type, fracture type, outcomes, and study results.
Quality assessment
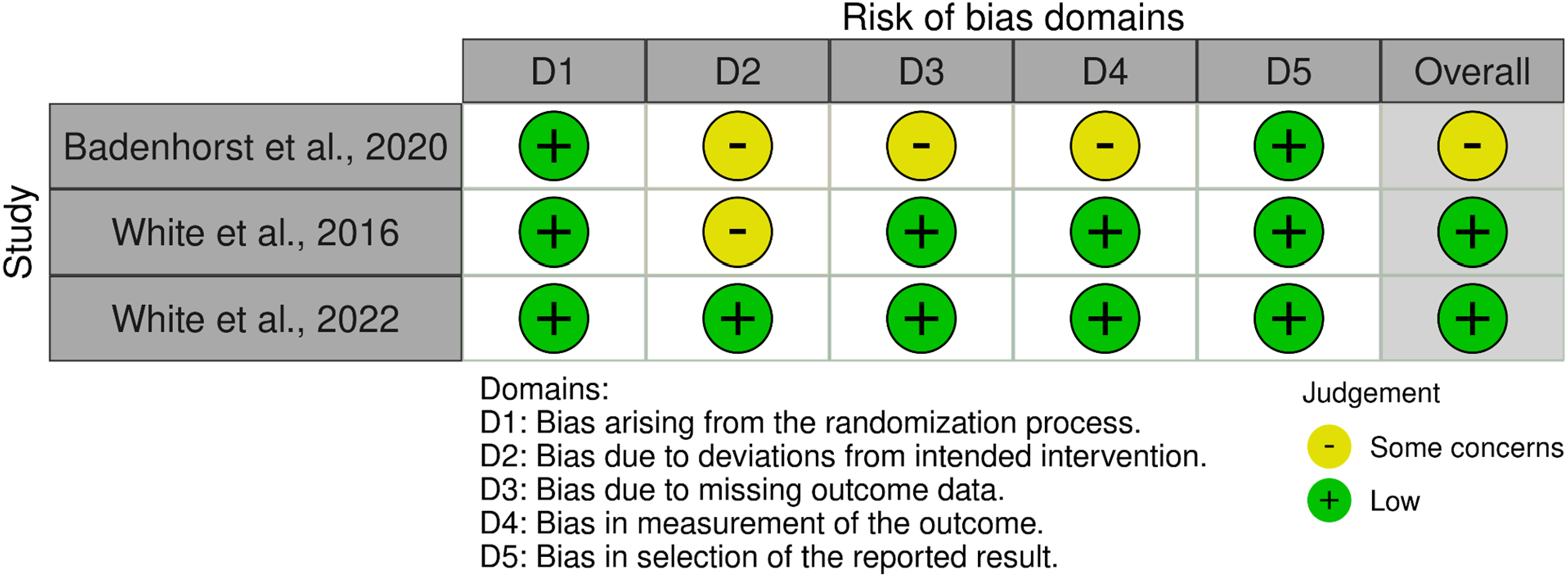
The Cochrane risk of bias 2 (ROB-2) for randomized control trials tool was used to assess all randomized control trials for bias. 17 The ROB-2 is composed of five domains which evaluates bias within randomized clinical trials. The bias is classified into three categories: high, some concern, and low. An overall bias assessment is produced upon the combination of the five domains.
The methodological quality of the nonrandomized studies included in the review was evaluated using the Methodological Index for Non-Randomized Studies (MINORS) Criteria. 18 The MINORS Criteria uses a validated 12-item checklist to ensure a critical appraisal of the study design through a standardized assessment. Three items were not applicable due to the retrospective cohort studies (i.e., prospective collection of data, loss to follow-up, prospective calculation of study size). A maximum of 18 points is possible for retrospective comparative studies, and studies with scores between 12 and 18 were considered high quality.
Statistical analysis
A meta-analysis was performed to compare fibular plating versus fIMN for the following outcomes: wound complications, defined as any occurrence of surgical site infection (SSI) or wound necrosis; hardware failure/loss of reduction; re-operations; malunion/nonunion; and Olerud & Molander score. These comparisons were analyzed with Mantel-Haenszel odds ratio (OR) estimates with 95% confidence intervals for dichotomous variables. A standardized mean difference (SMD) was used to compare continuous variables via a mean and standard deviation. Forest plots included studies with zero total events to maintain analytic consistency. 19 Heterogeneity was reported using the I2 statistic. Random and fixed effect models were used appropriately when the I2 statistic value was over and under 50%, respectively. A p value of less than 0.05 was considered statistically significant. Meta-analysis was performed using Cochrane’s Review Manager (RevMan, Version 5.4.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
PRISMA flow diagram
A preliminary search of three databases provided a total of 229 studies. 32 duplicates were removed. 187 abstracts and titles were screened, and 103 were removed for lack of relevance. 84 reports were sought for retrieval. All reports were obtained. Nine studies met the final inclusion criteria and were incorporated in this review. Eight studies met inclusion for meta-analysis. See Figure 1. PRISMA flow diagram.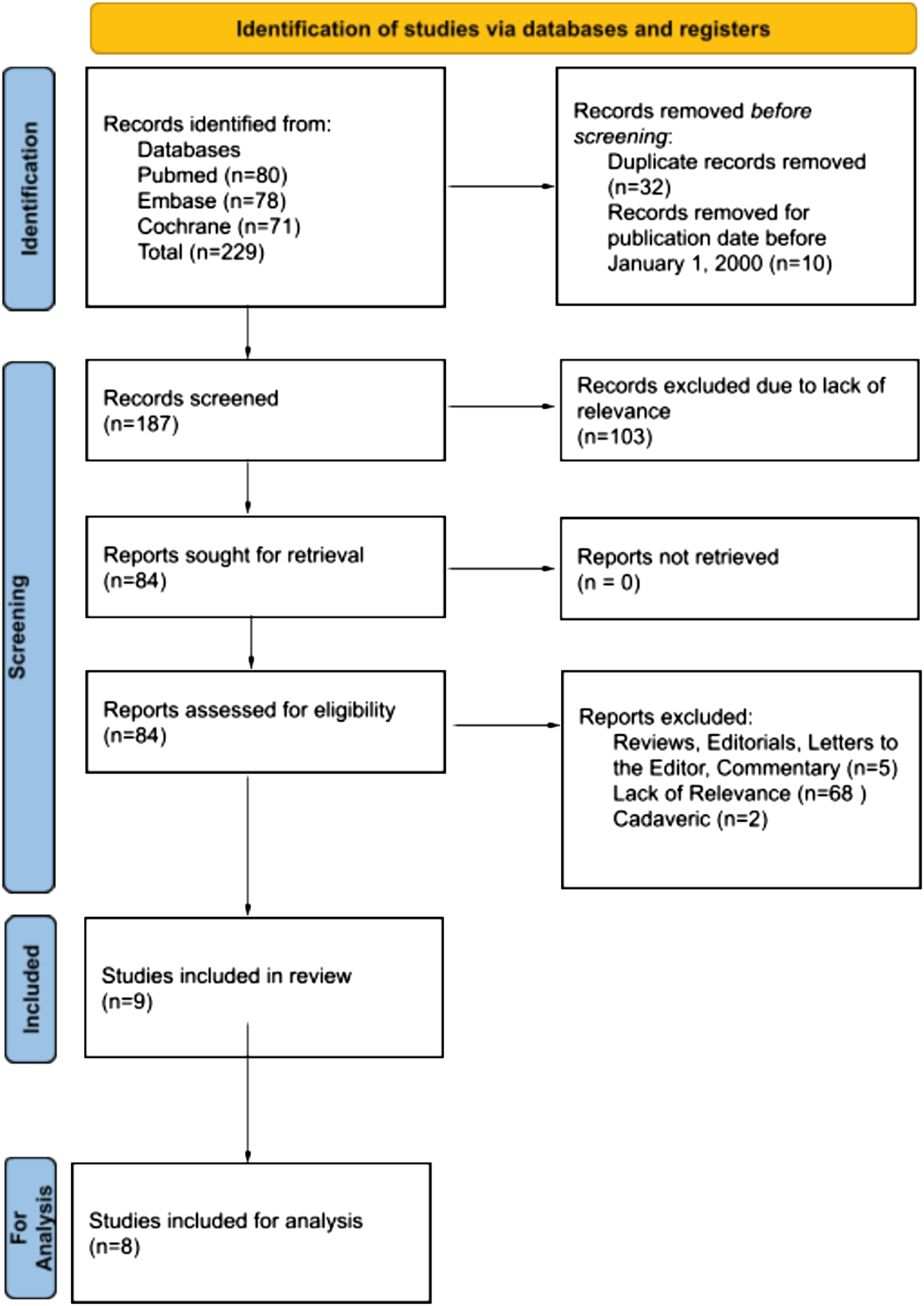
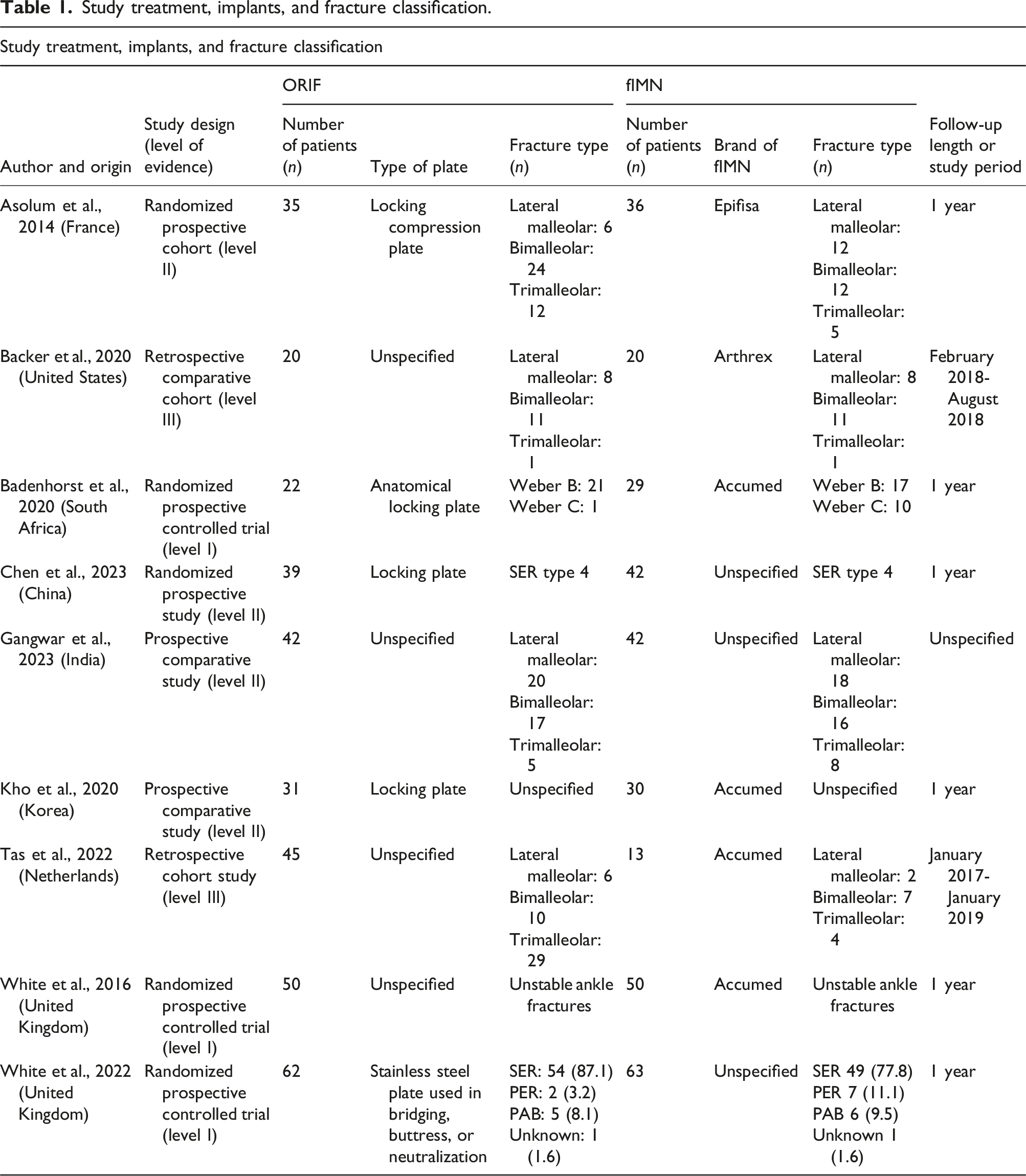
Study treatment, implants, and fracture classification
Study treatment, implants, and fracture classification.
Study demographics and outcomes
Study demographics and outcomes.

Quality analysis results
MINORS criteria quality assessment of non-randomized studies [Items are scored as 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate)].

Risk of Bias tool for randomized trials (ROB-2) plot.

Meta-analysis
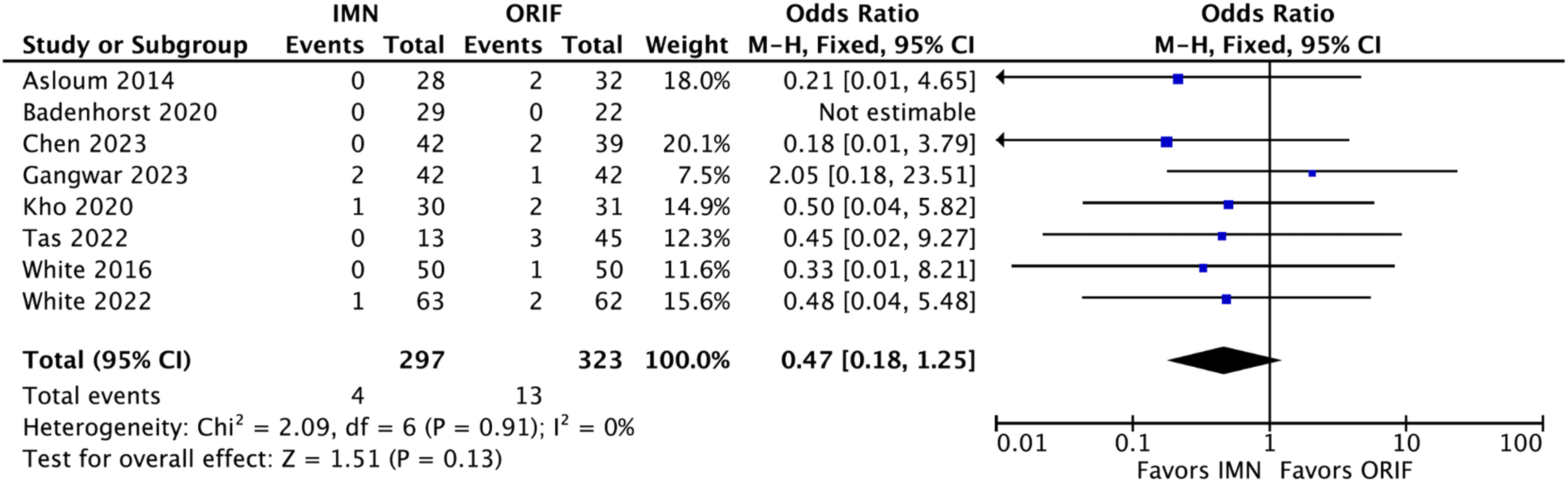
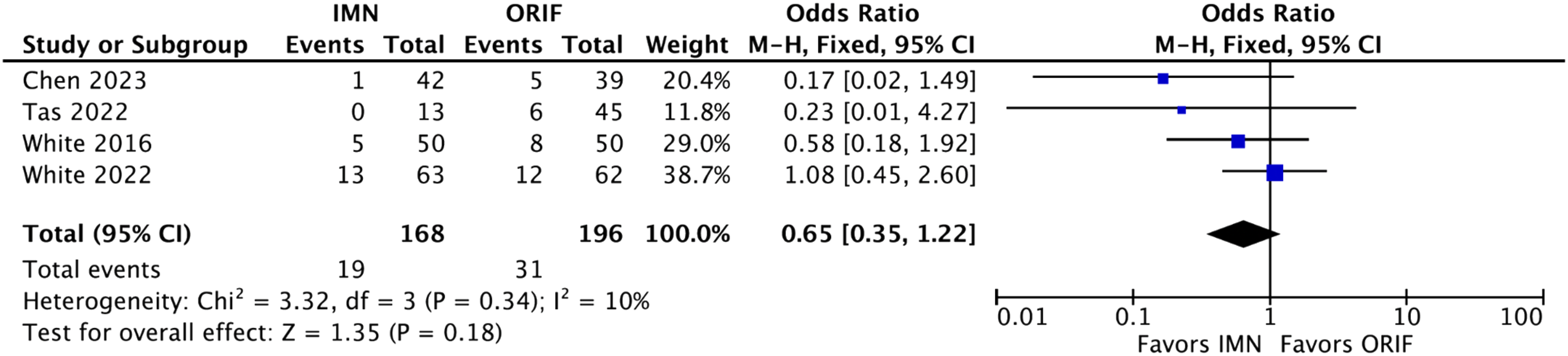
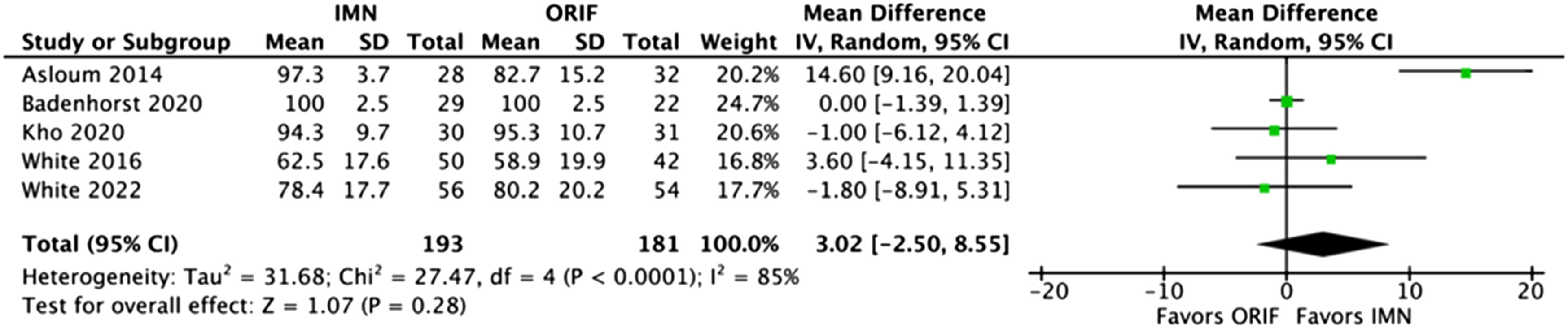
Wound complications analysis included eight studies which showed a statistically significant decrease in wound complications for fIMN when compared with ORIF with fibular plating (OR: 0.35 [0.18, 0.66] (p = .001)) (Figure 2). Loss of reduction/hardware failure analysis included eight studies which showed equivalent results for fIMN when compared with ORIF with fibular plating (OR: 0.47 [0.18, 1.25] (p = .13)) (Figure 3). Re-operation analysis included four studies which showed equivalent results for fIMN when compared with ORIF with fibular plating (OR: 0.65 [0.35, 1.22] (p = .18)) (Figure 4). Malunion/non-union analysis included seven studies which showed equivalent results for fIMN when compared with ORIF with fibular plating (OR: 0.68 [0.19, 2.48] (p = .56)) (Figure 5). OMAS score analysis included five studies which showed equivalent results for fIMN when compared with ORIF with fibular plating (OR: 3.02 [−2.50, 8.55] (p = .28)) (Figure 6). Wound complication analysis (Includes: Superficial SSI, Deep SSI, and wound necrosis). Loss of reduction and hardware failure. All Re-operations. Malunion/nonunion. Olerud & Molander ankle score.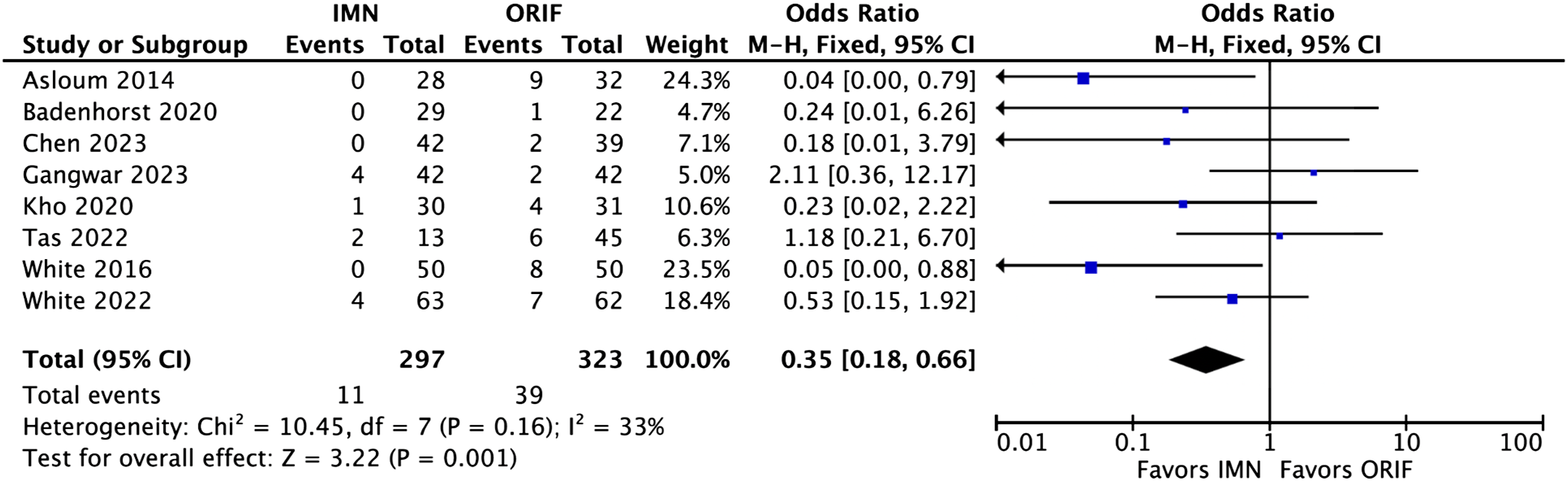

Discussion
fIMN was found to have equivalent outcomes to fibular plating when comparing Olerud and Molander Ankle score, malunion/nonunion, hardware removal/loss of reduction, and all re-operations. This study also found that operative time was equivalent for fibular nailing when compared with fibular plating. 21 fIMN was found to have a statistically significant decrease in wound complications when compared to fibular plating. This is the first systematic review and meta-analysis to our knowledge to evaluate all current comparative literature available when comparing fIMN versus fibular plating.
fIMN could be particularly of benefit with patients at high risk of wound complications. Some of these patient risk factors include diabetes, immunocompromise, injuries where additional nearby incisions are required (such as in pilon fractures), and in ankle fractures with soft tissue swelling.29,30 fIMN incisions are typically much smaller in size, 31 which could be the primary driver for decreased wound complications. Surgeons can effectively use this information in their preoperative planning to determine the most effective treatment for their patients, as these benefits could have a significant impact on the care of patients with fibula fractures.
While this study has shown that there are positive effects of fIMN, one potential concern is the cost of the implant when compared with plates and screws. Nailing has been proposed to decrease overall healthcare costs, as demonstrated in previous studies that evaluated cost benefit. 15 Peeperkorn et al., found that the median costs of fIMN implants to patients was $703 United States dollars (USD), and plates were $456 USD. 15 However, when comparing the overall median costs of treatment per patient, they found that fIMN cost $6444 USD and plating $7071 USD. 15 When they compared staged plating versus early fIMN, they found that early fIMN costs to the patient was $6298 USD and plating was $15,014 USD. 15 A second concern is the limited number of companies who currently offer fibular intramedullary nail implants. Access to these implants may be difficult for patients living in some locations due to lack of surgical services. 32 A third consideration is the learning curve associated with (for some surgeons) an unfamiliar fixation technique. 33
fIMN remains a relatively less common approach for fixation of fibula fractures. Future studies should evaluate the large-scale use of this device type with longitudinal outcomes to further evaluate the effects of fIMN. Future studies should also evaluate a complete cost analysis to determine episode-of-care costs associated with fIMN versus plating. At this point in time, fIMN is a safe and effective approach for fixation of fibula fractures. Surgeons can confidently use these implants in the operating room with literature to support their effectiveness.
Limitations
This study was not without limitations. There was the potential for missed literature; while our search was comprehensive and searched three major literature databases, it was possible that literature in another language or in a different database exists. Another potential limitation was that this study did not examine elastic fibular nails or intramedullary screws for similar efficacy. However, this study solely evaluated comparative studies regarding intramedullary fibular nail fixation versus traditional fibular plating, and therefore those investigations would be better evaluated in a separate study. A third limitation is the variations in comorbidities and fracture types. This was not evaluated due to variations within the literature and unclear reporting of these factors throughout some studies. Future clinical studies can prioritize these within their results. A fourth limitation is the wide age range of patients in the systematic review, with patient ages ranging from 40 to 80+ years of age. Two studies, Tas et al., 2022 and White et al., 2016 favor fIMN in the elderly population.26,27 These two studies may mask the outcomes of fIMN in younger populations, and is certainly a limitation of the current available literature. Future studies can evaluate fIMN by age. A fifth limitation is that our study evaluated all comparative literature, including older generation fibular nails, such as the nail used in Asolum et al., which lacks locking options or syndesmotic stabilization options. 20 These nails previously showed increased complications such as hardware migration, loss of reduction, and malunion. 9 This study may mask the true effect of the current nailing systems. As more literature becomes available on modern fibular nailing systems, future studies evaluating comparative literature can remove older generation nails. The fourth and fifth limitations of this study could contribute some potential bias to our study results. A final limitation is the potential variation in the different types of nail and plate systems used. These potential variations in products have not been evaluated in a comparison study clinically, and therefore differences remain unknown at this time.
Conclusions
fIMN showed mostly equivalent outcomes with the addition of decreased wound complications when compared with fibular plating. fIMN is a safe and effective method to fix unstable fibula fractures.
Supplemental Material
Supplemental Material - Comparison of fibula plating versus fibula nailing: A systematic review with meta-analysis of all current comparative literature
Supplemental Material for Comparison of fibula plating versus fibula nailing: A systematic review with meta-analysis of all current comparative literature by Troy B Puga, McKenna W Box, Charles R Marchese, Alan Lam, Sam Stegelmann and John T Riehl in Journal of Orthopaedic Surgery
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors of this study have no conflicts of interest to disclose. JTR is a consultant for and receives royalties from Arthrex Inc. The remaining authors have no potential competing interests to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
HCA Healthcare Disclaimer
This research was supported (in whole or part) by HCA Healthcare and/ or an HCA Healthcare-affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any affiliated entities.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.