
Abstract
Introduction
Oscillating saws are commonly used to remove casts placed for treatment of many conditions including extremity fractures. Cast saw burns are an unfortunate yet seemingly preventable iatrogenic complication of cast removal that not only cause harm to patients but also incur significant costs to the medical system. Reported rates of cast saw burns range from to 0.12 to 4.3 per 100 casts removed, and costs for a single burn can exceed $15,000 with lawsuit claims ranging from $2,995 to up to $125,000.1–5
Friction between the blade and the cast material can generate blade temperatures over 100°C.6,7 The burn threshold for adult skin is around 44°C and the pain threshold is around 43°C.8–10 In pediatric and geriatric patients, this threshold is even lower. 2 As a result, it is critical for practitioners to be aware of saw blade temperatures to decrease the risk of burn injuries during cast removal. While removal techniques have been suggested to help users decrease the heat generated during the removal process, to our knowledge no system exists to provide the cast saw user with information regarding how hot the cast saw blade is while a cast is being removed. 11
The purpose of this study was to develop and validate a real-time temperature feedback system for cast saw blades with LED light indicators for different temperature ranges. We hypothesized that when receiving real-time temperature feedback, cast saw users would keep the saw blade at safer temperature ranges when cutting casts. We also hypothesized that the number of times the cast saw blade touched the patient’s skin (as detected by the model) would decrease due to heightened awareness when using the device. To our knowledge, this is the first end-user tool for measuring saw blade temperatures in real-time with the goal of preventing cast saw burn injuries.
Materials and methods
Design
An infrared temperature sensor and LED device was designed by the authors and constructed with hardware by the Bresslergroup (Figure 1). The device was designed as a modified hood for the Stryker 940 cast saw, a widely used model of cast saw but with minor modifications could easily fit onto most any cast saw hood. The device measures temperature approximately 15 mm from the edge of the blade at two locations on the saw blade dividing the saw blade roughly into thirds. This information is transmitted to an onboard datalogger application that analyzes temperature readings once every second. The device has an LED light system that can emit four different variations: green, yellow, red, and blinking red (Figure 2). The LED lights can be on or off during operation of the device and the color of the lights is programmable to display a different color based on the maximum temperature being detected at the time, with a range set by the user. A provisional patent #62/906,401 was obtained for the device. (a) Infra-red heat sensor and LED system and quarter for scale with (b) left and right blade and ambient temperature sensors. Green, yellow, and red LED alerts corresponding with user-set temperature ranges. The green light across all three images indicates the sensor is fully charged.

Institutional Review Board (IRB) approval was obtained for this study. The testing setup is illustrated in Figure 3. Uniform model casts about 100 cm long were constructed on foam pool noodles. Each noodle was wrapped in one layer of copper to simulate a patient’s skin as part of the model to detect touches. This was then wrapped with four layers of cotton Webril and six layers of 4-inch fiberglass. Model cast thickness was determined by measuring the thickness of a random selection of 34 upper and lower extremity casts with a caliper and calculating the mean value (6.1 mm). Six layers of fiberglass approximated that measurement on our model casts. (a) Cast model pool noodle wrapped in 1 layer of copper to simulate patient skin followed by (b) 4 layers of webril and 6 layers of 4-inch fiberglass. (c) Illustration of testing setup.
The cast saw with the temperature sensor hood was connected to a Stryker 940 cast saw vacuum. The device was connected via a USB cable to a laptop to log temperature data. Custom software allowed the temperature data to be recorded with or without providing LED light feedback to the cast saw operator. A separate system based on a previously validated model using spikes of electrical conductivity from the cast saw blade to the copper sheeting was used to assess skin (“touches”). 7
Establishing temperature ranges
LED light thresholds.

Testing
Using the same model casts and testing setup, 15 additional subjects were tested. Participants included five cast technicians, five fellowship trained orthopaedic surgeons, and five medical trainees from a single level-I tertiary care pediatric trauma center. After obtaining informed consent from each participant, a standardized script was used to introduce the study setup and instruct participants (Appendix File 1). Each participant was asked to complete three cuts with the LED indicator off, followed by three cuts with the LED indicator on. Temperature and “touches” were collected throughout the duration of each run. The cast saw vacuum remained on throughout the duration of each test run. Participants were instructed to use their normal techniques for cast removal and cast saw cooling as they saw fit.
Analysis
The maximum temperature reading was used in the final temperature analysis. Standard descriptive statistics were used to report findings, including means and standard deviations for continuous variables. One-way and two-way analysis of variance (ANOVA) were used to evaluate differences between means and across participant groups. Significance for all tests was set at p = .05. Statistics were performed using SAS Version 9.3.
Sources of funding
No external funding was involved in this study. The investigators received an internal grant from their institution (The Children’s Hospital of Philadelphia) to fund development of the device prototype.
Results
Establishing temperature ranges
A total of 12 cuts across four cast technicians were included in our initial analysis to establish LED temperature indicator ranges. Cast technician experience ranged from 4 to 49 years of working at our institution. Temperature thresholds for the various LED alerts were established based on qualitative analysis of the saw blade temperature throughout the entire duration of each run (Table 1). The “safe” threshold at which the LED light remained green was determined to be < 31°C. This range marked approximately the 1/3 lowest temperature values of each cast technician’s test runs. The “warning” temperature range at which the LED light turned yellow was established as 31–37°C. The “unsafe” threshold at which the LED light turned red was determined to be >37°C. The “dangerously unsafe” threshold for blinking red was set at >40°C although was not differentiated from the continuous red range in our final analysis.
Device influence on temperature
Average time spent in each zone.

Values are reported as seconds, mean ± standard deviation. p-values describe the difference between the average time spent in each corresponding temperature zone with the LED off versus the LED on.
*indicates significance at p < .05.
Average percentage of time spent in each zone.
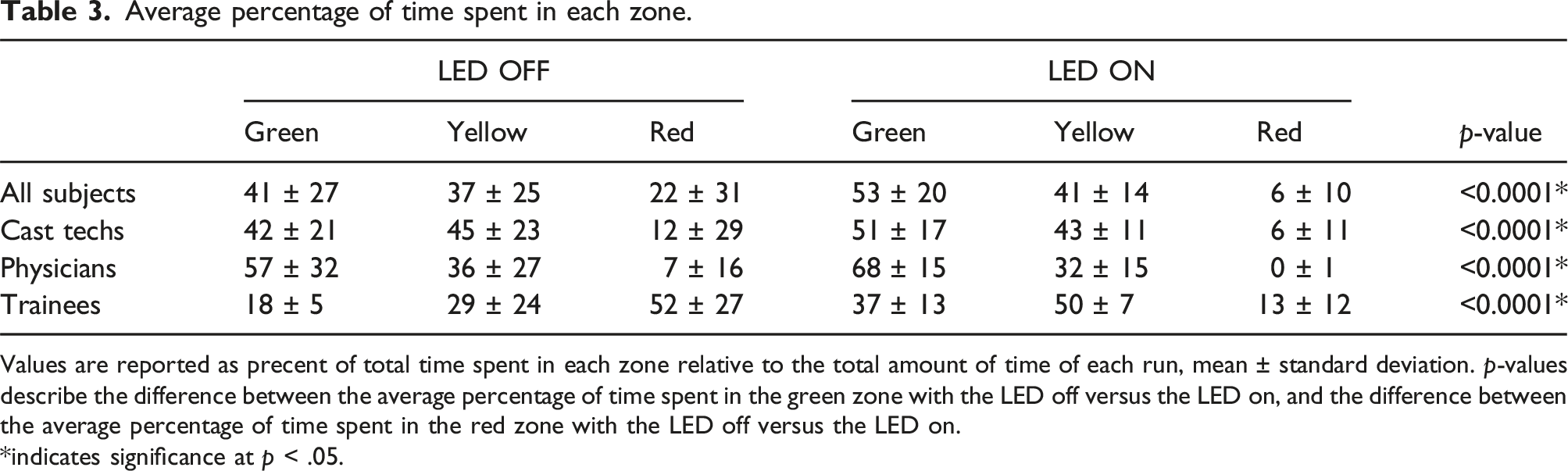
Values are reported as precent of total time spent in each zone relative to the total amount of time of each run, mean ± standard deviation. p-values describe the difference between the average percentage of time spent in the green zone with the LED off versus the LED on, and the difference between the average percentage of time spent in the red zone with the LED off versus the LED on.
*indicates significance at p < .05.
Device influence on skin touches
Average number of skin touches per test.

Discussion
Cast removal using an oscillating saw has the potential to cause significant patient harm with a reported rate of injury in up to 4.3% of cast removals.1–4 These injuries may lead to further expenses associated with additional medical care and legal claims of up to $125,000 per patient.1–3 The heat generated by cast saws can quickly reach thresholds for pain and cause burns. From our results, the minimum time it took to reach the red zone was just 20 s. This time is likely even less with poor removal technique, dull blades, and thicker casting materials.4,11 As a result, it is critically important for users to be aware of saw blade temperatures to help avoid burn injuries during cast removal. The purpose of this study was to develop and test a real-time temperature feedback attachment for cast saws and to determine whether the device decreased saw temperatures when operated by users of all experience levels.
Our findings suggest that the real-time temperature feedback system can alert users of unsafe temperatures and successfully decrease the amount of time the saw is operated at a potentially dangerous temperature. With the LED indicator turned on, the percentage of time users spent in the green “safe” temperature zone (<31°C) increased significantly while time spent in or above the red “unsafe” zone (>37°C) decreased significantly across all three experience levels (p < .0001). Our results suggest that this device has the potential to significantly decrease the risk of cast saw users heating the cast saw up to dangerous temperatures. The LED colors can be adjusted to fit different patient populations. While the pain threshold for adult skin is approximately 43°C, current literature suggests 39–40°C as the threshold for comfort in pediatric patients. 2 Participants in our study were responsive to the red zone indication, set at 37°C. Our findings suggest that users are responsive to the color indications, and that this device can decrease the risk of cast removal, particularly for patient groups who are most vulnerable to burn injuries.
Simultaneously, the number of times the blade contacted the model “skin” showed a downward trend when the LED light was active across all experience levels. It is possible that with a real-time feedback system, users also exercise more caution when handling the cast saw, thereby decreasing the likelihood of contacting the patient’s skin and chance of injury. Although the decrease in number of skin touches was not statistically significant in our study, it is possible that increased sample size may produce statistically significant findings. Still, this secondary finding demonstrates the possible ability of the feedback system to not only improve temperature control but also improve cutting technique and depth by continuously bolstering user awareness and caution.
A primary limitation of this study was sample size. The results presented in this study demonstrate the influence of a prototype on participants from a single institution. A-priori power analysis assuming independence across all cast saw users and test runs to detect a medium effect size of 0.25 and using an ANOVA with experience level as interaction, a sample size of 158 test runs was required to achieve 80% power at 0.05 level of significance. Provided that each participant completed 6 test runs (e.g., 3 with the LED off, 3 with the LED on), 27 users were required to satisfy the a-priori power analysis. However, due to cost and time limitations, the study was limited to 15 subjects subdivided across experience levels.
An additional limitation of the study was that it was conducted on models rather than live patients. However, the model casts were designed to simulate patients. Within clinical practice, there is also use of variable casting techniques and material, particularly within the setting of acute fracture care. Even so, given that the primary objective of the study was to determine the effect of the device on influencing user behavior, we believe that our results are likely to remain translatable to a real clinical setting despite such variability.
Despite these limitations, we believe this feedback system can improve safety of usage in participants across all experience levels ranging from experienced cast technicians to novice trainees. Previous studies have demonstrated nearly all clinicians make inadvertent contact with the underlying skin when removing casts, regardless of experience level or education. 12 This device has potential to be used in teaching less-experienced users such as cast technician trainees and medical trainees safe cast saw practices and by professionals within outpatient clinics, emergency departments, and operating rooms to improve the safety of the cast removal process. Alternatives to limit casting sequalae including custom fracture orthotics are not universally available and cannot be used in the acute setting. This device may serve as a more accessible, simple, and user-friendly solution. Future study may focus on the clinical integration of the temperature feedback device with live patients with various cast locations and sizes.
Cast saw injuries are seemingly preventable iatrogenic complications. Our study presents the first device to provide real-time temperature feedback for cast saw users. The results of this study indicate that this real-time temperature sensor has the potential to improve patient care and subsequently decrease medicolegal costs associated with burn injuries. The promising results from these tests suggest the benefits of future production of a pilot product which may help decrease the widespread burden of cast saw burn injuries.
Footnotes
Authors’ note
Dr B. David Horn and Dr J. Todd Lawrence hold a provisional patent #62/906,401 on the device discussed in this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.