
Abstract
Introduction
Various treatment modalities have been presented from past to present for the treatment of bone segmental loss. 1 Segmental bone loss may occur in trauma, osteomyelitis, congenital anomalies, skeletal system tumor resection, prosthetic surgery, and spine surgery. 2 The most preferred methods for reconstruction of these losses include autogenous bone grafting, surgery with bone allograft, distraction osteogenesis and free-vessel bone grafts. 3 In methods other than free vascularized fibula grafts (FVFG), the lack of continuous blood supply to the graft results in lower union rates, and the insufficient mechanical strength increases the risk of complications. Furthermore, these methods may be inadequate for the reconstruction of large segmental defects.4,5
With the development of microsurgical techniques, vascular grafts that preserve their biological properties in the transplanted tissue have come to the agenda. 6 Most of the bones transplanted with this method survive. No bone resorption is observed during union and fusion. Therefore, vascular autografts preserve their integrity more in the first 6 weeks 7 In vascularized bone grafts, the continuity of blood flow is a critical factor for bone healing and graft hypertrophy. 8 This process enhances the graft’s resistance to infection, accelerates the healing process, and improves its ability to withstand mechanical loading due to hypertrophy.9,10 Consequently, the incidence of graft resorption and stress fractures decreases. 11 Peat and colleagues reported that vascularized bone grafts yield more successful outcomes than delayed and early conventional bone grafting procedures. 12 Fibula, costa, tibia, olecranon and iliac bone can be used as grafts. The most commonly preferred of these is the vascularized fibula graft. Vascularized bone grafts can be used successfully in treating areas with bone loss greater than 6 cm for various reasons. 13
In this study, we aimed to evaluate the relationship between union time, functional outcomes, and quality of life in patients who underwent reconstruction with free vascularized fibula autograft for segmental bone defect resulting from resection of bone tumor in our clinic between 2005 and 2021. Secondarily, we attempted to identify factors affecting the union time of patients. Additionally, we assessed patients’ quality of life and functional outcomes using both physician-dependent and independent assessment tools, including the Visual Analog Scale (VAS), the Musculoskeletal Tumor Society (MSTS) extremity score, and the Short Form-36 (SF-36) quality of life scale, ensuring an objective analysis.
Materials and methods
This single-centre study was performed with ethics committee approval and in accordance with the Declaration of Helsinki (I10-636-21). Data of patients who underwent reconstruction with vascularised fibula graft for segmental bone defects larger than 6 cm after resection of bone tumours in our institution between December 2005 and December 2021 were collected retrospectively. The relationship between postoperative clinical functional scores and union was analysed retrospectively. Preoperative and postoperative hospital records, radiological examinations and clinical functions of patients who underwent repair with free vascularised bone graft were analysed. The oncological diagnoses of the patients were determined according to the pathology results. The follow-up forms, photographs and files of the patients were examined and the postoperative follow-up periods were determined. Patients with a follow-up period shorter than 24 months, patients who had undergone previous surgical intervention on the same extremity, patients who died during the follow-up period, and patients without regular hospital follow-up were excluded from the study. Patients without bone union were also excluded from the study. The remaining patient group was included in the study. Bone union was evaluated by X-ray films. Each of the proximal and distal osteotomies was considered to be united if union was seen in three of the four cortices on anteroposterior and lateral radiographs.
In this study group, demographic variables such as age, gender, etiology, anatomical location and extent of bone loss (cm), chemotherapy and radiotherapy status were evaluated. Functional outcomes were standardised by calculating Musculoskeletal Tumor Society (MSTS) and Short Form-36 (SF-36) scores at 24 months postoperative follow-up of patients with free vascularised fibula graft. After discharge, patients were scheduled for routine oncological follow-up at 6 weeks, 3, 6, 9, 12 and 18 months and at the second year follow-up. Bone union was evaluated by clinical examination of the surgical site and radiographic imaging. During the follow-up of bone union, the proximal and distal ends were evaluated separately by X-rays, and the bone segment that took the longest time to achieve union was considered as the union time. In patients with localised pain at the surgical site, union status was occasionally evaluated by computed tomography (CT).
Statistical analysis
When evaluating the findings obtained in the study, SPSS (Statistical Package for Social Sciences) for Windows 15.0 program was used for statistical analysis. Descriptive statistical methods (mean, standard deviation, percentage) were used to evaluate the study data. Paired t test was used for intra-group comparisons of normally distributed parameters. The chi-square test was used for comparison of qualitative data. ‘Mann Whitney U test’ was used to determine the difference between nonparametric tests. The results were significant at 95% confidence interval and p < .05 level.
Results
After repair with free-vessel fibula graft was planned for the treatment of long bone loss, it was performed in 47 patients. Since union was not observed in two patients, the study continued with 45 patients. These patients included 20 females and 25 males and ranged in age from 10 to 74 years (mean age 31.3 years). Of the 17 patients operated for upper extremity tumours, six were female (35.2%) and 11 were male (64.8%). Of the 28 patients operated for lower extremity tumours, 14 were female (50%) and 14 were male (50%).
When the relationship between the upper and lower extremity difference with union time and MSTS score was analysed, the difference between union times was considered statistically significant (p = .03). However, there was no statistically significant difference in MSTS score (p = .60).
Tumor localization in extremities.

The mean defect size during surgery was 13.73 cm (min: 6.07, max: 22.44). When the graft lengths were analysed, the mean graft length was 16.99 cm (min: 7.40, max: 24.92). Free vascularised fibula graft was used in isolation in 22 of 45 patients (48.88%) and with the ‘hot-dog’ technique in 23 patients (51.12%). A mean of 2.27 units (min: 1, max: 5) of erythrocyte suspension was administered intraoperatively and intraoperative fresh frozen plasma was required in eight patients. The mean operation time was calculated as 8.89 hours (min: 4, max: 13). The mean hospital stay was 12.14 days (min: 4, max: 45). The mean follow-up period was 50 months (min: 24, max: 147) and nine patients (19.15%) died during this period.
During the follow-up period, direct radiographs and computed tomographs used in some patients were evaluated and it was determined that graft union occurred in 45 patients and the mean union time was 6.7 months (min: 2, max: 14).
Various complications developed in 11 of 45 patients in the postoperative period. Treatment with superficial debridement was sufficient in five of seven patients with infection, while gastrocnemius flap was applied in addition to debridement in one patient with deep infection. In one patient with osteomyelitis, Ilizarov external fixation was performed with preservation of vascularised fibula graft after debridement.
One patient developed plate fracture and revision was performed with retrograde nail. In one patient who achieved union in the eighth month, a segmental shift was performed with the Ilizarov method after resection because of recurrence 11 years later. Two of the three patients with delayed union were reconstructed with iliac wing graft after debridement due to infection. In one patient who developed a fracture in the fifth month, revision was performed using an iliac wing autograft and union was achieved on direct radiography within 9 months after this procedure. No patient required amputation.
The duration of union was divided into four groups as 0-3 months, 3-6 months, 6-12 months and after the 12th month (Figure 1). Late graft union was detected in one patient in group 4. Since union could not be achieved in the postoperative period, this patient underwent a second operation with iliac wing graft and union was achieved afterwards. Preoperative and postoperative chemotherapy and radiotherapy treatments were analysed and classified (Table 2). Bone union time of upper and lower extremities. Preoperative and postoperative radiotherapy and chemotherapy treatments for patients.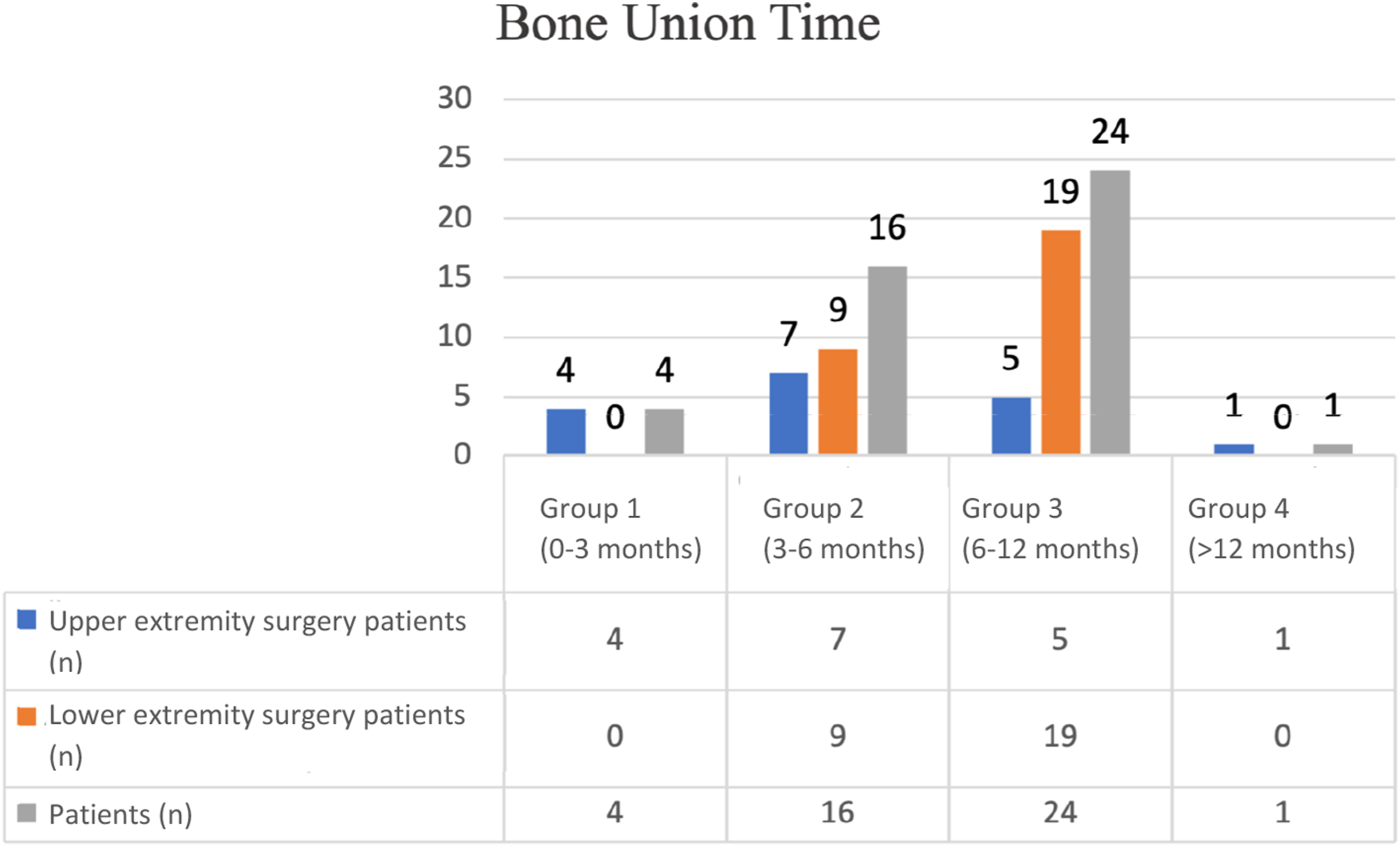

Statistical analysis of the SF-36 quality of life scale.
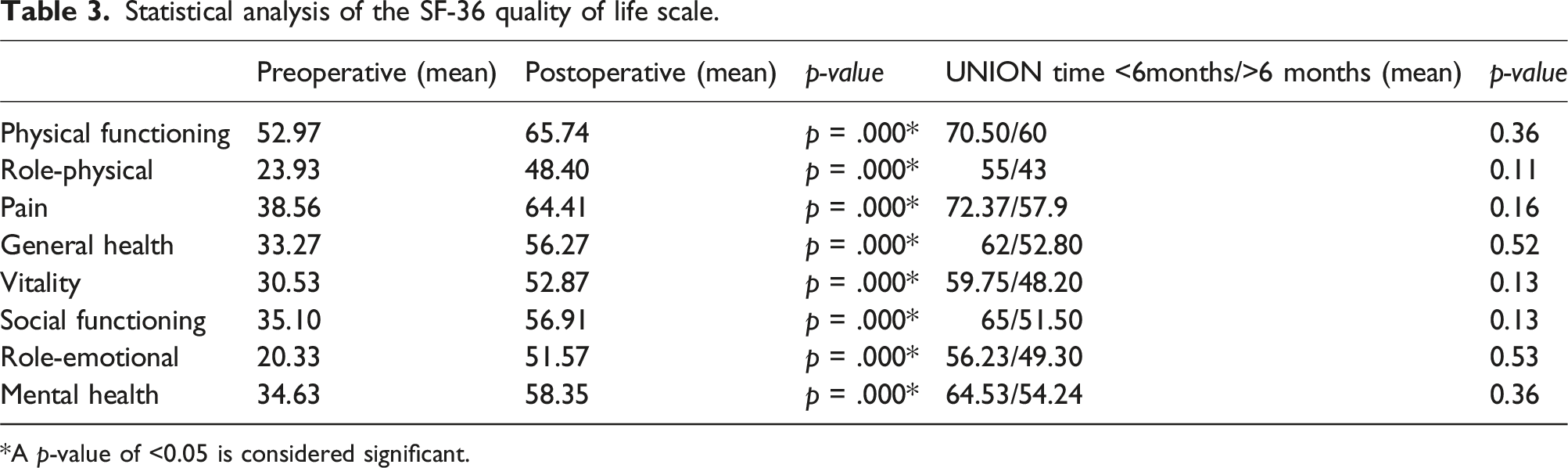
*A p-value of <0.05 is considered significant.
When VAS and MSTS scores were compared, the mean VAS score was 3.75 and MSTS score was 20.25 in four patients with union between 0 and 3 months. The mean VAS score was 2.55 and MSTS score was 23.11 in 16 patients with union within 3-6 months. The mean VAS score was 4.18 and MSTS score was 21.50 in 24 patients with union within 6-12 months. After 12 months, the VAS score was one and the MSTS score was 12 in the only patient with union (Figure 2). Association of bone union time with pain and functional outcomes.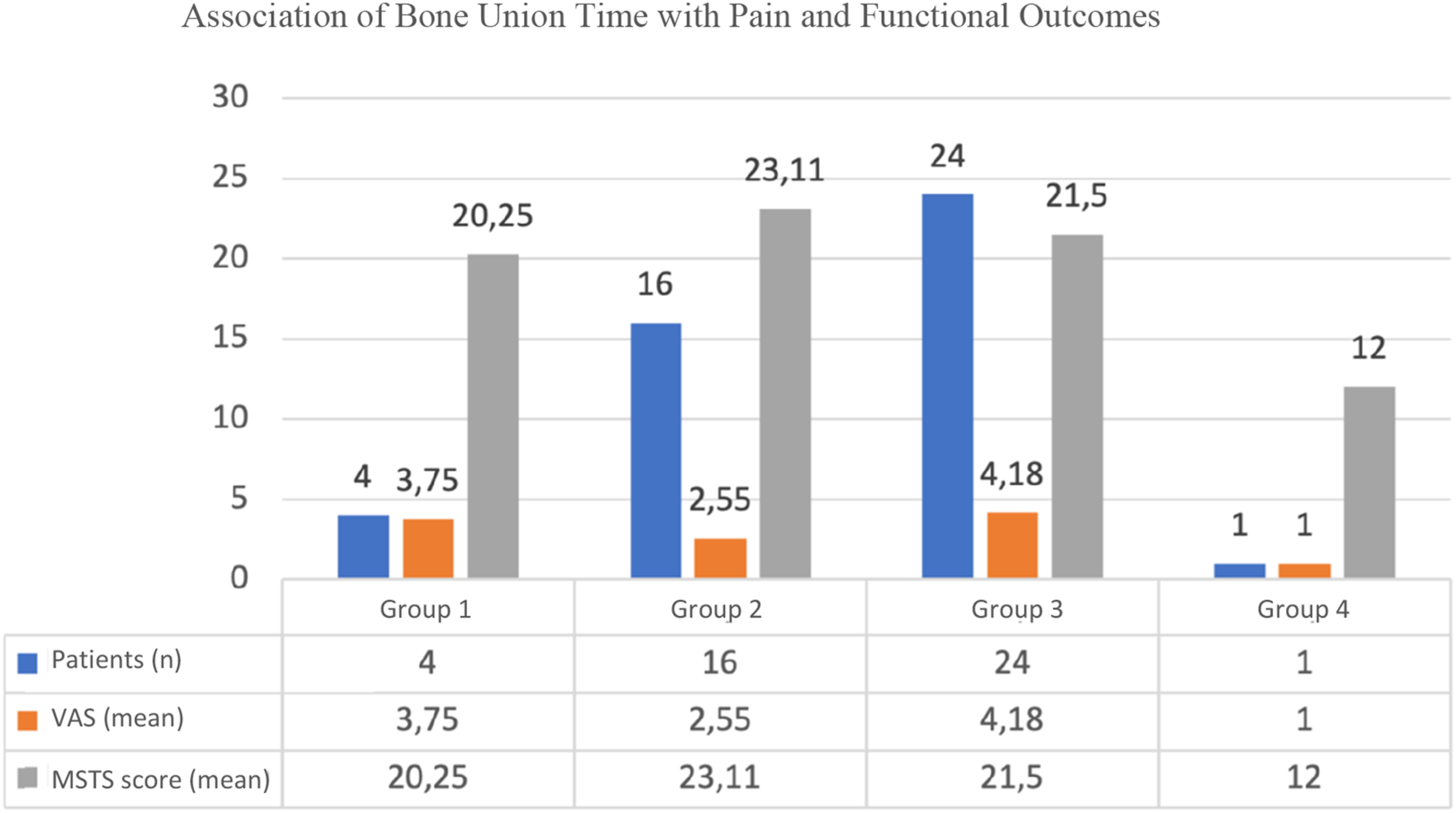
For comparison in terms of graft union time and MSTS score, the patients were divided into two groups as those with union before 6 months and those with union after 6 months. At the end of 12 months, patients without bridging callus formation in three different planes at the distal or proximal end were classified as non-union, while those with bridging callus formation in three different planes at the distal or proximal end were included in the delayed union group. In the study, one patient developed bridging callus in three different planes at the proximal end of the graft before the 12th month, whereas at the distal end, bridging callus formed in three different planes at the 14th month, and this patient was included in the delayed union group.
Statistical analysis of factors affecting bone union time and MSTS score.

*A p-value of <0.05 is considered significant.
Correlation of union time with MSTS score, VAS score, and age.
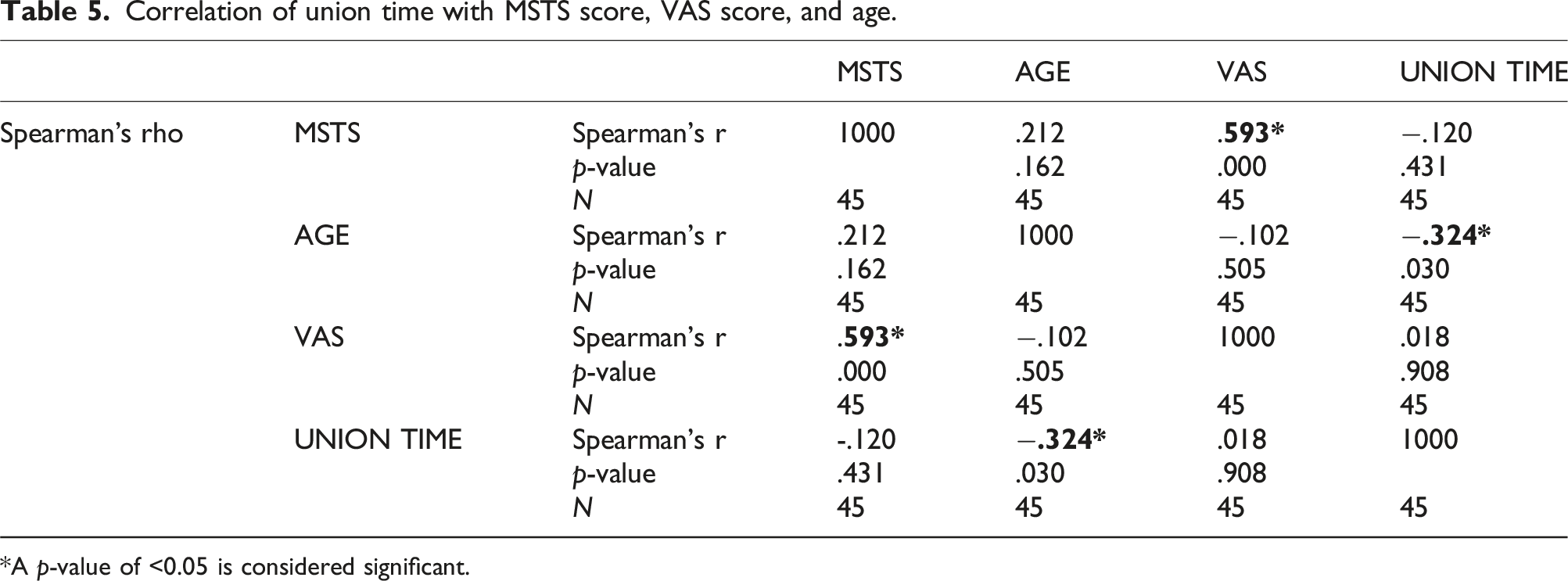
*A p-value of <0.05 is considered significant.
Discussion
In this study, we aimed to demonstrate that free vascularized fibula bone graft provides a reliable and functional solution for reconstruction after resection of upper or lower extremity bone tumors and to examine the relationship between this function and union time. The average bone union time of the patients was determined to be 6.7 months, and at the end of the 24th month, all patients had similar MSTS and SF-36 functional outcomes.
Xu et al in 2020 divided 18 patients who underwent reconstruction with FVGF due to osteosarcoma into two groups as upper and lower extremity according to the extremity where the tumor was located and found no difference in union time and MSTS scores between these groups. 14 In this study, we found that the union time of patients who underwent FVFG reconstruction for upper extremity defects was shorter than that of lower extremity patients (p = .03). However, this did not have a strong effect on the limb function of the patients at the end of 24 months (p = .60). Double plate was applied to our patients who underwent reconstruction with FVFG due to lower extremity tumour. We think that the longer union time is due to the fact that the fibula is exposed to less stress in the lower extremity due to double plate fixation. However, when we analyzed both the MSTS and SF-36 scores of the patients, it was seen that this did not have a lasting effect on the patient’s functions at the end of 24 months, even though the union time was prolonged.
The MSTS is frequently used because of its ease of use and because it is an acceptable assessment system for patient-centered outcomes in evaluating limb function after musculoskeletal oncologic surgery in general.15,16 In addition, the MSTS has standardized clinician reporting of patient-centered outcomes of limb salvage procedures. 17 The fact that it is reported by the clinician and that it does not cover objective movements such as sitting and standing much has been criticized by some authors, and some studies have even reported that the MSTS is moderately related to physical performance and cannot score some important differences in limb function. 18 In this study, we think that it is more appropriate to perform a holistic functional assessment of the patient with the SF-36, which reveals the patient’s self-administered physical, mental, emotional and social functionality as well as pain and general health assessment. In some studies in the literature, SF-36 scoring was used to evaluate the functions of patients after FVFG.19,20 Unlike these studies, this study is the first study to examine the effect of union time on SF-36. In our study, the scores of the SF-36 subheadings of the patients were higher than preoperatively and this was statistically significant. When we grouped the patients according to the duration of bone union, the SF-36 functional scores were higher in patients with a bone union time of less than 6 months, as expected, but this increase was not statistically significant (p > .05). This showed us that the effect of union time on patient function was limited.
It has been shown that MSTS score is higher after reconstructive surgeries compared to amputation.21,22 Fuchs et al. showed a mean MSTS score of 76.6% in 21 patients who underwent reconstruction after tumor resection. This score may be higher in pediatric patients. Indeed, in a large study in which FVFG was performed in pediatric patients, postoperative MSTS scores ranging from 88.3%–100% were shown for all patients. 23 In our study, the mean MSTS score was 70.3%. This may be related to our postoperative complication rate of 24.4%, but this score is still consistent with the literature. 11
Common complications of FVFG include nonunion, fracture, infection and revision surgeries.24–26 In this study, union time was 6.7 months. A union time compatible with the literature was observed. 11 In many studies, FVFG has been described for reconstruction after tumor resections, but patient function and its relationship with union have not been shown in studies.24,27
In a systematic review published by Mark et al. including 56 studies, complications were reported in 50 studies. The overall complication rate was 56.9% and the most commonly reported complication was fracture (11.7%). Other commonly reported complications were nerve injury (7.5%), infection (5.7%) and claw finger (3.3%). When the reoperation rate was analyzed in the same study, it was observed that 34.5% of the patients underwent reoperation on average. The most common reasons for reoperation were fracture (22.8% of reoperations), nonunion (17.7%) and infection (13.9%). 28 In general, infection rates in FVFG are around 6% on average and this rate is low compared to reconstructions using allograft with an infection rate of 20%–30%.29–31 In our study, a total of 11 (24.4%) patients developed complications. When we analyzed the patients with union in this study, the number of patients who underwent reoperation was 11 (24.4%) and both our complication rate and reoperation rate were lower than the rates reported in the literatüre. 28 In addition, complete union was observed in a total of 45 (95.7%) patients in our study. With close follow-up of the patients after meticulous surgery, status of union or non-union was detected on time and also complications such as infection were picked up and treated on time and we believe that this contributed to high union rate in our cohort. In 2 patients, union was not observed and atrophy developed. Revision surgery was performed in one of our patients at the 25th month and the other patient is still being followed up.
We found that the development of postoperative complications prolonged the union times of patients who underwent reconstruction with FVFG (p = .007). However, the effect of this situation on the function of the patients was not found to be significant (p = .10). Although the healing and union times of the patients were delayed because half of the complications of our patients involved deep tissue or bone, our mean union times are compatible with the literature. 32 It has been reported in many studies that chemotherapy and/or radiotherapy decreases bone remodeling in a dose- dependent manner.24,27 Although no statistically significant differences were observed between the presence of neoadjuvant and/or adjuvant chemotherapy and radiotherapy with respect to graft union times (p = .88) and MSTS scores (p = .22), these treatments are believed to adversely impact bone union. Subgroup analysis based on neoadjuvant or adjuvant chemotherapy and radiotherapy treatments could not be performed due to the insufficient sample size. However, it is hypothesized that these treatments contribute to the prolongation of the mean union time. In addition, the MSTS scores showed that patient- centered outcomes were not significantly affected by chemotherapy and/or radiotherapy.
There are some limitations in our study. First, our study is retrospective and there is no control group. In addition, patients who underwent upper and lower extremity reconstruction with FVFG were combined in our study. As a matter of fact, due to the differences in weight bearing, range of motion and participation in activities of daily living of the upper and lower extremities, differences between the reconstruction results can be expected. The effect of radiotherapy and chemotherapy on union and MSTS score by forming subgroups requires studies with a larger number of patients.
Conclusion
Although biologic reconstruction with FVFG has a relatively high complication rate and causes significant functional limitation in the early postoperative period, it may result in long-term recovery with acceptable functionality after cortical union is achieved. Our study is one of the rare studies to examine the correlation of bone union times of patients undergoing FVFG reconstruction with both physician reported as well as patient reported outcome measures. It also draws attention by examining the effect of many conditions on graft union time and functional score together. Although the bone union times of the patients were above the average union times, the limb functions of the patients were acceptable at the end of 24 months.
Footnotes
Acknowledgments
Not applicable.
Author Contributions
MCG designed the manuscript, researched the data, and wrote the text; MOK analyzed the data and researched the references; MCG designed the manuscript; HYY provided consultancy for the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
All data generated or analysed during this study are included in this published article.