
Abstract
Keywords
Introduction
A number of femoral component designs exist in total hip arthroplasty (THA), each offering theoretical risks and benefits to patients.1–4 Risk reduction of intra-operative and postoperative complications, including periprosthetic fracture and aseptic mechanical loosening, remain primary goals. 5 Variables in femoral stem design include proximal geometry (e.g., taper), metaphyseal or diaphyseal fixation, broach technique and philosophy, presence of a collar, coating, and metallurgical composition.6–8 Differences in these variables correlate to proximal femoral load transfer and osseointegration of stem to help maintain position over time and avoid subsidence. 9 In metaphyseal engaging stems, failure to achieve early metaphyseal fixation contributes to aseptic loosening. 10
Among contemporary femoral stems, the ACTIS stem (DePuy Synthes, Warsaw IN, USA) has gained in popularity since being introduced nationwide in 2018 and was the most commonly implanted femoral stem for elective primary total hip arthroplasty in 2022. 11 It is a collared, triple-tapered, titanium, cementless femoral stem fully coated with hydroxyapatite. It is designed to “fit and fill” the proximal femoral metaphysis. 12 Initially marketed as a stem designed for the anterior approach, prior studies have reported outcomes with its usage, but primarily utilizing a direct anterior (DA) approach.13–15 To the author’s knowledge, there has been one study on the subject that combined anterior and posterior approach, but included only 15 cases in the posterior cohort. 16 Prior studies evaluating common cementless femoral stems report mixed results, with some studies reporting increased femoral component loosening and fracture when an anterior approach was utilized, 17 while others demonstrate no difference in fracture rates or loosening based on approach.17,18 Additionally, studies have identified that rather than approach, the femoral stem type is a risk factor for increased fracture risk.19,20 There have been no large, longer-term follow-up studies reporting the clinical and radiographic results associated with the ACTIS stem implanted through a posterior hip approach.
Automated broaching (AB) delivers single or continuous impacts at a consistent energy, direction, and vector during femoral preparation, eliminating the use of a mallet for femoral preparation.21,22 Outcomes in patients who underwent femoral AB versus manual broaching (MB) in THA have been discrepant, with increased final femoral size in the AB groups and fracture rate consistent with the literature on cementless stems.16,23 AB has received increased attention recently given its theorized benefits of decreasing the number of off-center strikes during broaching and the surgeon’s physical burden that is associated with swinging a 3- to 5-lb mallet nearly 300 times per operative day.24–27 Surgeon adoption of AB has been mitigated by concerns regarding a potential higher rate of periprosthetic femur fractures and unnoticed cortical perforation. 21
The purpose of our current investigation was to report the clinical and radiographic outcomes of the ACTIS stem implanted with AB via a posterior approach in THA. A secondary goal was to investigate the presence of a “learning curve” of both AB and ACTIS usage.
Methods
Institution Review Board (IRB) approval was obtained at our institution prior to initiation of this study. All patients who underwent primary THA by a single fellowship trained surgeon (RMN) were retrospectively identified from January 1st, 2018 to June 1st, 2023. All patients underwent a minimally invasive THA using an approximately 6.0 cm incision via a mini-posterior approach (6-7 cm skin incision) as previously described. 28 All femoral canals were prepared using the KINCISE (Depuy Synthes, Warsaw IN, USA) automated broaching and impaction system. This automated broaching system was used for femoral broaching and final femoral implant impaction, it was not used on the acetabular component. Patients were included if they received an ACTIS femoral stem implant at the time of index surgery. Demographic, radiographic, and patient-reported outcome measure data were collected. Age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) score, laterality, diagnosis, preoperative and postoperative patient-reported outcomes measurement information system (PROMIS) scores, postoperative complications, revision surgery, and length of postoperative follow-up were obtained from chart review. Postoperative complications were divided into medical complications requiring readmission within 90 days of the index surgery, and surgical complications, including periprosthetic fractures, dislocations, prosthetic joint infections, superficial wound dehiscence, and “other” at any time point post-operatively. Surgical complications denoted as “other” included aseptic loosening, symptomatic psoas tendon irritation, seroma, and sciatic nerve palsy. Patients requiring any return to the operating room as well as those requiring revision of components were noted. Acetabular cup type and intra-operative complications were obtained from the patient’s operative note. Dorr classification, canal width, cortical width, and resultant femoral cortical index were all obtained from every patient’s preoperative standardized AP radiograph to characterize proximal femoral anatomy. Subsidence was calculated by subtracting the distance of the proximal femoral stem to the tip of the greater trochanter at the latest postoperative follow-up AP radiograph from the distance measured on the earliest postoperative radiograph. 29 Radiographs were analyzed for the presence of any lucent lines around the femoral stems on sequential postoperative radiographs. 30 The length of postoperative follow-up at the time of latest radiograph used to measure subsidence was recorded. The distance the medial collar of the ACTIS stem sat up in millimeters was measured from the neck cut.
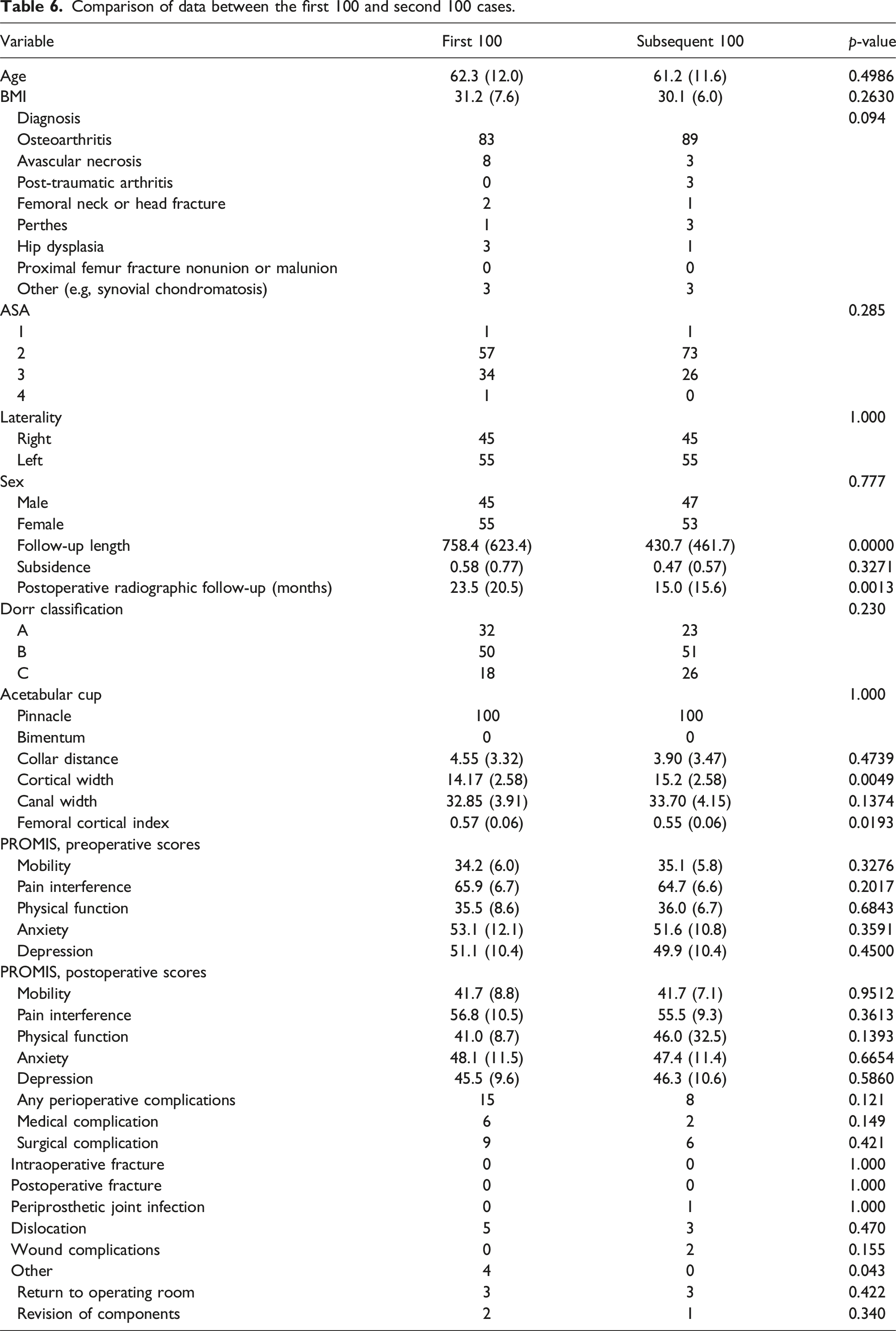
“Learning curve” was assessed by comparison of frequency and type of complication between the first 100 and subsequent 100 THAs. Additional comparison tests were performed between the first half (n = 498) and subsequent half (n = 523) of the cohort.
Statistical analysis was performed using the STATA version 17.1 (StataCorp, College Station, Texas, USA). Categorical variables were compared using chi-square analysis. Continuous variables were compared via the t test. Data was then compared between patients who have no subsidence versus patients who have any subsidence. Correlation data was obtained, and Pearson’s correlation coefficients were reported. Radiographs were analyzed by three orthopaedic surgery residents in their third or fourth year of training (RRA, HFB, MTS) and validated by a senior author (RMN).
Results
Demographic, radiographic, and PROMIS data for all patients.

Comparison of data between the first half and second half of cohort cases.

Categorization of intraoperative and postoperative complications.

Comparison of data between cases with any subsidence versus no subsidence.

All patients experienced statistically significant improvement in their PROMIS scores postoperatively. Specifically, they experienced lower depression, anxiety, and pain interference. They reported higher physical function and mobility. All differences met thresholds exceeding previously established minimal clinically important differences. 31
There were seven (0.68%) intraoperative fractures. They were all calcar fractures, managed with cerclage wires around the proximal femoral canal. These were followed for an average of 303 days post-operatively and none required revision surgery or demonstrated significant postoperative subsidence >5 mm, a common threshold for clinically significant subsidence.32–34 There were 11 (1.08%) postoperative periprosthetic fractures. There were 4 B2 periprosthetic fractures identified within the first 2 weeks postoperatively. These underwent open reduction and revision of the femoral stem by the index surgeon (RMN). These did not demonstrate postoperative subsidence or require revision surgery beyond their index revision. There were three minimally displaced meta-diaphyseal B1 fractures noticed within the first month postoperatively that were treated non-operatively and went on to radiographic and clinical union without any impact on postoperative outcomes. These fractures were often noted after a patient had successfully had a period of full weight bearing without fracture displacement, and thus the surgeon felt comfortable treating these non-operatively. Three additional fractures were Vancouver A greater trochanteric fracture managed non-operatively; and the final was a Vancouver B1 fracture treated with open reduction and internal fixation at an outside hospital without stem revision. In total, seven post-operative fractures were noted within the first month after surgery. Given the possibility that these may reflect missed intra-operative fractures, conservatively this would bring the total to fourteen (1.37%) intraoperative fractures. Of the true intra-operative as well as potential missed intra-operative fractures, 11/14 were female, with a range of Dorr classifications, 5/14 with Dorr A bone, 6/14 Dorr B and 3/14 Dorr C.
Association of subsidence and other demographic or radiographic variables.

When comparing data between the first 498 and subsequent 523 cases, there were no difference in preoperative or postoperative PROMIS scores between groups as seen in Table 2. The latter cohort of cases demonstrated a slightly higher degree of radiographic subsidence (0.6 vs 0.4 mm, p = .06). The latter cohort also featured a higher frequency of Dorr A/B femurs with higher femoral cortical indices than present in the first half. The first 498 cases experienced a higher rate of perioperative complications (8.8% vs 5.4%, p = .03), and a higher rate of post-operative surgical complications (6.2% vs 3.3%, p = .025), largely owing to postoperative dislocations. Overall, 2.6% of patients experienced a medical complication, and 4.7% experienced a surgical complication including periprosthetic fractures, dislocation, prosthetic joint infection, wound dehiscence, or other related complications. A total of 1.86% of patients required return to the operating room for any reason, with 1.27% requiring revision of components for fracture, dislocation, or infection (Table 3). The attending surgeon switched from the use of a Pinnacle acetabular cup (DePuy Synthes, Warsaw IN, USA) to primarily the Bimentum dual mobility mono-block cup (DePuy Synthes, Warsaw IN, USA) at the transition period between groups to increase the effective head size to minimize dislocation risk, which may help explain the 12/498 (2.4%) dislocations in the first half versus 1/523 (0.2%) dislocations in the latter half. 28 The Pinnacle acetabular cup was used in 10 patients in the latter half to allow for screw fixation. Overall, there was no difference in the rate of intra-operative fracture in between groups (0.6% vs 0.7%, p = .75). More postoperative fractures were observed in the latter cohort of cases, though there was no concomitant increase in revision surgery for periprosthetic fracture. All identified fractures were on the femoral side.
Comparison of data between the first 100 and second 100 cases.
Discussion
This single-surgeon, consecutive series of 1021 posterior-approach THA with ACTIS stem and AB demonstrates low rates of intra-operative and postoperative complications. Our intra-operative and postoperative periprosthetic fracture rates were 0.68% and 1.07%, respectively. The all-cause revision rate was 1.8%. There were no cases of implant loosening at mid-term follow-up were identified. Additionally, since there was no difference in the frequency or type of complications between the first 100 and subsequent 100 cases, we did not identify a “learning curve” for AB.
While intraoperative and postoperative calcar fracture is a relatively common (0.1%–5.0%) and potentially devastating complication in THA, the rates identified in this study were low.19,35–37 Automated broaching has been introduced as an alternative to manual broaching in total hip arthroplasty. This carries the theoretical benefits of strikes with a consistent energy, vector and direction, limiting off center strikes and broach malalignment. 21 It has been shown to reduce operative time and could reduce physician work-related injuries due to the repetitive stress of malleting. 23 The major concern with the advent of automated broaching remains the risk of intra-operative fracture. 38 A recent study by Strait et al reported no significant difference in incidence of calcar fractures and between cases performed with MB versus AB among 2048 DA THAs. 38 In their study, they reported 12/1048 intra-operative calcar fractures (1.1%), 4/1048 (0.38%) postoperative-operative greater trochanteric fractures, three intra-operative cortical perforations (0.29%), and no postoperative acute periprosthetic fractures in their AB group for cementless THA. 38 The rate of calcar fractures was higher in their study than the present study, but their rate of postoperative fracture was lower. Similar to our study, they noted zero revisions for mechanical loosening. Additionally, Osondu et al reported a 1.2% intra-operative calcar fracture rate and a 0.4% postoperative periprosthetic fracture rate in AB with ACTIS among 1453 cases. 14 Again, while the rate of intraoperative fracture is lower in the present study, our rate of postoperative fracture is higher, potentially suggesting missed intra-operative non-displaced fractures. Prior literature classifies early post-operative fractures as a post-operative and not intra-operative fracture. 39 However, if all early post-operative fractures in this study were assumed to be true intra-operative fractures, our rates of intra-op fractures (1.37%) and post-operative fractures (0.20%) would align with prior literature on automated broaching, and continue to have intra-operative fracture rates similar to those utilizing manual broaching.35–37 The rate of combined intra and postoperative rates is similar between our studies. While surgical approach has often been studied in association with fracture rate, prior studies have also emphasized that stem geometry, such as with taper wedge stems, is an independent risk factor for fracture rate. 20 Our study adds to the existing literature by reporting these rates in AB for ACTIS with a posterior approach, while prior literature focuses predominantly on the anterior approach, with only one single study discussing 15 posterior approach THAs. 16
Our experience with ACTIS stem has been positive with respect to short and mid-term surgical outcomes. Significant improvement in postoperative PROMIS scores, low rates of subsidence, and no cases of mechanical loosening were key findings in our study. Further, the high rate of survivorship among patients who have all types of femoral cortical anatomy and demographics supports its use in most primary THA, regardless of surgical approach. Bornes et al reported a 4.4% all-cause revision rate of the Zimmer M/L single-taper femoral stem (Warsaw, IN) in 502 cases over 4 years that excluded any Dorr C femora. 40 This included 2 cases that demonstrated subsidence >5 mm that were revised for mechanical loosening and/or instability. Additionally, they reported statistically significant correlations between presence of any subsidence and elevated BMI >25, older age, and incidence of revision surgery. Conversely, we found no association of subsidence with BMI, age, or Dorr C femora in our study using the ACTIS stem, although it is possible this association exists, and our study may not be powered to detect it. Kaszuba et al demonstrated via a short-term, retrospective study of 330 THAs with Corail and ACTIS stems at a 1-year minimum follow-up that the ACTIS stem had low rates of stress shielding, cortical hypertrophy, and calcar atrophy. 41 Only one patient in that cohort had subsidence ≥ 2 mm, and no patients underwent revision surgery for any reason.
This investigation adds to the existing literature that automated broaching systems can be safely integrated into the surgical workflow of a busy arthroplasty practice, even amongst surgeons with no previous experience utilizing this technology. Given we did not find a difference in outcome between the first 100 and subsequent 100 cases, we did not identify a “learning curve” for this technology.
The limitations of our study are its retrospective nature, lack of a control group with manual broaching, low rate of adequate postoperative imaging available for subsidence analysis despite excellent follow-up rates, heterogeneity with mixed acetabular implants, and single surgeon design which may limit generalizability. Additionally, fractures that were identified within the first month post-operatively were reported as post-operative fractures but may have been missed intra-operative fractures. 39 The theoretical adjusted percentages if these were assumed to be intra-operative fractures have been reported in the results section.
Conclusion
This large, consecutive, single-surgeon series demonstrates excellent results of a medial collared, triple tapered, cementless stem prepared and impacted with an automated broaching system. At mid-term follow-up, there were no revisions for mechanical loosening and there was an all-cause survivorship of 98.2%. Automated broaching is a safe alternative to manual broaching; however a randomized control trial would be beneficial on this topic.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors has received research support from DePuy and Stryker. One of the other authors has received intellectual property royalties from DePuy and Smith and Nephew, has received consultant payment from DePuy, Ethicon, Medtronic, Mirus, Rom Tech, Smith and Nephew, has received research support from Stryker, Zimmer, and Smith and Nephew, has stock/stock options in Rom Tech, and has worked as a Board member/committee member of American Association of Hip and Knee Surgeons and the Southern Orthopaedic Association.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.