
Abstract
Purpose:
Cementless modular fluted hip stems are commonly used in revision arthroplasty. Nevertheless, there is a wide spectrum of recommendations concerning the minimum bone stock required to enable osseous ingrowth and implant–bone micromotions <100 µm. This experimental study investigated the primary stability of a tapered cementless fluted revision stem depending on different types of bone defects.
Methods:
Implant–bone interface movements with a bimodular stem were examined under cyclic axial and torsional loading using composite femora. In four degrees of freedom, the implant subsidence and micromotions were captured with linear variable differential transformers for the intact femora and seven different defects ranging from Paprosky type I to type IIIB.
Results:
With a 7-cm length of intact diaphysis proximal to the isthmus (Paprosky IIIA), mean implant–bone micromotions of 66 µm occurred. An implant–bone contact zone of only 5 cm (Paprosky IIIA) resulted in micromotions notably over 100 µm and significantly increased subsidence (p < 0.05). With a Paprosky IIIB defect (3 cm of intact diaphysis) rotational instability occurred in all specimens.
Conclusions:
Aside from critically increased interfacial micromotions (>100 µm), rotational instability emerged as a mechanism of fixation failure when the implant–bone contact zone was only 5 cm or less. Hence, future studies investigating the implant fixation in the case of femoral bone defects should consider both axial and torsional loading. With regard to the clinical application, our data suggest maintaining 7 cm of diaphyseal implant–bone contact for a safe anchorage of cementless fluted hip revision stems.
Introduction
Uncemented revision stems with a tapered fluted design have become an established solution for complex hip arthroplasty revision cases with large bone defects. 1 –3 Clinical studies with monoblock or modular cementless fluted stems revealed a stem survivorship of 91.7–97.6% after a mean follow-up of 8–15.8 years. 4 –10 Nevertheless, clinical data indicated a worse outcome with increasing sizes of femoral bone defects. 1,7,10
Insufficient primary stability and excess interfacial movements between the implant and the bone are known to inhibit adequate osseous integration of the implant. Based on studies with animals and human osteoblasts, relative implant–bone micromotions below 100 µm seem to be a prerequisite for osseous implant integration. 11 –13
Although primary stability is an essential point when using uncemented revision stems, the recommendations concerning the necessary minimum lengths of sufficient implant–bone anchorage differ widely, ranging from 2 cm, 14 3–4 cm, 15,16 4–6 cm, 4 and about 7 cm or 2 femoral diameters 5,17,18 up to 8–12 cm. 19 Previous experimental studies addressing this issue often focused on specific single aspect such as axial or rotational stability and smaller bone defects. 20 –23
The first aim of the present study, therefore, was to measure the interfacial micromotion and subsidence of modular tapered revision stems under dynamic loading conditions, using composite femora and linear variable differential transformers (LVDTs). The second aim was to investigate the relative interface movements between the implant and the bone with seven different types of bone defects (Paprosky I to Paprosky IIIB). It was hypothesized that it would be possible to identify the requisite minimum value of diaphyseal bone support to avoid instability of the implant or critical interfacial micromotion.
Materials and methods
Bone model and defect types
Fourth-generation left composite femora (n = 5, type 3406, Pacific Research Labs, Sawbones Europe AB, Malmö, Sweden) were used for this investigation, corresponding to other studies. 24 –27 Reproducible orientation and embedding of the specimens were ensured by using the manufacturer’s standardized transcondylar and femoral neck drill holes as well as the femoral isthmus as reference marks. Measurements were taken starting with the intact femora (“defect type 0”) and, subsequently, after the infliction of seven defined defects (Figure 1). The wedge-shaped defects were located at the anterior cortex extending from the neck resection line to the height of the lesser trochanter (defect 1) respectively 70 mm (defect 2) and 140 mm (defect 3) inferior to the lesser trochanter (Figure 1). Inter-specimens reproducibility of the different defects was ensured by using templates (one per defect) made from casting tape (Scotchcast™ Plus, 3M Health Care, St Paul, MN, USA). Subsequently, the femoral defect was enlarged using an electronic multi-tool cutter with a diamond disk (Dremel®, Robert Bosch Power Tools GmbH, Leinfelden, Germany).

Femoral defects types: intact femur (“0”) and wedge-shaped defects (“1–3”). Complete resection inferior to the minor trochanter (“4”) and with 7 cm (“5”), 5 cm (“6”), and 3 cm (“7”) of intact diaphysis above the isthmus (solid line).
Implants
A two-part modular cementless revision system (Restoration® Modular; Stryker Orthopaedics, Mahwah, NJ, USA) consisting of a proximal cone body and a tapered fluted stem based on a titanium alloy (Ti-6Al-4V) was used for this study (Figure 2). Specimen preparation and implants insertion were performed with the original instruments according to the manufacturer’s protocol by an orthopedic surgeon familiar with this implant (ME). Adequate press-fit and distal conical fixation were verified with an image intensifier. All femur specimens received implants of identical sizes, combining a bowed stem (length 235 mm, diameter 16 mm), implant body (length + 0 mm, diameter 21 mm), and a 32-mm metallic head (length + 0 mm, V40 cone).
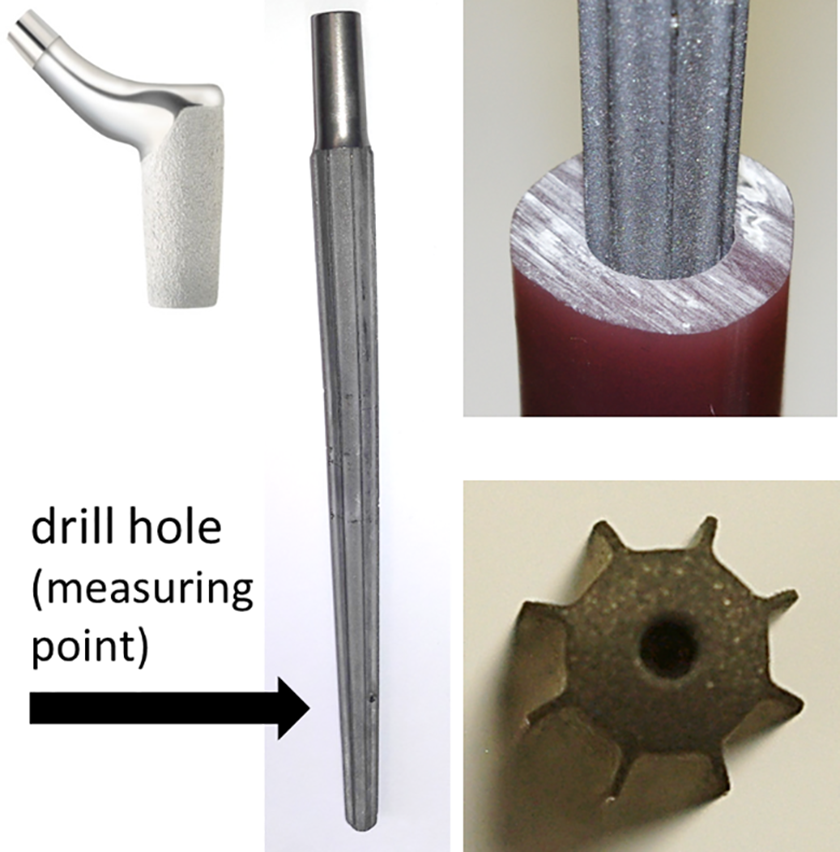
Left side: Bimodular cementless hip revision system with a grit-blasted conical fluted stem and hydroxyapatite-coated body. Drill hole for the fixation of one part of the measuring device. Right side: Implant at the height of a diaphyseal defect and view of the tip of the stem showing the flutes.
Test setup, measuring device, and loading protocol
The load regimen was based on the data published by Bergmann et al. 28 These data acquired by the means of total hip endoprostheses with internal force sensors are also provided by a free public database named OrthoLoad. To apply a resultant hip force in one direction as it occurs during the heel strike maximum of the gait cycle, femora were mounted in 15° adduction and 31° posterior rotation. A biaxially adjustable mounting device and a cylindrical stainless steel pot facilitated an exact and reproducible positioning of the specimens (Figure 3). A single sinusoidal axial load (frequency 1 Hz, minimum 100 N, maximum 1 kN) was applied with a servo-hydraulic testing machine (Instron 8842, Instron GmbH, Pfungstadt, Germany). Relative movements between the implant and the bone were recorded via an 8.0 mm single cortical drilling 3 cm below the isthmus at the posterior aspect of the femur specimen (Figure 3). Through this cortical drill hole, a 2 mm internal thread was milled into the revision stem after insertion. Finally, a metal cuboid was rigidly fixed to the implant by a threaded rod (Figure 3). Four LVDTs (DP/5/S, 1 µm resolution, Solartron Metrology, Meerbusch, Germany) were used to capture micromotions (reversible interfacial motions) as well as implant subsidence of one rotational (around the femoral shaft axis) and all three translational degrees of freedom (Figure 3). A program based on LabVIEW 2011 (National Instruments Germany GmbH, Munich, Germany) was developed to record and store LVDT position data. The micromotion magnitude was calculated based on the amplitude information derived from the envelope curves of the four LVDTs. For each type of femoral defect, the trial procedure started with 1000 load cycles of preconditioning for implant seating. The subsequent 500 load cycles served to acquire the data for further evaluation. Micromotion and subsidence measurements were taken for the first (cycles 0–20), middle (cycles 240–260), and last (cycles 480–500) 20 cycles to limit the amount of data. Micromotions were calculated based on the mean of these 60 cycles for all composite femora. Subsidence data were cumulated over the entire 500 load cycles.

Test rig (left) and fixation device for the LVDTs consisting of a stainless steel mount clamped to the femoral cortex (right). The implant motion was captured employing a metal cuboid rigidly fixed to the implant by a threaded rod. LVDT: linear variable differential transformers.
Statistics
The statistical evaluation included n = 5 specimens with defect types 0–5 and n = 4 specimens with defect type 6. The distribution of the data was tested using the Kolmogorov–Smirnov test. Since the data showed no normal distribution, the nonparametric Kruskal–Wallis test was used to check the micromotion and subsidence readings with the different defects for potential statistical differences. Further, a comparison of measurement data was performed separately for each spatial direction (translational and rotational motions) and all defect types (pairwise). The values of p ≤ 0.05 were considered significant. Data were stored on MS Excel (Microsoft Corporation, Redmond, WA, USA) and analyzed using the statistical package SPSS 21.0 (SPSS, Chicago, IL, USA).
Results
All n = 5 specimens completed the test series for the intact femora and defect types 1–5. With defect type 6, one Restoration Modular stem in specimen 1 showed continuous stem rotation with subsidence exceeding the measuring range of the setup (3 mm). Hence, the measurement series could not be completed with specimen 1, leaving n = 4 specimens in that group. With only 3 cm of conical anchorage (defect 7, Paprosky IIIB), a loss of rotational implant stability occurred in all specimens. Relative translational movements between the implant and the composite femur were captured in medial–lateral (x-axis), anterior–posterior (y-axis), and inferior–superior (z-axis) directions (Figure 3). Rotational movements around the femoral shaft axis (z-axis) were acquired. The vector sum was calculated from translational relative movements in the x-, y-, and z-directions.
Measurement of micromotions
Intact femur
The mean vector sum of interfacial micromotions in the intact femora (defect 0) was 90 µm (Table 1, Figure 4).
Measurement results (mean ± 1 SD) for the micromotion vector sum (mm (vsum)), translational micromotions (mm_t (x), mm_t (y), mm_t (z)), and rotatory micromotions around the z-axis in the horizontal plane (mm_r (z)).a
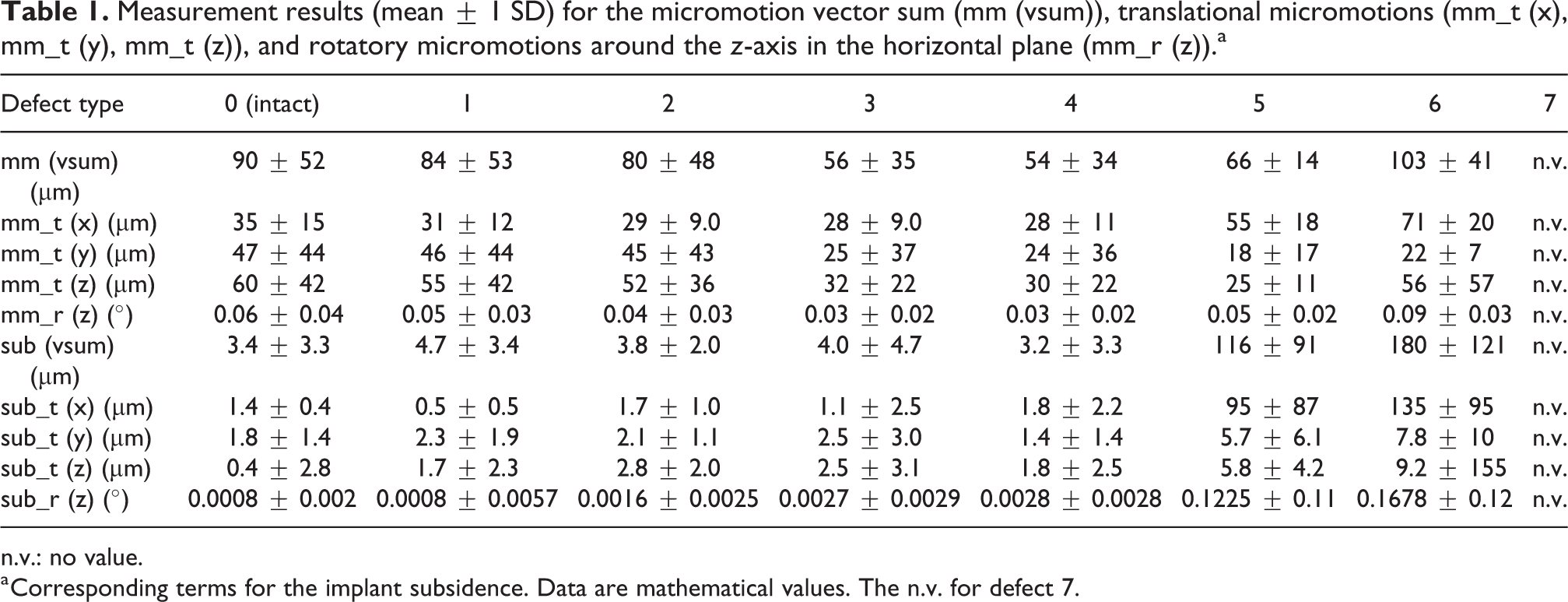
n.v.: no value.
a Corresponding terms for the implant subsidence. Data are mathematical values. The n.v. for defect 7.

Boxplot for the vector sums of the micromotion (μm) of all composite femora. Box corresponds to the IQR with mark for the median. Min–max whiskers; points for extreme outliers (threefold IQR). IQR: interquartile range.
Defects
In defect types 1–5, the micromotions vector sums remained well below 100 µm. Reduction of the implant–bone contact zone to 5 cm (defect 6) and 3 cm (defect 7) caused a marked increase of micromotions (Table 1, Figure 5). The micromotion vector sums obtained with defects 3 and 4 were lower than with the intact composite femora (Table 2). The pairwise analysis of the vector sums revealed significantly higher micromotions with defect 6 when compared to defects 3, 4, and 5 (Table 3). Translational micromotions in the x-direction with defect types 5 and 6 (Paprosky IIIA) were significantly higher than those obtained for the smaller defect types 1–4 (p < 0.001) (Figure 5). Reducing the diaphyseal anchorage within the Paprosky IIIA group from 7 cm (defect 5) to 5 cm (defect 6) resulted in a significant increase in micromotions in the x-direction (p = 0.032) and rotational micromotions (p = 0.004).

Boxplot for the micromotion (μm) in the x-direction for all composite femora. Box corresponds to the IQR with median marker. Min–max whiskers; points for extreme outliers (threefold IQR). IQR: interquartile range.
p Values from the pairwise analysis of the micromotion vector sums.a

n.v.: no value.
a The n.v. for defect 7 due to rotational instability of all test specimens.
b p < 0.05: significant difference.
p Values from the pairwise analysis of the subsidence vector sums.a
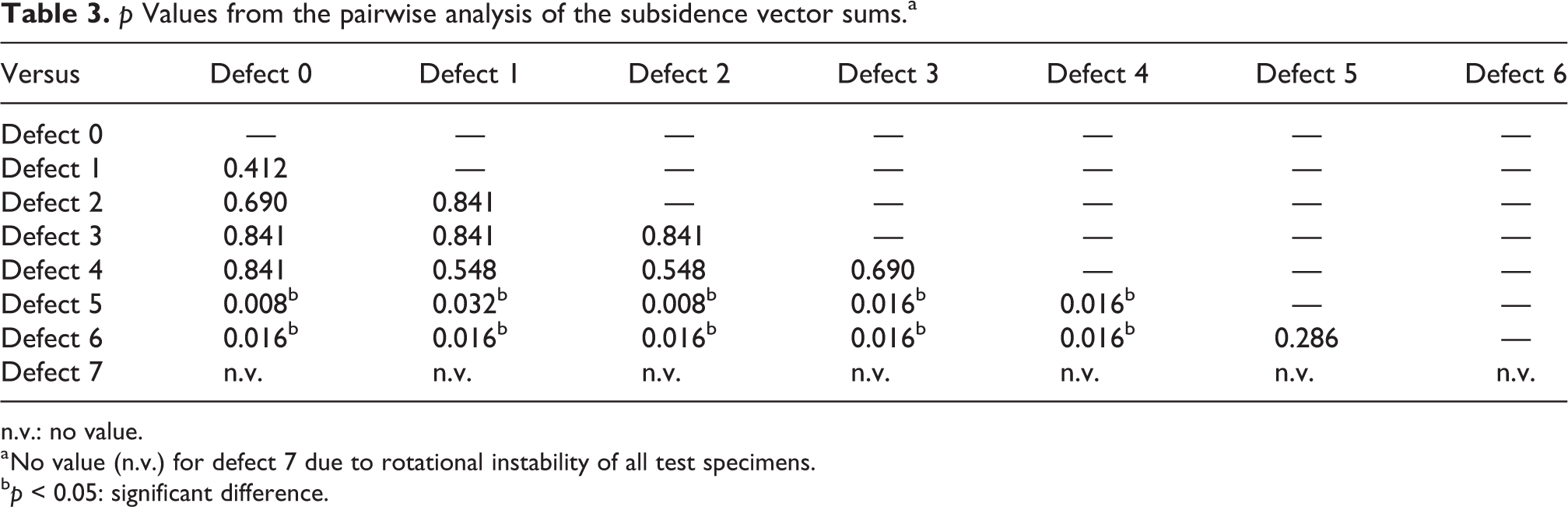
n.v.: no value.
a No value (n.v.) for defect 7 due to rotational instability of all test specimens.
b p < 0.05: significant difference.
Measurement of subsidence
Intact femur
The mean vector sum of implant subsidence in the intact femora (defect 0) was 3.4 µm/500 cycles (Table 1, Figure 6). Rotational subsidence was insignificant averaging 0.0008°/500 load cycles.

Boxplot for the vector sums of the subsidence (μm) of all composite femora. Box corresponds to the IQR with mark for the median. Min–max whiskers; points for extreme outliers (threefold IQR). IQR: interquartile range.
Defects
The subsidence vector sums with small defects (types 1–4) were less than 5 µm/500 load cycles and did not differ significantly (Table 1). With regard to the direction of translational implant subsidence in defects 1–4, none of the directions x, y, or z was clearly dominant (Table 1). Progressive resection of the proximal femur increased the subsidence vector sum and rotational subsidence, with consecutive translational subsidence in the x-direction being the main component (Table 1).
The pairwise statistical analysis showed no difference of implant subsidence between the intact femur and defects 1–4. Only with defects 5 and 6, the rotatory subsidence and translational subsidence (x-direction) were significantly higher (p ≤ 0.016) compared to the intact femur and smaller defects (types 1–4).
Discussion
As a result of our present study, rotational relative motion between the implant and the bone stock was the most remarkable degree of freedom. Micromotions and subsidence in the x-direction resulting from the rotation around the femoral shaft axis increased significantly with growing size of femoral defects. Diaphyseal anchorage of 7 cm turned out to be the minimum bone stock to warrant safe fixation of the revision stem for all specimens.
Jakubowitz et al. 20 and Kinkel et al. 21 investigated the primary torsional stability of revision endoprostheses under dynamic testing only with torsional loading (±7 Nm), recording the relative rotational movement of the implant. With a conical bimodular stem (MRP® stem, Peter Brehm GmbH, Weisendorf, Germany) 10 cm of intact diaphysis in composite femora 20 and about 8 cm stem anchorage in cadaver femora 21 were rated to be sufficient for a safe stem fixation. Kirk et al. employed a cadaveric bone loss model with peak loads of 750 N (axial loading) and 11 Nm (torsional loading). 29 The authors reported a sufficient primary fixation of conical fluted stems (Link® MP™ Hip Stem; Link America, Pine Brook, NJ, USA) with 10 cm of diaphyseal bone stock. The loading scenarios differed from our present study, and the influence of larger defects was not investigated. 20,21,29 Nevertheless, these experimental findings support that 8–10 cm of diaphyseal anchorage allows a safe fixation of cementless fluted revision stems. 20,21,29
Another notable finding of our present study was that diaphyseal anchorage of 7 cm (in case of Paprosky IIIA defect) also was sufficient to keep the interfacial micromotion vector sums below the critical limit (<100 µm) for bone ingrowth of the implant. 11 –13
Vanhegan et al. confirmed that a Restoration Modular stem achieves safe anchorage in Paprosky III defects. 22 Under dynamic axial load incrementing from 750 N to 1500 N, the authors found an overall axial stem subsidence of 167 µm and interfacial micromotions <150 µm for all loading conditions. 22 Vanhegan et al. applied higher axial loads than those used in our present study, but disregarded any torsional loading as it occurs in vivo. Hence, the described mechanism of failure was axial subsidence. 22 In our present study, implant rotation emerged to be the limiting factor. With view to these findings, the consideration of a combined torsional and axial loading is encouraged for experimental investigations on the primary stability of revision hip stems.
An unexpected finding of our study was that micromotion vector sums in midsize defects (types 3 and 4) were lower than with the intact femur and small defects (types 1 and 2). However, this effect was not observed for the subsidence data, which were consistently low for the intact femur and defects 1–4. Based on clinical experience and the manufacturer’s recommendations, a 235 mm distal stem is unnecessarily long for an intact femur or small proximal bone defects. 30 This may cause incalculable tension of the kinked revision stem in the medullary canal even after thorough reaming. Together with the position of our measuring point distally to the conical stem fixation zone, this could favor measurement of unexpected micromotions with the intact femur and small defects. Hence, with respect to primary to stability, small defects (Paprosky 0 and I) can be considered negligible in experimental studies with long fluted revision hip stems in the future.
Nevertheless, with growing size of defects our micromotion measurements clearly indicated that a certain minimum distance is required for a safe conical fixation. A reduction of the stem fixation zone from 7 cm to only 5 cm resulted in a 56% increase of the micromotion vector sum. The importance of a circumferential conical anchorage is confirmed by experimental and clinical data. 15,31 Heinecke et al. investigated the migration of cementless fluted stems under dynamic loading condition employing synthetic femora. 31 A better implant–bone contact was clearly correlated with less absolute stem migration. 31 Fink et al. reviewed 202 hip arthroplasty revisions via transfemoral or endofemoral approach using conical curved revision stems. 15 Endofemoral revisions resulting in a rather three-point fixation than conical fixation were found to have an over 50% higher rate of radiological signs for stem subsidence. 15 Hence, the quality and type of stem fixation should also be considered for in vitro investigations.
The limitations of our study arise from the loading configuration, which represents a simplification of the in vivo situation. Nevertheless, cyclic loading with a maximum of 1 kN corresponded to in vivo data when walking is supported with crutches in both hands (assumed body weight 80 kg) as given by OrthoLoad and Bergmann et al. 28 Moreover, the application of a rotational moment resulting from the axial loading in combination with the position of the femora is a common practice for experimental studies. 31 Another limitation may be the use of composite femur models. However, their geometry and mechanical properties match those of human bones. 24,25 Composite bones were thoroughly tested and rated to be appropriate for comparative primary stability studies. 26,27 Manual stem impaction could contribute to inter-specimen variance of primary implant stability. Hence, the use of a hammer instrumented with a force sensor may be considered for the future. 33 Furthermore, our measuring point was located distally to the conical stem fixation zone. This could result in higher micromotions measured than if captured directly in the fixation zone. Hence, the recommended diaphyseal anchorage of 7 cm may be rather conservative. Finally, the sample size of n = 5 was chosen without prior statistical calculation, but it met the approach of other studies and the dimension for implant testing according to ISO and ASTM standards. 20,21,32
Conclusion
Critical interfacial micromotions and rotational instability emerged as mechanisms of failure of revision stems with increasing femoral defects. Based on our findings, at least 7 cm of diaphyseal implant–bone contact should be recommended when using the Restoration Modular hip stem. Further clinical validation with specific respect to Paprosky type IIIA and type IIIB defects is needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Association for Orthopaedic Research (AFOR) foundation. The AFOR did not influence the study design, collection, analysis and interpretation of data, writing of the report, and the decision to submit the article for publication. No further specific grant from funding agencies in the public, commercial, or not-for-profit sectors was received.