
Abstract
Purpose
The necessity of lesser trochanter (LT) fixation in unstable intertrochanteric fractures remains uncertain, particularly in cases with LT displacement between 5 and 10 mm. This study aimed to determine whether cerclage wire augmentation improves postoperative hip flexor strength, functional recovery, and fracture healing compared to standard cephalomedullary nail fixation alone.
Methods
A double-blinded, randomized controlled trial was conducted at a tertiary referral center, enrolling patients aged ≥60 years with unstable intertrochanteric fractures and LT displacement of 5–10 mm. Patients were randomly assigned to cephalomedullary nail alone (Group A) or cephalomedullary nail with cerclage wire fixation (Group B). The primary outcome was maximal isometric hip flexor strength at 1.5, 3, 6, and 12 months. Secondary outcomes included Barthel’s Index (BI), Harris Hip Score (HHS), Radiographic Union Score for Hip (RUSH), operative time, hospital stay, and complications. Statistical analyses included independent t-tests, chi-square tests, and linear mixed models.
Results
A total of 46 patients (23 per group) were analyzed. No significant differences were observed in hip flexor strength or functional outcomes. However, the cerclage wire group demonstrated significantly higher RUSH scores at 3, 6, and 12 months (p < .05), indicating enhanced fracture healing. Operative time was significantly longer in the cerclage wire group (p = .005). Two cases of cerclage wire breakage occurred, neither requiring reoperation.
Conclusion
LT fixation for 5–10 mm displacement did not improve hip flexor strength or functional recovery but significantly enhanced fracture healing. Given the increased operative time, LT fixation should be selectively considered in cases where accelerated fracture healing is a priority. Further research is warranted to assess long-term clinical outcomes.
Keywords
Introduction
Hip fractures are a growing global health concern, particularly among the elderly, with incidence expected to rise due to an aging population.1–3 These fractures, often caused by low-energy trauma in individuals with osteoporosis, lead to significant morbidity, loss of independence, and increased mortality. Many patients experience long-term mobility limitations, requiring assistive devices or caregiver support, and are at high risk for recurrent falls and secondary fractures.4,5
Intertrochanteric fractures account for nearly half of all hip fractures and are classified based on stability, with unstable variants frequently involving lesser trochanter (LT) displacement. 6 The LT contributes to proximal femoral stability and serves as the insertion site for the iliopsoas muscle, which aids in hip flexion and balance. While intramedullary fixation with cephalomedullary nail is the preferred treatment for unstable fractures, the necessity of LT fixation remains debated, as it is often not addressed in standard surgical procedures despite its potential role in load distribution and functional recovery.7,8
Studies have suggested that LT displacement can compromise fracture stability, leading to an increased risk of implant failure, varus collapse, and delayed union, particularly when the fracture extends to the posterior cortex or involves significant medial wall compromise.9–11 A systematic review found that complication rates ranged from 2.5% to 32.3% in the non-fixation group and concluded that LT displacement >2 cm warrants surgical. 12 Additionally, retrospective studies have indicated that LT displacement exceeding 1 cm is associated with higher postoperative pain and complication rates. 13 However, many surgeons globally do not routinely fix the LT and instead opt to use a long femoral nail when concerned about fracture stability and medial wall compromise.7,11
Biomechanical studies have suggested that fixation of the LT may enhance primary stability in intertrochanteric fractures, potentially preventing excessive varus collapse and improving load distribution. 14 However, clinical evidence remains limited. While some retrospective studies have reported positive functional outcomes following LT fixation, they lack control groups for direct comparisons. 15 Additionally, no high-quality randomized controlled trials (RCT) have evaluated whether LT fixation in the 5–10 mm displacement range improves surgical or functional outcomes, nor is there conclusive evidence on its effect on postoperative hip flexor strength, as compensatory mechanisms involving other hip flexor muscles may mitigate the impact of LT disruption.
This study aims to address this gap by evaluating the effects of cerclage wire augmentation in unstable intertrochanteric fractures with 5–10 mm LT displacement. We hypothesize that fixation of the LT using cerclage wire in combination with cephalomedullary nail will improve postoperative hip flexor strength, as measured by maximal isometric hip flexor strength at 12 months postoperatively.
Patients and methods
Study design and setting
This study was a double-blinded, randomized controlled trial conducted at a tertiary referral center. All participants and/or their legal guardians provided written informed consent before enrollment.
Participants
From March 2023 to March 2024, a total of 56 patients diagnosed with unstable intertrochanteric fractures involving the LT were screened for eligibility. The inclusion criteria were as follows: patients aged 60 years or older with good cognitive function and communication ability, those diagnosed with an unstable intertrochanteric fracture with LT displacement classified as AO/OTA 31A2.2, 31A2.3, or 31A3.3 without extension below the lesser trochanter; and those with LT displacement between 5 and 10 mm after closed reduction, with sufficient fragment size for cerclage wire application. Patients were required to be available for at least 12 months of follow-up.
Exclusion criteria included previous ipsilateral hip or femoral surgery, non-osteoporotic pathological fractures, multiple fractures, pre-existing bedridden status or walking disability, severe perioperative risk classified as American Society of Anesthesiologists (ASA) score IV or V, and refusal to participate.
Based on the eligibility criteria, five patients were excluded—two due to non-osteoporotic pathologic fractures, two with pre-existing impaired ambulation, and one with a history of previous ipsilateral hip surgery. A total of 51 patients were randomized into two groups: Group A (cephalomedullary nail without cerclage wire, n = 25) and Group B (cephalomedullary nail with cerclage wire, n = 26).
During follow-up, five patients were lost due to mortality. In Group A, two patients died—one from systemic complications during hospitalization and one within 3 months postoperatively. In Group B, three patients died—one during hospitalization and two within 3 months postoperatively. As a result, 46 patients completed the study and were included in the final analysis. (Figure 1) All analyses were conducted on an intention-to-treat basis, with 23 patients in each group analyzed as per their original assignment. CONSORT flow diagram depicting patient enrollment, randomization, allocation, follow-up, and analysis in this study. A total of 56 patients were assessed for eligibility, with five excluded due to non-osteoporotic pathologic fractures, pre-existing impaired ambulation, or prior ipsilateral hip surgery. The remaining 51 patients were randomized into two groups: Group A (cephalomedullary nail without cerclage wire, n = 25) and Group B (cephalomedullary nail with cerclage wire, n = 26). Follow-up losses included two patients in Group A and three in Group B due to postoperative mortality. Ultimately, 23 patients in each group were included in the final analysis.
All eligible patients who met the inclusion criteria agreed to participate in the study. This high participation rate may be attributed to the fact that the study was conducted in a tertiary referral center and an academic teaching hospital, where patients are generally accustomed to receiving treatment within a research-driven environment. Additionally, thorough pre-enrollment discussions were conducted to ensure that all participants fully understood the study objectives, potential risks, and benefits before providing informed consent.
Surgical techniques
A 2-g dose of intravenous cefazolin was administered preoperatively for antibiotic prophylaxis. All procedures were performed under general or spinal anesthesia by a single orthopedic trauma surgeon. Patients were positioned supine on a fractured table with the injured limb in traction, while the contralateral limb was placed in a hemilithotomy position to facilitate fluoroscopic imaging. Closed reduction was attempted using axial traction, adduction, and internal rotation. During closed reduction, real-time fluoroscopic assessment was performed to ensure that lesser trochanter displacement remained within the predefined 5–10 mm range. Patients whose post-reduction displacement exceeded this range would have been excluded; however, all included patients maintained displacement within this limit after reduction, likely due to strict preoperative screening and controlled reduction techniques performed by the experienced orthopedic trauma surgeon. If successful, and if LT displacement remained between 5 and 10 mm, patients were randomly assigned in a 1:1 ratio using computer-generated block randomization. The random allocation sequence was generated by an independent statistician using computer-generated block randomization in a 1:1 ratio. The allocation was concealed in sealed, opaque, sequentially numbered envelopes and was opened by the treating surgeon only after participant enrollment and confirmation of eligibility. The surgeon was aware of the allocation; however, both the patients and the evaluating physicians remained blinded to the treatment assignment.
A proximal lateral skin incision of approximately 4–10 cm was made, with length adjusted based on patient anatomy, fracture complexity, and the need for adequate reduction and implant placement. The entry point was confirmed fluoroscopically, and the proximal femur was reamed over a guide pin. A spiral blade was inserted into the center-center or center-inferior position to achieve an optimal tip-apex distance (TAD) of 5–10 mm. The distal locking screw was then placed to complete the fixation. Both groups underwent the same surgical procedure, with the only difference being the addition of cerclage wire fixation in Group B.
For patients in Group B, a mini-lateral incision was made to perform lesser trochanter fixation. The fascia lata was incised, and the vastus lateralis was bluntly dissected to expose the fracture site. A Hohmann retractor was used to assist in reduction, and the quality of reduction was confirmed under fluoroscopy. A cerclage wire was passed around the LT using a wire passer and tightened until the desired tension was achieved.
Postoperative management
Following surgery, patients were transferred to the orthopedic ward under the supervision of a multidisciplinary team, including physicians, nurses, and physical therapists. On postoperative day 1, patients received cold compression therapy, intermittent pneumatic compression for thromboprophylaxis, breathing exercises, and ankle pumping exercises. On postoperative day 2, patients commenced isometric hip exercises, range of motion (ROM) exercises, and upper limb strengthening. By postoperative day 3, patients were mobilized with a walker, and weight-bearing was encouraged as tolerated.
Patients were followed up at 1.5, 3, 6, and 12 months postoperatively for radiographic and functional evaluations. The evaluating physician was blinded to the treatment allocation.
Study outcomes
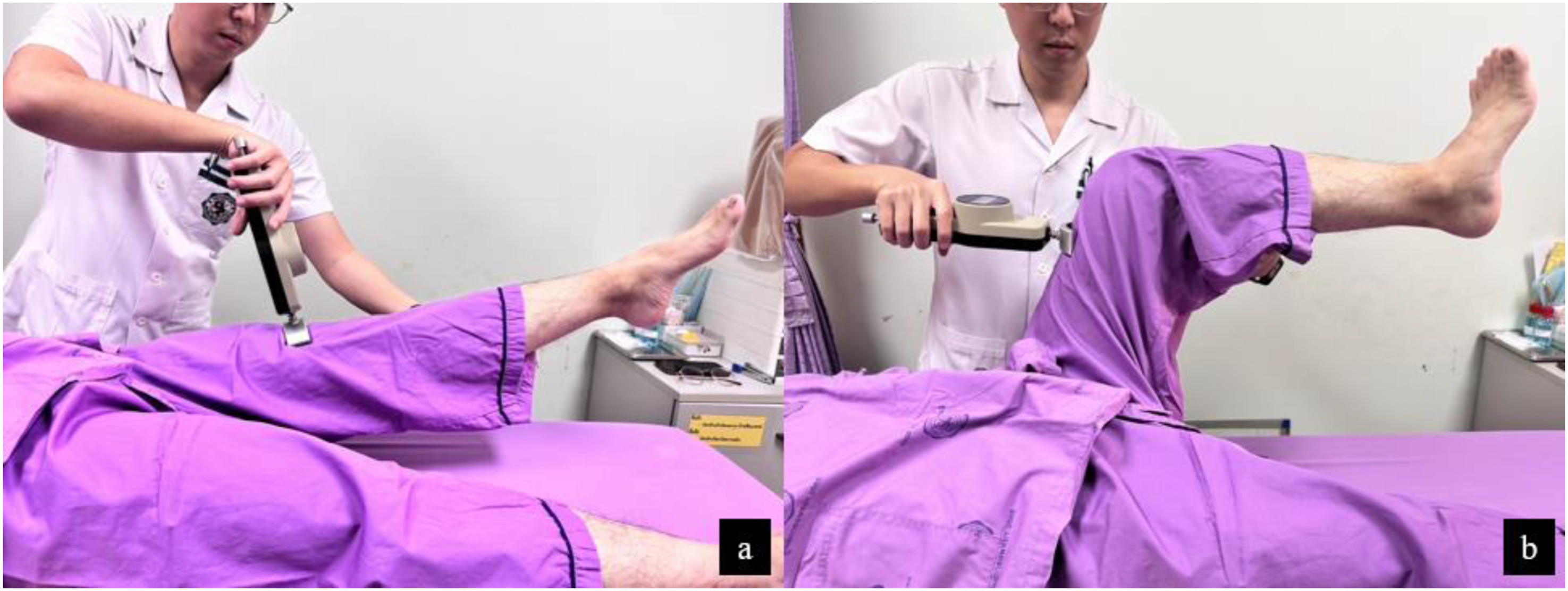
The primary outcome measure was maximal isometric hip flexor strength at 12 months postoperatively, assessed using a handheld dynamometer (Figure 2). Strength was measured in both neutral (0°) and 90° hip flexion positions (Figure 3) at 1.5, 3, 6, and 12 months postoperatively to evaluate recovery progression. The hip flexor strength deficit was calculated as the percentage difference between the non-affected side (XNA) and the affected side (XA), using the formula Handheld dynamometer used for measuring maximal isometric hip flexor muscle strength. Assessment of maximal isometric hip flexor muscle strength using a handheld dynamometer. (a) Measurement in a neutral (0°) hip flexion position. (b) Measurement in a 90° hip flexion position.
Secondary outcomes included functional outcomes assessed using Barthel’s Index (BI) and Harris Hip Score (HHS), fracture healing assessed using the Radiographic Union Score for Hip (RUSH)—which evaluated the healing of the intertrochanteric fracture as a whole, not the lesser trochanter fragment alone—and operative parameters, including surgical time, hospital length of stay, tip-apex distance (TAD), and neck shaft angle (NSA). Postoperative complications, including implant failure, varus malreduction, nonunion, screw cut-out, and wire breakage, were also recorded.
Statistical analysis
Sample size calculation was performed using STATA version 14.0, with a significance level of 0.05 and 80% power. Based on prior studies, 16 a minimum of 20 patients per group was required to detect a clinically meaningful difference of approximately 16 N in maximal isometric hip flexor strength, reflecting the largest observed strength difference between the operated and contralateral sides in patients with LT displacement. To account for a 10% dropout rate, a final sample size of 23 patients per group was determined.
Demographic and baseline characteristics were summarized as means and standard deviations for continuous variables and as frequencies for categorical variables. Between-group comparisons for continuous variables were conducted using independent t-tests, while categorical variables were compared using chi-square tests. Longitudinal outcome data, including hip flexor strength, BI, HHS, and RUSH, were analyzed using a linear mixed model to assess repeated measures over time. Analysis of covariance (ANCOVA) was used to control for baseline differences, with results reported as mean differences with 95% confidence intervals.
Results
Patient demographic data and clinical variables.

Data are presented as mean ± SD or n (%).
Primary outcome measures during the follow-up period for the two groups.
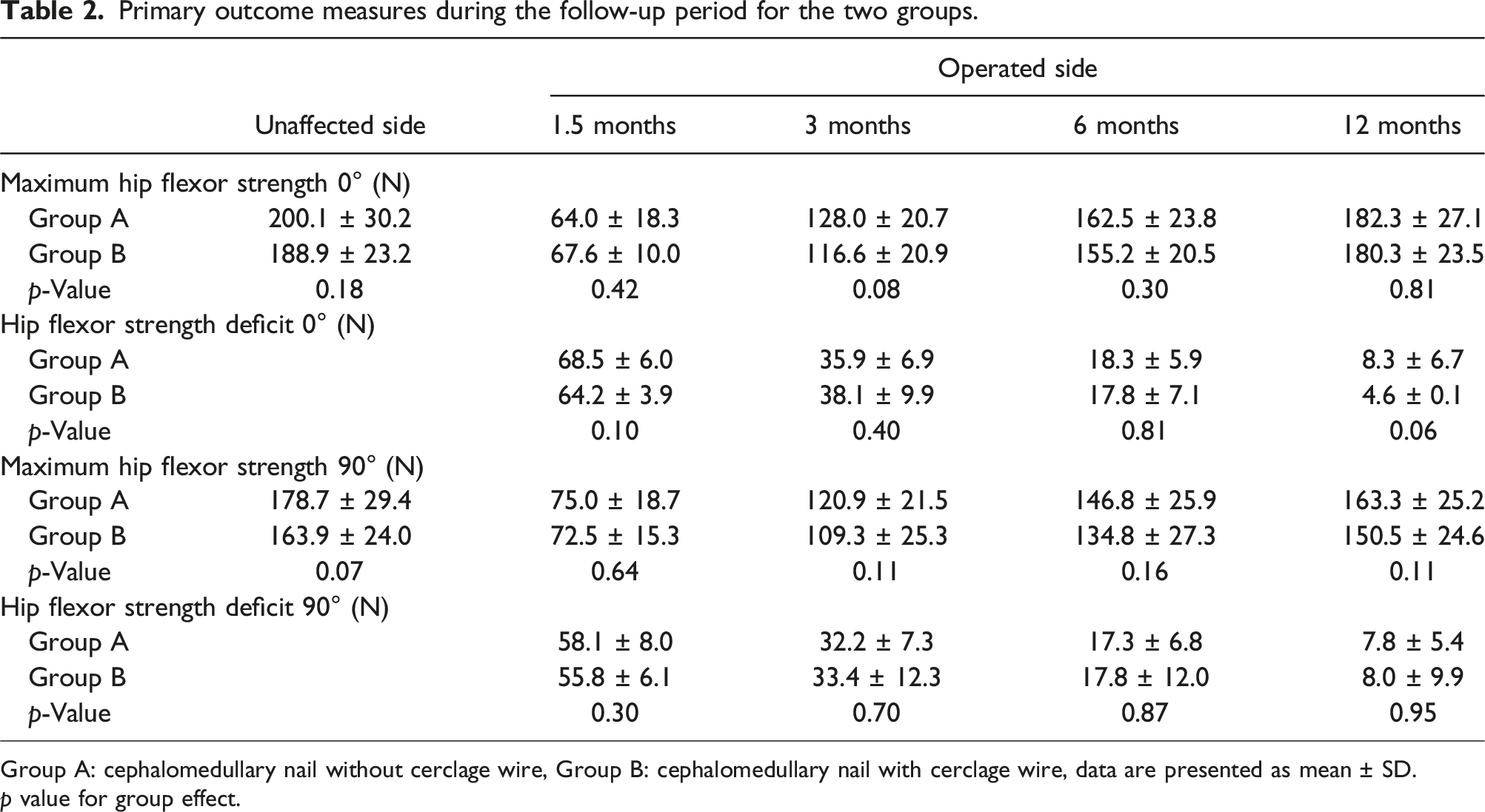
Group A: cephalomedullary nail without cerclage wire, Group B: cephalomedullary nail with cerclage wire, data are presented as mean ± SD.
p value for group effect.
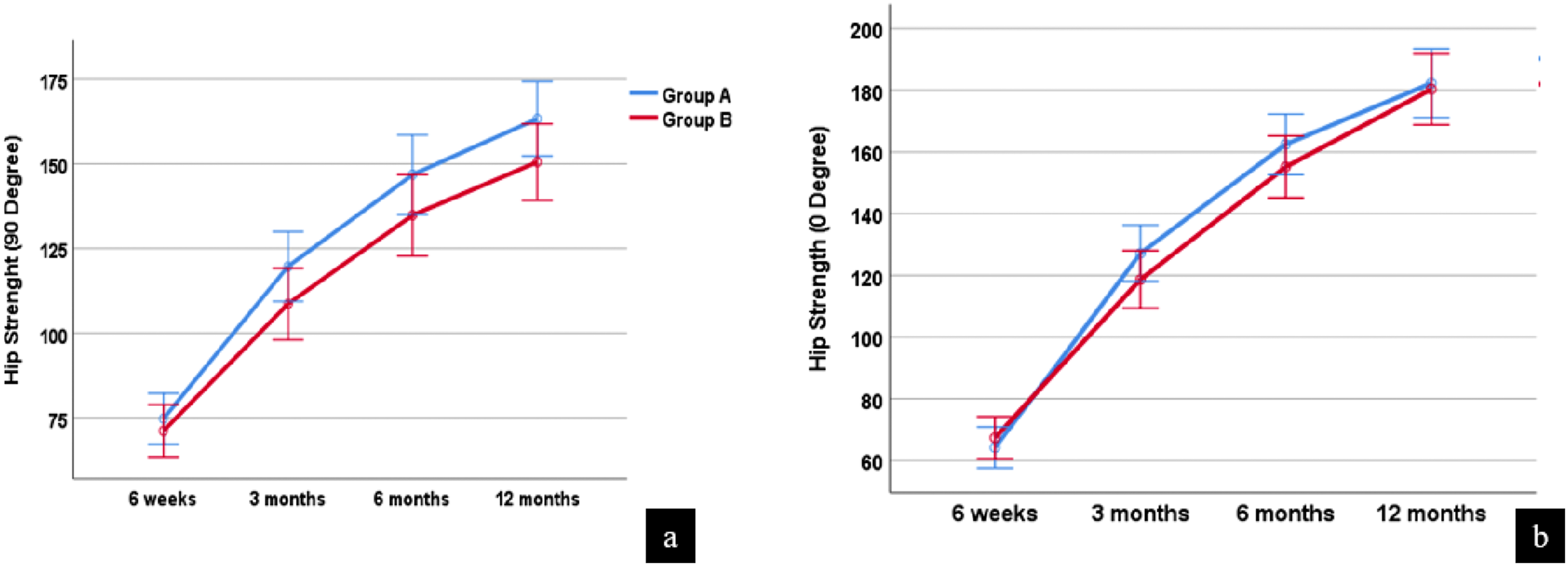
Comparison of maximal isometric hip flexor muscle strength (N) between the two groups at 6 weeks, 3 months, 6 months, and 12 months post-surgery. (a) Strength measurement in a 90° hip flexion position. (b) Strength measurement in a neutral (0°) hip flexion position. Error bars represent standard deviations. Group A (cephalomedullary nail without cerclage wire) is shown in blue, and Group B (cephalomedullary nail with cerclage wire) is shown in red.
Comparison of secondary outcome measures after operation between study groups.
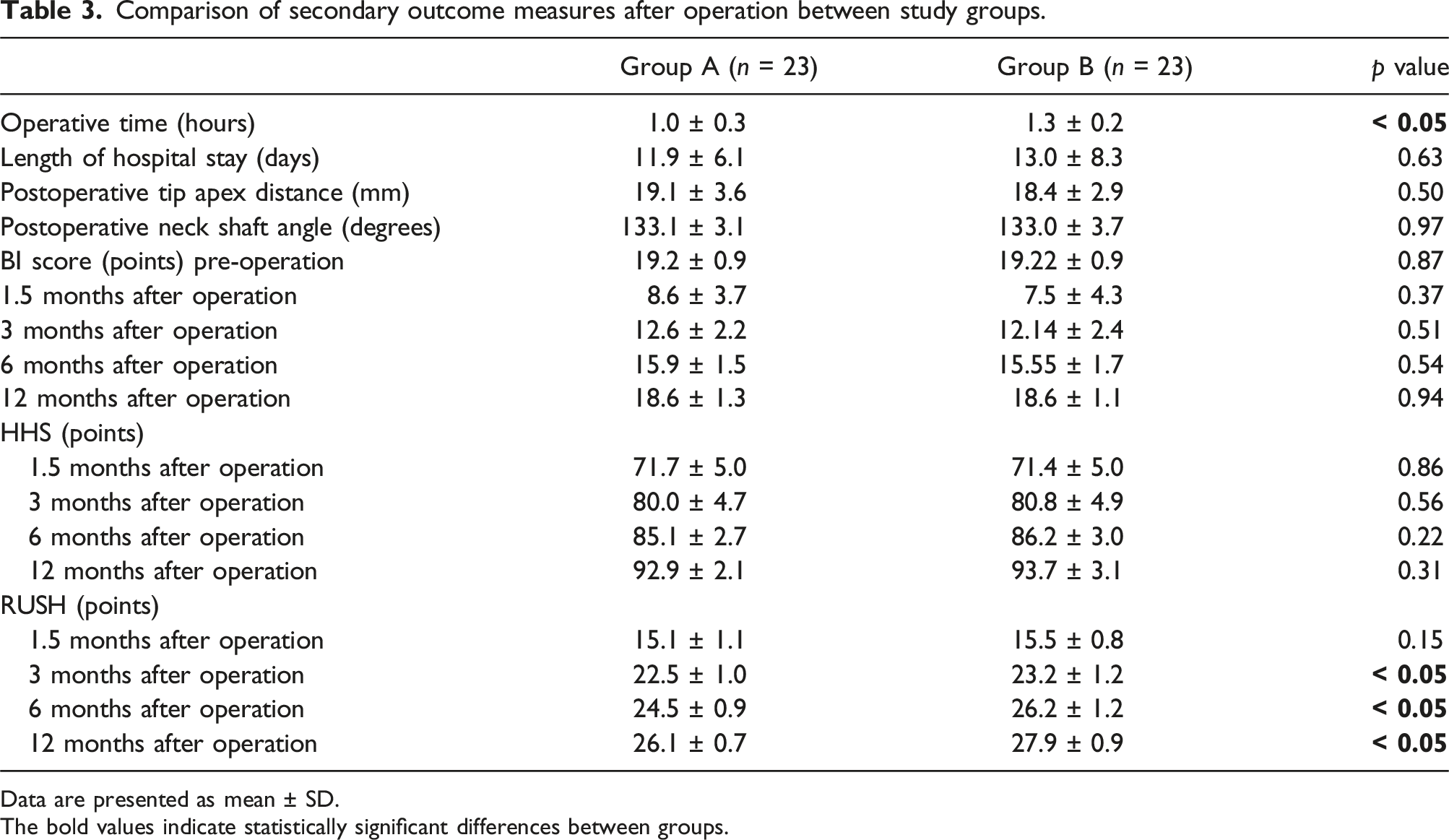
Data are presented as mean ± SD. The bold values indicate statistically significant differences between groups.
Analysis of functional and radiographic outcomes demonstrated no statistically significant differences in Barthel’s Index (BI) or Harris Hip Score (HHS) at any follow-up interval. However, the cephalomedullary nail with cerclage wire group exhibited significantly higher RUSH values at 3 months (p < .05), 6 months (p < .05), and 12 months (p < .05) postoperatively, indicating accelerated fracture healing in this group. These findings suggest that the addition of cerclage wire may facilitate earlier bone consolidation. Furthermore, trend analysis (Figure 5) demonstrated a continuous improvement in BI, HHS, and RUSH scores in both groups from 1.5 to 12 months, reflecting progressive recovery in daily activity capacity, hip joint function, and fracture healing. Comparison of postoperative recovery trends between the two groups at preoperative, 6 weeks, 3 months, 6 months, and 12 months post-surgery. (a) Barthel Index (BI) score, (b) Harris Hip Score (HHS), and (c) Radiographic Union Score for Hip (RUSH). Error bars represent standard deviations. Group A (cephalomedullary nail without cerclage wire) is shown in blue, and Group B (cephalomedullary nail with cerclage wire) is shown in red.
There were no cases of superficial or deep wound infections, varus malreduction, nonunion, screw cut-out, or implant failure in either group. Two cases of cerclage wire breakage occurred in the cephalomedullary nail with cerclage wire group (8.7%, 2/23), while none were observed in the cephalomedullary nail without cerclage wire group (0%, 0/23). However, neither case required reoperation. Early systemic complications were noted in both groups, with respiratory infections occurring in 13.0% (3/23) of patients in the cephalomedullary nail group and 17.4% (4/23) in the cerclage wire group (absolute risk difference: 4.4%, relative risk: 1.33). Urinary tract infections were reported in 21.7% (5/23) of patients in both groups. There was no significant difference in the overall incidence of systemic complications between the groups.
Discussion
This randomized controlled trial evaluated the impact of lesser trochanter fixation using cerclage wire compared to no fixation in unstable intertrochanteric fractures with LT displacement between 5 and 10 mm. The findings demonstrated no significant differences in hip flexor muscle strength, both in maximal strength and strength deficit, between the cephalomedullary nail with and without cerclage wire groups at all follow-up time points. Additionally, there were no significant differences in clinical and functional outcomes, including BI, HHS, length of hospital stay, postoperative neck shaft angle, or tip-apex distance. However, patients in the cephalomedullary nail with cerclage wire group exhibited significantly better RUSH scores at 3, 6, and 12 months postoperatively, indicating accelerated fracture healing compared to the non-fixation group. These findings suggest that while LT fixation may not provide functional advantages in terms of hip flexor strength recovery, it may promote earlier bone consolidation and could facilitate early weight-bearing and rehabilitation.
LT displacement in unstable intertrochanteric fractures has long been debated in terms of its impact on surgical and functional outcomes. Previous studies have suggested that displaced LT fragments may lead to impaired iliopsoas function, resulting in reduced hip flexion strength. Aprato et al. 17 reported a significant reduction in hip flexion force in patients with LT fractures, hypothesizing that shortening of the iliopsoas muscle due to LT displacement could impair its contractile function. Qi Sun et al..13 I further demonstrated that LT displacement exceeding 1 cm was associated with increased postoperative complications, including implant failure, varus malreduction, and nonunion.
Despite these concerns, the necessity of LT fixation remains unclear. While biomechanical studies9,14 have suggested that fixation may improve primary stability, clinical studies have yielded mixed results. A retrospective study involving 22 patients with displaced LT fragments treated with proximal intramedullary nailing and cerclage wiring reported favorable outcomes, with patients regaining pre-fracture hip function. 10 However, the study lacked a control group, limiting direct comparisons between fixation and non-fixation strategies.
Our study provides stronger evidence by employing a randomized controlled design. The lack of significant differences in hip flexor muscle strength between the two groups suggests that preserving iliopsoas muscle insertion through LT fixation may not be a critical factor in maintaining dynamic gait and balance in elderly patients with LT displacement of 5–10 mm. This aligns with previous studies 16 that reported no significant impact of LT integrity on surgical outcomes or hip function following intramedullary nail fixation for intertrochanteric fractures. Furthermore, a study examining 20 patients with pertrochanteric fractures and displaced LT found no significant reduction in hip flexion force, despite notable iliopsoas muscle atrophy, suggesting that compensatory mechanisms, such as recruitment of other hip flexors, may play a role in maintaining function. 18
While our study suggests that LT fixation does not improve functional outcomes, it was associated with a significantly longer operative time, highlighting the technical demands of the procedure. Given that elderly patients often have multiple comorbidities, the routine fixation of the LT in this population may not be necessary, particularly in cases where the anticipated functional benefits are minimal. However, the significantly higher RUSH scores observed in the cephalomedullary nail with cerclage wire group suggest that fixation may accelerate fracture healing, potentially allowing for earlier mobilization and improved weight-bearing capacity.
This study has several limitations. First, while our results suggest that LT fixation does not impact hip flexor strength in cases with 5–10 mm displacement, the generalizability to larger LT displacement (>10 mm) or cases with severe posteromedial wall comminution remains uncertain. The biomechanical significance of LT fragments may vary depending on the extent of medial wall compromise, potentially influencing the need for fixation. Future RCT should explore whether fixation provides functional or biomechanical benefits in cases with >10 mm displacement, as these patients may exhibit different stability characteristics, healing patterns, and weight-bearing capacities.
Second, this study did not incorporate quantitative muscle imaging or electromyographic assessments to further evaluate potential compensatory mechanisms in hip flexion strength. While our results indicate that iliopsoas dysfunction may not be clinically significant in these cases, advanced imaging or functional assessments could provide more insight into whether other muscle groups compensate for LT displacement.
Third, while our study found a significantly higher RUSH score in the cerclage wire group, the clinical significance of this finding remains uncertain. The FAITH trial suggests a union threshold of 18 at 6 months, 19 and RUSH scoring beyond this timeframe has not been fully validated. Although improved RUSH scores may indicate enhanced radiographic healing, it is unclear whether this translates into faster mobility recovery, a lower risk of secondary fractures, or long-term functional benefits. Future studies should explore whether higher RUSH scores at later time points correlate with better gait mechanics, patient-reported outcomes, and long-term quality of life measures, while extending follow-up beyond 12 months.
Lastly, although our study was powered to detect a clinically meaningful difference (MCID) of 16 N, the power calculation was based on literature comparing hip flexor strength in normal hips versus non-fixed LT fracture patterns, 16 rather than direct comparisons between fixation and non-fixation groups. This may affect the applicability of our findings, and future studies should derive power calculations from direct comparisons to enhance validity. Additionally, post hoc analysis revealed that while our study was adequately powered for the MCID, it was underpowered to detect smaller observed differences (2.0 N), with only 5.8% power. Detecting such small differences would require a larger sample size. While alternative outcomes could have been used for sample size estimation, hip flexor strength was chosen because no prior studies have measured it in patients undergoing this specific surgical approach. Given the lack of direct comparative data, we based our power calculation on existing literature comparing hip flexor strength in normal hips versus non-fixed LT fracture patterns, assuming that fixation may restore strength closer to the contralateral limb. Future studies should aim to validate this assumption by directly comparing fixation and non-fixation groups while also considering alternative functional outcomes, such as gait analysis, patient-reported outcomes, and return to activity measures, to provide a more comprehensive assessment of clinical benefits.
Conclusion
This RCT demonstrates that in unstable intertrochanteric fractures with LT displacement of 5–10 mm, cerclage wire fixation does not significantly improve hip flexor strength or functional outcomes compared to standard cephalomedullary nail fixation alone. However, LT fixation was associated with enhanced fracture healing, as evidenced by significantly higher RUSH scores, suggesting that it may facilitate earlier weight-bearing and rehabilitation. Given the longer operative time required for LT fixation, its use should be selectively considered in cases where fracture healing is a primary concern, rather than for functional restoration of hip flexor strength. Further research with larger sample sizes and extended follow-up is warranted to clarify the long-term clinical implications of LT fixation in this population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Faculty of Medicine, Srinakharinwirot University. (Contract No. 534/2566)