
Abstract
Keywords
Introduction
Osteoporosis (OP) is a systemic metabolic bone disease characterized by decreased bone mass, decreased bone strength and increased bone fragility. Osteoporotic vertebral compression fracture (OVCF) is a common complication of OP. OVCF can lead to loss of fracture cone height, kyphosis and intractable back pain. 1 At the same time, the expert consensus in 2021 shows that the mortality rate of OVCF patients after 1 year of fracture is significantly higher than that of the general population, and the 4-year survival rate is only 50 %, which seriously threatens the life safety of patients. 2
Percutaneous vertebroplasty (PVP) is a classic surgical procedure for treating osteoporotic vertebral compression fractures (OVCF). It involves percutaneous injection of bone cement into the fractured vertebra to enhance its strength and stiffness, thereby preventing further vertebral collapse and deformity. 3 However, as most OVCF patients are elderly, their post-fracture callus formation tends to be slow. As shown in the study by Chen Weina et al., 4 the incidence of delayed fracture healing after surgery in OVCF patients is as high as 45.57%. Delayed fracture healing can prevent patients from bearing normal loads or resuming regular work, leaving them with persistent low back pain. Some patients may even require secondary surgery, which not only increases their financial burden but also raises the risk of poor prognosis. 5 Therefore, there is an urgent clinical need to investigate the factors influencing delayed healing in OVCF patients postoperatively and to construct a predictive model.
Asprosin is a peptide hormone and a C-terminal cleavage product of fibrillin. In the review of Ovali MA, 6 it was mentioned that Asprosin can affect the bone mineral density of patients through various ways such as glucose metabolism and regulation of insulin sensitivity. MicroRNA-21 (miR-21) is located on human chromosome 17q23.2. miR-21 has always been considered as a proto-oncogene. At present, clinical research focuses on angiogenesis, inflammation and immunity.7,8 However, some studies have shown that miR-21 is also involved in bone diseases. In the study of Li X, 9 miR-21 can be directly involved in regulating the expression of bone marrow mesenchymal stem cells, osteoblasts and osteoclasts, and regulating bone tissue balance. Therefore, it is speculated that serum Asprosin and miR-21 may be involved in the postoperative fracture healing of OVCF patients. In view of this, this study focuses on the analysis of the relationship between the two and the postoperative delayed healing of patients.
Materials and methods
Study design
A prospective study was conducted, and 300 OVCF patients admitted to the hospital from June 2022 to June 2024 were selected as the study subjects. All patients underwent preoperative serum asprosin and miR-21 testing. Three months post-surgery, X-rays were used to assess fracture healing, and the patients were divided into a delayed healing group and a normal healing group. The baseline data of the two groups were statistically analyzed and compared. The least absolute shrinkage and selection algorithm (LASSO) regression was used to screen the factors that may affect the delayed healing of OVCF patients after surgery, and binary logistics regression analysis was performed. A nomogram model for delayed healing of OVCF patients after surgery was constructed, and the receiver operating characteristic (ROC) curve was drawn to evaluate the value of the nomogram model in predicting delayed healing of OVCF patients after surgery.
Patient population
Inclusion criteria: ① OVCF meets the diagnostic criteria of the 2021 consensus guidelines 2 ; ② PVP treatment is performed in accordance with the “Expert Consensus on Percutaneous Vertebroplasty Surgical Techniques” 10 ; ③ Surgery is performed by the same group of physicians, and there are no serious complications after the surgery; ④ Single vertebral compression fracture with no symptoms of spinal cord compression; ⑤ Age ≥18 years. Exclusion criteria: ① Secondary osteoporosis; ② Recent use of medications that may affect bone metabolism; ③ Concomitant thyroid disease; ④ Combined with other orthopedic diseases; ⑤ History of thoracolumbar surgery; ⑤ Combined with immune system diseases.
According to the above inclusion and exclusion criteria, a prospective study was conducted and 300 patients with OVCF admitted to the hospital from June 2022 to June 2024 were selected as study subjects. This study was approved by the hospital’s medical ethics committee, and informed consent was obtained from all patients.
Baseline data
Baseline data of the patients were collected through the hospital medical records system, including gender, age, body mass index (BMI), fracture site, bone mineral density T score [measured using a dual-energy X-ray absorptiometry device (Osteosys Co., Ltd, CFDA approval number: 20172061588)], height recovery rate of injured vertebral, improvement of kyphosis Cobb angle, bone cement injection volume, cause of the disease, delayed weight-bearing after surgery (unable to complete weight-bearing exercises more than 12 weeks after surgery), combined hyperlipidemia, hypertension, and diabetes, smoking history and drinking history.
Criteria for delayed healing and grouping
According to the criteria in the Diagnosis and treatment of nonunion of osteoporotic thoracolumbar fractures, 11 X-ray examination (Canon, CFDA approval number: 20173061346) was performed 3 months after surgery. Delayed healing was defined as no or minimal callus formation, visible gaps at the fracture site, and sclerotic bone edges. Patients with delayed fracture healing were assigned to the delayed healing group (n = 74), while those with normal healing were assigned to the normal healing group (n = 226).
Serum asprosin and miR-21 testing methods
Before surgery, 5 mL of fasting venous blood was collected from the patients and centrifuged at 3500 rpm for 15 minutes with a 10 cm radius using a centrifuge centrifuge (Fresenius Kabi AG, CFDA approval number: 20183100418) to separate the serum. Serum asprosin levels were measured using enzyme-linked immunosorbent assay (ELISA). Total RNA was extracted from the serum using the TRIzol method, and reverse transcription was performed using a reverse transcription kit to convert total RNA into complementary DNA (cDNA). Reverse transcription conditions were 37°C for 15 minutes and 85°C for 5 seconds. PCR amplification was conducted using cDNA as a template. Primer sequences were as follows: forward primer 5′-GCGGTAGCTTATCAGACTGA-3′, reverse primer: 5′-TGCGTGTCGTGGAGTC-3′. PCR reaction conditions were: 95°C for 10s, 95°C for 5s, 60°C for 30 s, for a total of 40 cycles. Using U6 as an internal control, and the relative expression level of miR-21 was calculated using the 2- ∆∆CT method. All kits were provided by Roche Molecular Systems, Inc.
Statistical methods
SPSS25.0 software was used for data processing. The measurement data were expressed as “
Results
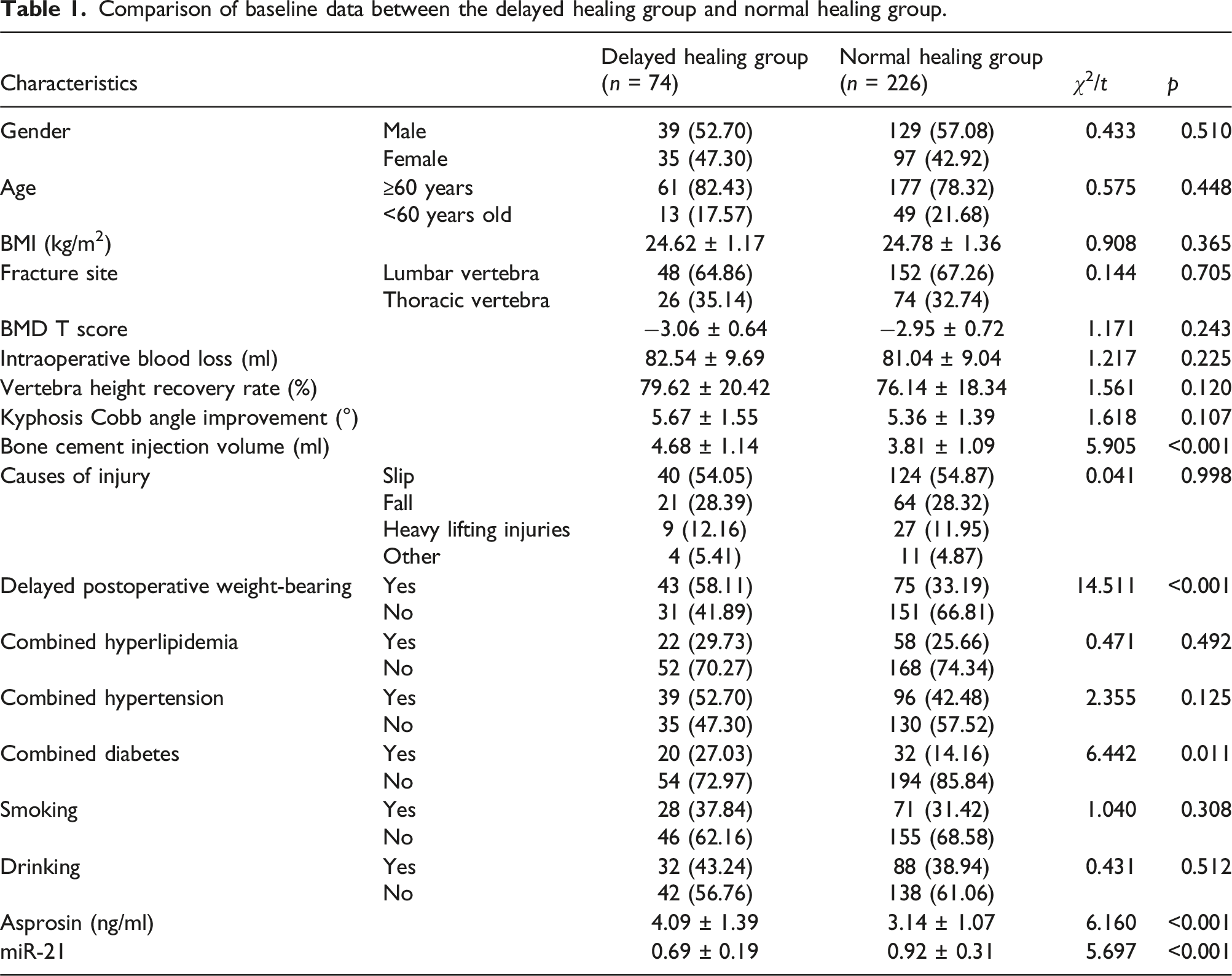
Comparison of baseline data between the delayed healing group and the normal healing group
Comparison of baseline data between the delayed healing group and normal healing group.
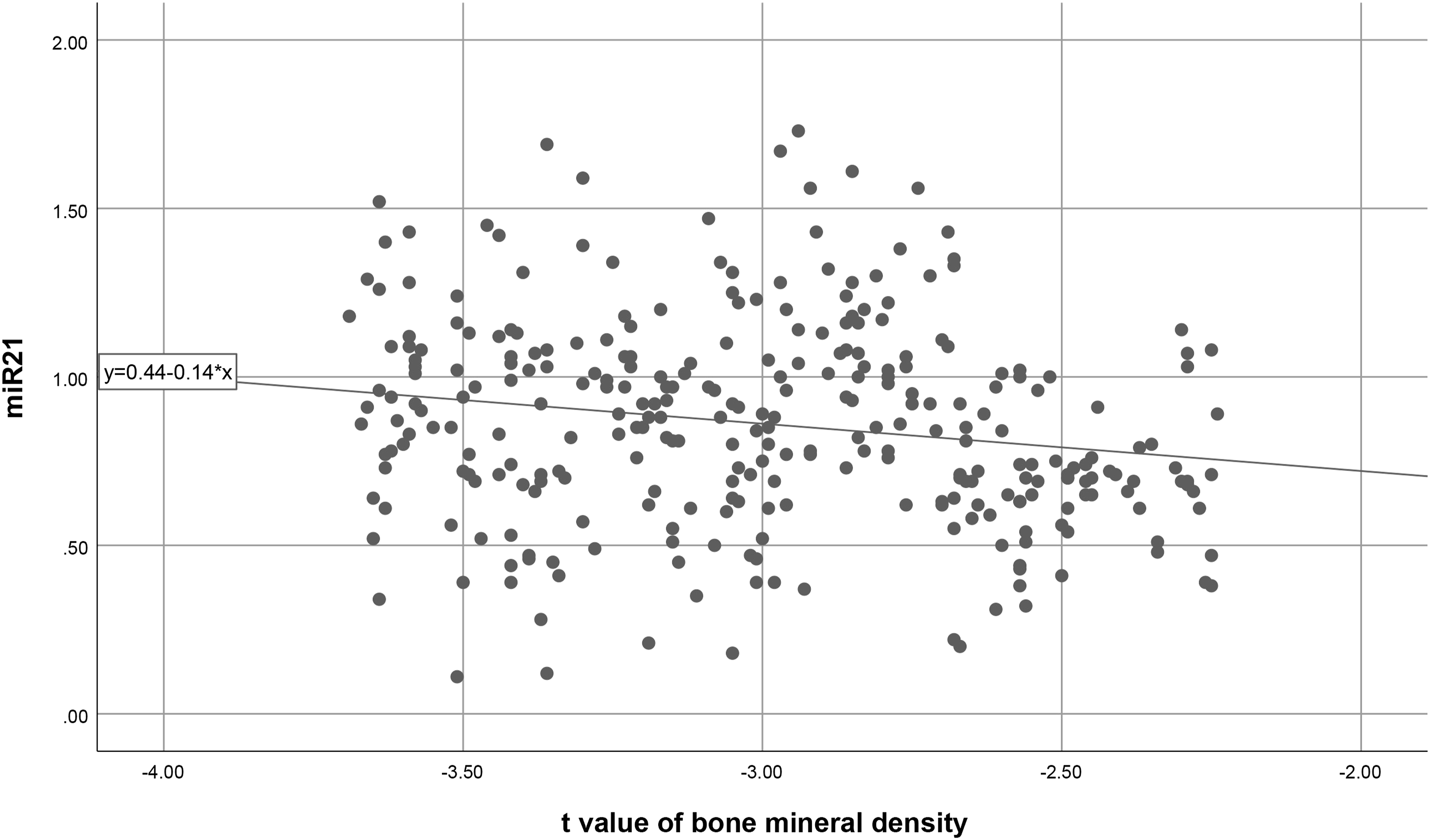
Correlation between serum asprosin, miR-21 levels, and bone mineral density T score in OVCF patients
The bone density T score of OVCF patients was positively correlated with asprosin (r = 0.281, p < 0.001) and negatively correlated with miR-21 (r = −0.184, p = 0.001). The scatter plots are shown in Figures 1 and 2. Scatter plot of bone density T score and serum Asprosin levels in OVCF patients. Scatter plot of bone density T score and serum miR-21 levels in OVCF patients.
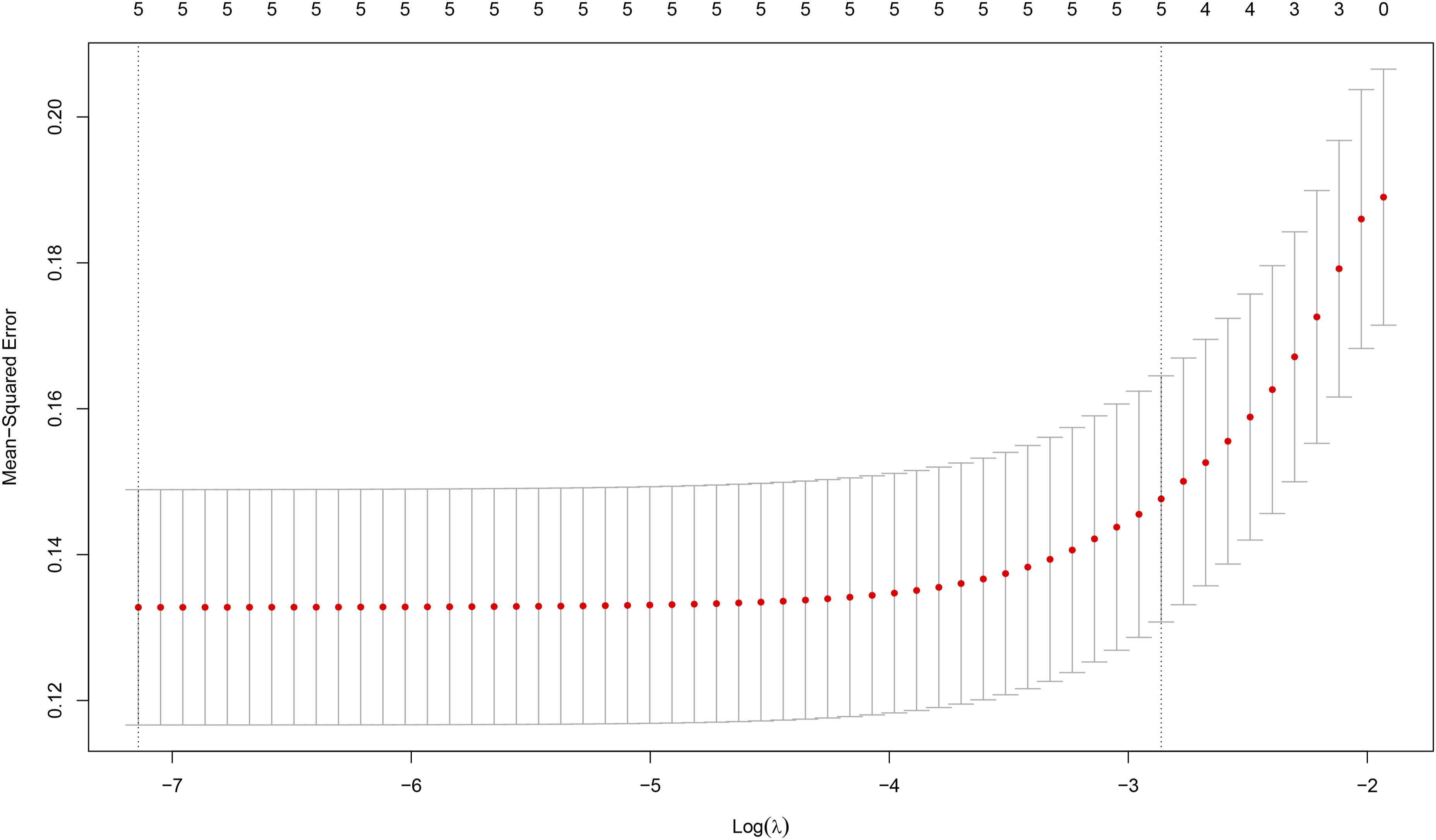
LASSO regression screening results for delayed healing in OVCF patients
The LASSO regression model identified five potential factors associated with postoperative delayed healing in patients with OVCF. These factors are: bone cement injection volume, postoperative delayed weight-bearing, combined diabetes, serum asprosin levels, and serum miR-21 levels. See details in Figures 3 and 4. LASSO regression coefficient path. LASSO regression cross validation results.
Regression analysis of influencing factors of delayed healing in OVCF patients
Regression analysis of influencing factors for delayed healing in OVCF patients.

Construction of a nomogram prediction model for delayed healing in OVCF patients
Based on the factors with differences in Table 2 (bone cement injection volume, delayed weight bearing, combined diabetes, serum asprosin, serum miR-21), a nomogram prediction model for delayed healing after surgery in OVCF patients was constructed (see Figure 5). The nomogram model was validated using the Bootstrap internal validation method (see Figure 6), and the results showed that the C-index value was 0.867. Nomogram for delayed healing after OVCF surgery. Calibration curve of nomogram for delayed healing after surgery in OVCF patients.

The value of the nomogram model in predicting delayed healing after OVCF surgery
The ROC curve was drawn to perform internal validation of the nomogram model. The results showed that the AUC of the nomogram for predicting delayed healing after surgery in OVCF patients was 0.868 (95% confidence interval 0.824-0.911, p < 0.001), the specificity was 0.686, the sensitivity was 0.892, and the Youden index was 0.578. See Figure 7 for details. ROC curve for the nomogram model predicting delayed healing after surgery in OVCF patients.
Serum levels of asprosin and miR-21 in OVCF patients before treatment and 3 months after treatment
After 3 months of treatment, serum Asprosin [(3.46 ± 1.22) ng/ml] in OVCF patients was lower than that before treatment [(3.03 ± 1.03) ng/ml], and serum miR-21 (0.85 ± 0.30) was higher than that before treatment [ (0.99 ± 0.33)] (t = 4.039, 4.318, p < 0.05).
Discussion
As a mature minimally invasive spinal surgery, PVP is widely used in clinical practice due to its advantages in improving local spinal symptoms and restoring limb mechanical strength. Most OVCF patients can achieve good recovery of the fractured vertebra after PVP surgery, however, a small number of patients experience delayed healing or even non-healing of fractures after surgery. The research data of Jia Jinlong et al. 12 showed that the incidence of delayed healing of fractures after PVP surgery in OVCF patients was 26.53%, which is similar to the 24.67% in this study.
Fracture healing is a trauma repair process in which osteoblasts and osteoclasts interact with each other, and the proliferation and differentiation of both play a decisive role in this process. 13 Recent studies have shown that some adipose factors can regulate the proliferation and differentiation of osteoclasts and osteoblasts, inhibit the expression of intracellular osteogenic signals, and thus affect bone metabolism and participate in bone healing. 14 Asprosin is a secretory adipose factor secreted by white adipose tissue. Some studies have shown that changes in asprosin levels are closely related to bone mineral density in diabetic patients 15 miR-21 is an important member of the miRNA family. Existing studies have shown that miR-21 plays an important role in embryonic development and cell differentiation. 16 Furthermore, Meng Yubin’s 17 doctoral thesis found that high expression of miR-21 can increase the expression of osteogenic-related genes in human umbilical cord mesenchymal stem cells, thereby participating in the osteogenic differentiation process. Therefore, serum asprosin and miR-21 levels may be related to postoperative fracture healing in OVCF patients.
Five potential factors related to delayed healing after surgery in OVCF patients were finally screened out through the LASSO regression model: the bone cement injection volume, postoperative delayed weight bearing, combined diabetes, serum asprosin level, and serum miR-21 level. High expression of serum asprosin: Xue Guohui et al. 18 found that asprosin can promote the release of inflammatory factors such as tumor necrosis factor-α (TNF-α) in pancreatic β cells and skeletal muscle cells. TNF-α can directly or indirectly regulate bone metabolism through inflammatory and oxidative stress response pathways, regulate the proliferation and differentiation of osteoclasts and osteoblasts, and accelerate bone loss in OVCF patients. 19 Additionally, TNF-α can enhance the expression of V-ATPase on osteoclasts, thereby enhancing the bone resorption activity of osteoclasts, destroying the balance between osteoblasts and osteoclasts, and thus affecting the postoperative bone healing of patients. 20 Asprosin can also promote the expression of Toll-like receptor 4 (TLR4), activate the phosphorylation of JNK, and mediate β-cell inflammatory response, cell dysfunction and apoptosis through the TLR4/JNK signaling pathway, thereby affecting the postoperative recovery of OVCF patients. TLR4 can also disrupt the normal function of osteoblasts and osteocytes, disrupt the balance of bone metabolism, and thus affect bone healing. In a mouse experiment by Cao, 21 it was found that knocking out TLR4 in diabetic osteoporosis mice could effectively delay the progression of the disease in mice. This shows that asprosin can indirectly affect the bone metabolism level of OVCF patients by promoting TLR4 expression and inflammatory response, thereby increasing the risk of delayed healing after surgery. Low expression of miR-21: With the deepening of clinical research, more and more studies have found that miR-21 is closely related to osteoblast differentiation. Studies have shown that miR-21 can regulate osteogenesis by targeting specific target genes. Spry2 is one of the target genes and is a key regulatory factor for osteoblast differentiation. 22 Yang Nan 23 found that miR-21 can upregulate the osteoblast-related gene core binding factor subunit α1 by regulating the signal transduction of Spry2, promote the differentiation of mesenchymal stem cells into osteoblasts, and promote bone healing. In addition to regulating osteoblasts, a 2020 study found that miR-21 can negatively regulate osteoclastogenesis and bone resorption by intervening in the target gene PTEN and activating the PI3K/Akt signaling pathway. 22 Therefore, miR-21 can effectively regulate the balance of osteoblasts and osteoclasts and promote bone healing. 24
The results of binary logistic regression analysis showed that, in addition to serum asprosin and miR-21 levels, delayed weight-bearing after surgery, combined diabetes, and bone cement injection volume were also influencing factors for delayed healing after surgery in OVCF patients. Delayed postoperative weight-bearing: Fracture healing is a complex biological repair process, which is affected by mechanical stress stimulation and blood supply. Mechanical stress stimulation is one of the important factors, and weight-bearing is one of the common ways of mechanical stimulation of fracture callus. 25 Schwarz C’s 26 rat study showed that the newly formed bone tissue at the fracture site of rats in the mechanical loaded group was significantly higher than that in the unloaded group, suggesting that mechanical stress stimulation can stimulate osteoblast proliferation, differentiation, and secretion of extracellular matrix. Additionally, mechanical stress stimulation can also improve the bone microenvironment, promote the release of growth factors at the fracture site, promote local angiogenesis, and thus promote fracture healing. Combined diabetes: Due to changes in glucose homeostasis, diabetic patients can inhibit osteocalcin and insulin-like growth factor-1 and increase reactive oxygen species, thereby causing bone loss. Long-term hyperglycemia can directly affect the function and differentiation of osteoblasts, and has a toxic effect on the differentiation of bone marrow interstitial cells such as adipocytes. It can also increase the production of bone marrow adipocytes by upregulating oxidase proliferator-activated receptor γ, thereby affecting the function of osteoblasts and osteoclasts, leading to delayed fracture healing. 27 Bone cement injection volume: A higher injection volume of bone cement indicates more severe disease, making postoperative fracture healing more difficult. Lai Xianliang ‘s 28 study showed that a large amount of bone cement injected does not significantly improve the patient’s clinical efficacy, but can cause the bone cement penetration rate to be as high as 30% to 41%, thereby affecting the patient’s postoperative fracture healing. The ROC results showed that the AUC of the nomogram for predicting delayed healing after surgery in OVCF patients was 0.868 (95% confidence interval 0.824-0.911, p < 0.001), the specificity was 0.686 , the sensitivity was 0.892, and the Youden index was 0.578, indicating that the nomogram model constructed based on serum asprosin and miR-21 can effectively predict the risk of delayed healing after surgery in OVCF patients.
However, this study has certain limitations, such as a small sample size and single-center design, which may limit the generalizability of the results. Additionally, only preoperative serum Asprosin and miR-21 levels were evaluated, and continuous monitoring of these levels in OVCF patients was not performed, which could have helped in analyzing the relationship between their changes and fracture healing. Future studies should consider a multi-center design and a larger sample size to validate our findings. Moreover, further mechanistic studies should be included to explore the specific role of serum Asprosin and miR-21 in the physiological process of fracture healing in OVCF patients.
In conclusion, serum Asprosin and miR-21 levels are closely associated with delayed fracture healing in OVCF patients. Additionally, bone cement injection volume, delayed postoperative weight-bearing, and diabetes comorbidity are important factors affecting fracture healing. A nomogram model based on these factors can effectively predict the risk of delayed fracture healing in OVCF patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Anhui Medical University Fund Support Project (2023xkj097) and Key Project of Natural Science Research in Anhui Provincial Universities by the Education Department of Anhui Province (2022AH050749).
Data Availability Statement
Data available on request from the authors.