
Abstract
Purpose
To analyze the effect of artificial dermis technology combined with full-thickness skin graft coverage in the treatment of foot and ankle wound defects in the elderly.
Methods
A total of 90 elderly patients treated for foot and ankle wound defects from January 2021 to December 2022 were selected as the study subjects and were divided into a control group of 40 cases and a study group of 50 cases according to the random number table method. The control group was treated with retrograde saphenous nerve flap transplantation, while the study group was treated with artificial dermis technology combined with full-thickness skin graft coverage. The therapeutic effect of artificial dermis technology combined with full-thickness skin graft coverage was observed. The ankle function, pain level, postoperative wound recovery, relevant indicators, and postoperative wound complications were compared between the two groups.
Results
At 2 and 4 weeks after treatment, the ankle function of both groups was higher than before treatment, and the ankle function of the study group was higher than that of the control group (p < .05). At 2 and 4 weeks after treatment, the VAS and PPI scores of both groups were lower than before treatment, and the VAS and PPI scores of the study group were lower than those of the control group (p < .05). Compared with the control group, the study group had lower color, thickness, vascular distribution, and softness, as well as shorter surgical preparation time, hospital stay, antibiotic use, and fewer dressing changes. The overall incidence of flap edema, wound infection, and total wound infection was lower in the study group (p < .05).
Conclusion
The use of artificial dermis technology combined with full-thickness skin graft coverage in the treatment of foot and ankle wound defects in the elderly helps to improve ankle joint function, reduce the degree of pain, and results in better postoperative wound recovery and a lower complication rate.
Keywords
Introduction
The structure of the foot is composed of joints interconnecting numerous bones, allowing the foot to directly bear the body’s weight while maintaining optimal stability and mobility. 1 With a normal foot structure, the muscular system expends minimal effort to support the body’s weight. 2 The ankle joint, located at the junction of the tibia, fibula, and talus, enables dorsiflexion and plantarflexion in the sagittal plane. Despite its small area, the ankle joint plays a crucial role in body posture and in transferring the body’s weight to the foot during standing, walking, and running. 3 When a wound defect occurs in the foot and ankle area, coupled with the decreased mobility and restricted joint activity in the elderly, as well as exposed tendons and bones, it becomes very difficult for the injured person to move the affected area voluntarily. 4 Elderly patients often have decreased physical functions and multiple underlying diseases, making the choice of treatment for foot and ankle wound defects particularly critical. Artificial dermis technology combined with full-thickness skin graft coverage can form new active granulation tissue within the induced membrane, offering advantages such as reliability and mechanical isolation. 5 Based on this, this article aims to analyze the effect of artificial dermis technology combined with full-thickness skin graft coverage in the treatment of foot and ankle wound defects in the elderly.
Materials and methods
General information
A total of 90 elderly patients with foot and ankle wound defects treated in our hospital from January 2021 to December 2022 were selected as the study subjects and were divided into a control group of 40 cases and a study group of 50 cases according to the random number table method. The control group had an age range of 62-78 years, with an average age of (70.65 ± 7.56) years; the wound defect area ranged from 4.5 cm × 6.3 cm to 7.1 cm × 12.6 cm; the causes of injury included 17 cases of crush injury and 23 cases of traffic accident injury; the injured sites were 8 cases in the lower segment of the leg, 20 cases in the foot and ankle, and 12 cases in the dorsum of the foot; combined injuries included 19 cases of tendon rupture and 21 cases of ankle fracture. The study group had an age range of 61-79 years, with an average age of (71.21 ± 7.57) years; there were 21 cases of crush injury and 29 cases of traffic accident injury; the injured sites were 10 cases in the lower segment of the leg, 24 cases in the foot and ankle, and 16 cases in the dorsum of the foot; combined injuries included 24 cases of tendon rupture and 26 cases of ankle fracture. The general information of the two groups was comparable (p > .05). This study was approved by the ethics committee of our hospital.
Inclusion criteria: (1) Patients met the diagnostic criteria for elderly foot and ankle wound defects in the “Expert Consensus on the Clinical Diagnosis and Treatment of Post-Traumatic Multiple Organ Dysfunction Syndrome” 6 ; (2) Age ≥60 years; (3) Confirmed by imaging examination; (4) Normal mental and willpower, able to communicate normally; (5) Both patients and their families were informed and signed the consent form.
Exclusion criteria: (1) Abnormal heart, liver, or kidney function; (2) Combined with diseases affecting tissue healing; (3) Incomplete clinical data; (4) Combined with other organic diseases; (5) Patients intolerant to surgical treatment; (6) History of mental illness; (7) Poor patient compliance.
Treatment methods
The control group was treated with retrograde saphenous nerve flap transplantation. The flap was designed first, and the flap was trimmed according to the size of the wound in the patient’s foot and ankle. The line connecting the midpoint between the lateral malleolus and the Achilles tendon to the midpoint of the popliteal fossa was used as the axis. A pneumatic tourniquet was used, and no blood or partial blood was driven out to facilitate the identification of the small saphenous vein. The skin was incised along the flap with a rotation point, the skin was incised and separated to both sides, and the subcutaneous tissue was excised. The wound was cleaned with iodine and normal saline, and the wound was sutured to complete the surgery.
The study group was treated with artificial dermis technology combined with full-thickness skin graft coverage. (1) Before surgery, patients were treated symptomatically for underlying diseases. Patients were placed in a supine position and were given general anesthesia combined with epidural anesthesia. Under the condition of a tourniquet, debridement was performed, the muscle interval was excised and decompressed, and the wound and surrounding skin were repeatedly cleaned with hydrogen peroxide, iodine, and normal saline to completely remove the necrotic wound and perform anti-inflammatory treatment. To prevent cross-infection, disposable gloves were changed, and for those with dislocation or fracture, Kirschner wires, titanium plates, and screws were used for coverage, and the ruptured tendons were sutured and repaired. The negative pressure closed drainage (VSD) dressing was trimmed and spliced according to the area and shape of the wound to cover the wound. The mesentery method was used to close the wound and connect the VSD, and the gaps were filled in layers to avoid effusion. The pressure was maintained at -120-250 mmHg for negative pressure suction, and the VSD was stopped after 4-7 days, and the dressing was changed according to the individual’s condition. If the expanded wound showed exposed bone in the foot and ankle, exposed soft tissue of the dorsal foot tendon, or infected wound, antibacterial drugs could be placed on the wound, and bone cement was used for coverage, and holes were drilled on the surface of the bone cement for coverage, and sterile gauze was used for press coverage. When the wound was free of infection, artificial dermis coverage surgery could be performed. After the surgery, the wound was covered with plaster and antibiotics were given. (2) In the second-stage surgery, the gauze and artificial dermis were removed. If the granulation growth was good and there was no exposure of tendons and bones, disinfection and edge cleaning were performed, the area of skin defect in the wound was measured, and the skin was taken from the iliac fossa according to the size and shape of the wound, and planted in the defective area of the wound, covered with gauze, and finally covered with plaster for fixation. (3) The affected area was placed in an elevated position to prevent diseases such as lower limb venous thrombosis.
Observation indicators
① Observe the therapeutic effect of full-thickness skin graft coverage using induced membrane technology. ② Ankle function: The Kofoed scoring standard was used to evaluate the ankle function of patients before treatment and at 2 and 4 weeks after treatment from aspects such as pain and toe walking activity. Scores of 85-100 were considered excellent, 75-85 good, 70-74 pass, and below 70 poor. ③ Pain degree: The visual analog scale (VAS) and the present pain intensity scale (PPI) were used to assess the pain degree of patients before treatment and at 2 and 4 weeks after treatment. The total score of VAS was 0-10, with higher scores indicating more severe pain; PPI had a total of 5 points, with 0 for no pain, 1 for mild discomfort, 2 for discomfort, 3 for distress, 4 for terrible pain, and 5 for extreme suffering. ④ Postoperative wound recovery: The Vancouver Scar Scale was used to assess the color, thickness, vascular distribution, and softness of patients before treatment and at 2 and 4 weeks after treatment. The scores were 0-3 for color, 0-4 for thickness, 0-3 for vascular distribution, and 0-5 for softness, with higher scores indicating worse postoperative wound recovery. ⑤ Related indicators: The surgical preparation time, hospital stay, antibiotic use time, and dressing change times of the two groups were recorded. ⑥ Postoperative wound complications: Complications such as flap edema, wound infection, and Flap (or skin graft) necrosis that occurred after surgery in the two groups were recorded.
Statistical processing
SPSS 19.0 statistical software was used for analysis and processing. Measurement data were described as mean ± standard deviation (
Results
Effect of artificial dermis technology combined with full-thickness skin graft coverage
Typical case: A patient suffered from a right anterior ankle and foot reverse avulsion injury due to a traffic accident, resulting in severe contamination and local skin soft tissue and toe extensor tendon defects. The patient underwent emergency debridement of the right foot, repositioning of the long toe extensor tendon, coverage of the interphalangeal joint, and reverse skin grafting with VSD coverage. One week postoperatively, the VSD was removed, revealing extensive necrosis of the reverse skin graft, as shown in Figure 1 (a)–(b). In the second phase, the patient underwent expansion debridement and artificial dermis coverage for the necrotic skin and soft tissue of the right foot, as shown in Figure 1(c) . After expansion, exposure of the outer ankle bone and dorsal foot tendon tissue was observed. Following artificial dermis coverage, as shown in Figure 1(d), the artificial dermis outer membrane was removed 3 weeks later, as shown in Figure 1(e). After removal of the artificial dermis, the wound was debrided, and good granulation growth was observed, especially at the exposed bone and tendon sites, as shown in Figure 1(f). Skin was harvested from the iliac fossa and grafted onto the defective area of the wound, as shown in Figure 1(g). One month postoperatively, the grafted skin showed good survival, as shown in Figure 1(h). The ankle function 1 month postoperatively is shown in Figure 1(i)–(j). Effect of artificial dermis technology combined with full-thickness skin graft coverage.
Comparison of ankle function between the two groups
Comparison of ankle function between the two groups (

This table shows that the ankle function of the study group improved significantly more than that of the control group at 2 and 4 weeks after treatment, indicating the effectiveness of the artificial dermis technology combined with full-thickness skin graft coverage in enhancing ankle function in elderly patients with foot and ankle wound defects.
Comparison of pain intensity between the two groups
Comparison of pain intensity between the two groups (

This table illustrates the effectiveness of the treatment in reducing pain, as measured by the Visual Analog Scale (VAS) and the Present Pain Intensity (PPI) scale. The study group showed significantly greater improvement in pain reduction compared to the control group, indicating the potential benefits of the artificial dermis technology combined with full-thickness skin graft coverage in managing postoperative pain in elderly patients with foot and ankle wound defects.
Comparison of postoperative wound recovery between the two groups
Comparison of postoperative wound recovery between the two groups (
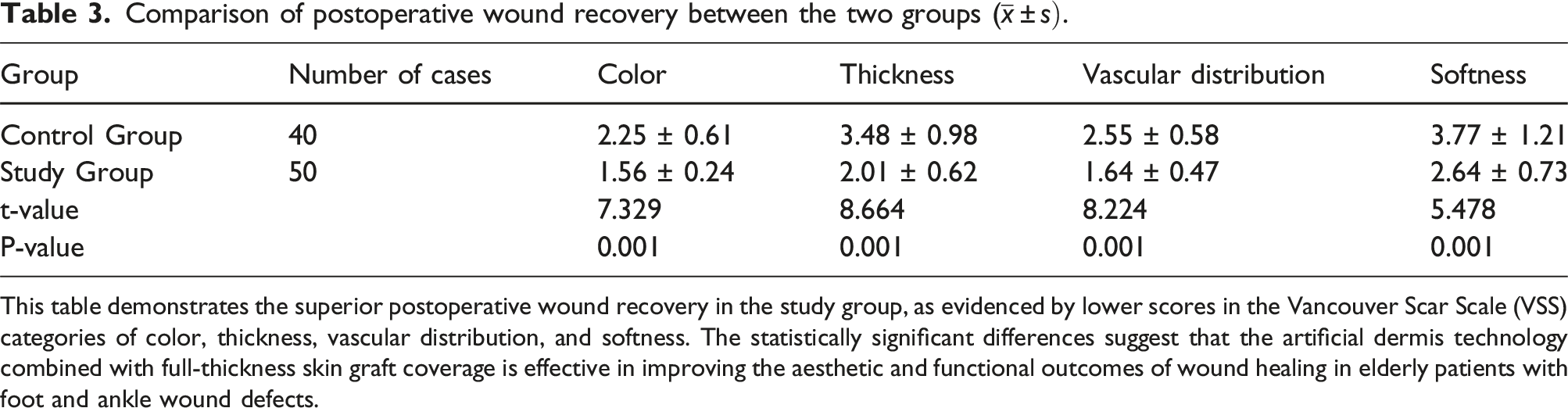
This table demonstrates the superior postoperative wound recovery in the study group, as evidenced by lower scores in the Vancouver Scar Scale (VSS) categories of color, thickness, vascular distribution, and softness. The statistically significant differences suggest that the artificial dermis technology combined with full-thickness skin graft coverage is effective in improving the aesthetic and functional outcomes of wound healing in elderly patients with foot and ankle wound defects.
Comparison of related indicators between the two groups
Comparison of related indicators between the two groups (

This table highlights the efficiency of the treatment in the study group, as evidenced by reduced surgical preparation time, hospital stay, and antibiotic use time, along with fewer dressing changes. These statistically significant differences suggest that the artificial dermis technology combined with full-thickness skin graft coverage not only improves wound healing but also optimizes the overall treatment process, reducing the burden on both patients and healthcare providers.
Comparison of postoperative wound complications between the two groups
Comparison of postoperative wound complications between the two groups (

This table demonstrates that the study group had significantly fewer postoperative complications, indicating that the artificial dermis technology combined with full-thickness skin graft coverage is effective in reducing the risk of complications in elderly patients with foot and ankle wound defects.
Discussion
Artificial dermis serves as a dermal regeneration template, capable of guiding the wound to generate thicker dermal tissue. This newly formed dermal-like tissue has a structure and function similar to that of normal dermis. 7 Artificial dermis not only protects the wound but also primarily guides the reconstruction of the dermal layer, preventing wound contraction and ensuring skin elasticity. The material is also completely biodegradable and is replaced by host cells. 8 In skin grafting, the current consensus is that the thickness of the dermal layer determines the quality of the graft. Adequate thickness of the dermal layer can prevent the contraction of the graft and the subsequent proliferation of scars.9,10 Therefore, split-thickness skin grafts, which lack a dermal layer, are prone to contraction and scar proliferation, while full-thickness skin grafts, which include more dermal layers, have better grafting effects. 11 Skin grafts are typically harvested from the patient’s own body and are categorized into split-thickness, full-thickness, and dermal vascular network grafts based on their thickness. 12 Full-thickness skin grafts include the epidermal and dermal layers, as well as some skin appendages such as hair follicles and sweat glands, with a thickness of approximately 1 mm.13,14 The advantages of full-thickness skin grafts are minimal late contraction, superior color and texture, and good elasticity and wear resistance. However, they require higher vascular conditions and nutritional status of the recipient bed, and the technical operation requirements are high. 15 After full-thickness skin grafting with artificial dermis technology, as the nerves in the recipient area slowly grow into the graft, the graft, rich in elastic fibers, glands, and capillaries within the dermal layer, can quickly grow and fuse with the recipient tissue, maintaining skin color. After survival, the graft can slightly contract, and the sensory and motor functions of the foot gradually recover. 16
Based on the overall results of this study, the clinical significance and application value of artificial dermis technology combined with full-thickness skin graft coverage in the treatment of elderly foot and ankle wound defects are evident. Compared with traditional methods such as retrograde saphenous nerve flap transplantation, this combination therapy not only significantly improves ankle joint function and reduces pain levels but also promotes better postoperative wound recovery with fewer complications. These findings highlight the innovation of our study, as it provides a more effective and safer treatment option for elderly patients with foot and ankle wound defects.
The innovation of our study lies in combining artificial dermal technology with full-thickness skin graft fixation for the treatment of foot and ankle wound defects in the elderly. Previous studies have mostly focused on single treatment methods, while our study systematically evaluated the application of artificial dermal technology in this field by comparing two different treatment plans and analyzing from multiple dimensions (such as ankle function, pain levels, postoperative wound recovery, etc.), providing new ideas and references for subsequent research and clinical practice.
When comparing the study group with the control group, several key advantages of using artificial dermis technology combined with full-thickness skin graft coverage are observed. Firstly, the surgical procedure is simpler and requires less time, reducing the overall risk during surgery. Secondly, the postoperative recovery is faster, as evidenced by better ankle function and lower pain scores. Additionally, the incidence of complications such as flap edema and wound infection is significantly lower in the study group. These advantages can be attributed to the reliable and mechanical isolation properties of artificial dermis, which facilitate the formation of new active granulation tissue within the induced membrane.
Despite the promising results, there are certain limitations to the surgical method used in the study group. The effectiveness of the grafting may be compromised if the wound is severely infected or if the tissue defect is too large. Moreover, the relatively high cost of artificial dermis materials could pose an economic burden on patients. Future studies should focus on addressing these limitations and exploring ways to optimize the surgical process and material selection.
The key points to ensure the success of the surgery and patient safety during the procedure include: (1) Thorough Preoperative Assessment: A comprehensive evaluation of the patient’s underlying diseases should be conducted to ensure that the patient can tolerate the surgery. At the same time, a detailed examination of the wound condition, including the size, depth, and infection status of the wound, should be performed to provide a basis for the formulation of the surgical plan. (2)Thorough Debridement: Thorough debridement of the wound should be performed before surgery to remove necrotic tissue and infectious materials, ensuring a clean wound and creating favorable conditions for the subsequent grafting surgery. (3)Accurate Grafting Operation: During the grafting process, the accurate placement and fixation of artificial dermis and full-thickness skin grafts should be ensured to avoid displacement or wrinkling, which can improve the success rate and effectiveness of the grafting. (4)Postoperative Care: Close monitoring of the patient’s vital signs and wound recovery should be conducted after surgery to detect and manage possible complications in a timely manner. At the same time, patients should be guided to perform rehabilitation exercises to promote the recovery of ankle function.
In light of the advantages and limitations discussed above, several suggestions for improvement are proposed. These include optimizing the surgical procedure to reduce unnecessary operation time, enhancing preoperative assessment to ensure patient suitability, and providing detailed postoperative rehabilitation guidance to promote faster recovery. By implementing these suggestions, the clinical applicability and relevance of artificial dermis technology combined with full-thickness skin graft coverage can be further enhanced.
Conclusion
In conclusion, the treatment of elderly foot and ankle wound defects with artificial dermis technology combined with full-thickness skin graft coverage has demonstrated significant benefits in improving joint function, reducing pain, and promoting better wound recovery with fewer complications. Future research should aim to expand the sample size and further investigate the long-term effects and specific mechanisms of action of this treatment approachexploring ways to optimize the surgical procedure and material selection, and studying how to better combine rehabilitation treatment to further improve patients’ postoperative quality of life (Figure 2). Postoperative 6-month effect of artificial dermis technology combined with full-thickness skin graft coverage.
Footnotes
Author contributions
Qiang Xie and Wang Pei conceived the work, interpreted the data, and substantively revised the work. Wang Pei designed the work and substantively revised the work. Hao Yu and Li Xiao Dong analyzed and interpreted the data. Qiang Xie drafted the work. All the authors approved the submitted version and agreed to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.