
Abstract
Background:
Chronic Achilles tendinopathy following Haglund disease is a common ankle condition that is difficult to manage. In this study, we will compare the clinical outcomes of debridement and ostectomy with and without FHL tendon transfer in treating Haglund deformity.
Methods:
Forty eligible patients aged >50 years who did not respond to conservative treatment were randomly divided into 2 groups for surgical approach: using flexor hallucis longus (FHL) tendon transfer (FHL group) or “standard procedure” (control group). The main surgical treatment included debridement and ostectomy. AOFAS and VISA-A scores were obtained from all patients pre- and postoperatively.
Results:
Twenty patients were assigned to each of the 2 groups and were observed for at least 1 year. The American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot scores and the Victorian Institute of Sports Assessment self-administered Achilles (VISA-A) questionnaires scores improved more in the FHL group; however, the average difference in the change in scores did not reach the levels previously reported for minimal clinically important differences. Surgical complications and hallux function were not significantly different between the 2 groups.
Conclusion:
We found that FHL tendon transfer may improve the clinical outcome scores of Achilles tendon treatment in patients aged >50 years using debridement and ostectomy. However, tendon transfer increases the time of surgery and creates additional skin incisions, which may cause more short-term wound complications, and the significance of the differences in outcome improvement may not be clinically meaningful.
Level of Evidence:
Level II, grade A recommendation.
Keywords
Introduction
Chronic Achilles tendinopathy following Haglund deformity is a common ankle disorder. The Achilles tendon consists of gastrocnemius and soleus muscle fibers and acts as a plantar flexor of the ankle. 4 Blood supply is provided by the paratenon, but in cases of overuse, the blood flow to the area that is 2-6 cm proximal to the Achilles tendon insertion may alter. This may lead to inadequate vascular supply and subsequent damage and fibrosis of the affected tendon. 25 Occurrence of Achilles tendon tendinopathy can either be acute or chronic. Acute tendinopathy that is commonly known as tendonitis is a reversible condition, whereas chronic tendinopathy or tendinosis comes with irreversible fibrous degeneration.3,23
Haglund deformity is a condition where the back of the calcaneum sticks out and affects the bursa and the tendon that connect to the heel bone. 11 Surgical management is a good treatment option if conservative treatment fails in Haglund deformity, showing favorable results in the long term.8,12 Various surgical techniques have been implemented; however, none of these techniques currently stand out as superior to the rest. One common difference mentioned in the articles is how well the calcaneus exostosis is accessed and how much the tendon can be safely removed to ensure that it is not weakened afterward. Most studies show good to excellent outcomes; however, each of them has specific complications. 10
Flexor hallucis longus (FHL) tendon transfers are often performed to strengthen the final tendon structure by providing mechanical strength and improving vascular supply.17,18 It has been shown useful in 2 conditions: when debridement of >50% is required and in patients aged >50 years.15,21 In patients with advanced age, tendon repair or tendon transfer is mostly recommended. 7 Because of the lack of evidence, the choice of surgical technique is usually based on the surgeon’s personal opinion. 14 In this study, we will compare the clinical outcomes of debridement and ostectomy with and without FHL tendon transfer in treating Haglund deformity.
Material and Methods
Study Design
This study was a single-blinded randomized controlled trial (RCT). Conducting a double-blinded trial was not achievable because the surgeons knew the patients and the technique they used, but the patients were kept blind in the process.
Patient Selection and Randomization
Following the approval of the University Ethics Committee and obtaining informed consent, patients older than 50 years with a clinical diagnosis of Haglund disease who underwent at least 6 months of unsuccessful conservative treatment, including immobilization, a period of relative rest, shoe modification, nonsteroidal anti-inflammatory drugs, and physiotherapy were included. Patients were excluded if they were smokers or had diabetes mellitus, previous Achilles tendon surgery or injury, active wound, or infection in the ipsilateral leg that made the FHL tendon unsuitable for transmission. In the process of this study, once surgery was started, if we noticed that a patient in the debridement group had less than 50% of their tendon available, they would also be immediately excluded from the study, and the tendon transfer would be performed. After determining sample size using similar studies, 40 patients were allocated randomly into 2 groups based on FHL transfer (FHL group) or not (control group) using the block randomization method. Patients, all care providers, nurses, and analyzers were blinded throughout the study with the aid of an investigational nurse who randomly allocated patients in a 1:1 ratio. Stratified block randomization was used with a block size of 4.
Data Collection and Analysis
Patients’ demographics including height, weight, age, and preexisting conditions, were recorded. The American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot score and the Victorian Institute of Sports Assessment self-administered Achilles (VISA-A) questionnaires were obtained from all participants before and 1 year after the surgery. For statistical analysis, the amassed data were coded and entered into IBM statistical analysis software (SPSS), version 27.
Surgical Technique
Ostectomy and Debridement Procedure
After spinal anesthesia, the patient was placed in a prone position. A longitudinal incision was made 1-2 cm lateral to the Achilles extending 3-4 cm proximal and 2-3 cm to the upper calcaneus tuberosity. With mobilization of the tendon to the wide side, we were able to reveal the retrocalcaneal bursa and bony prominence. If there are osteophytes in the central part of the tendon, complete debridement of the tendon’s lesion including osteophytes is performed with removal of the retrocalcaneal bursa and Haglund deformity. The tendon is then reconnected.
FHL Tendon Transfer
In the prone position, a skin incision is made on the medial border of the Achilles tendon with an overall length of approximately 10 cm in the center of the tendon (Figure 1). The paratenon is cut, and any inflammatory peritonitis gets removed. The area of degeneration is debrided until only the normal tendon remains. For FHL transfer, a longitudinal incision is made just to the depth of the Achilles tendon. Neurovascular structures are protected between the FHL and the peroneal tendons. Once the FHL is identified, it passes within an intraosseous tunnel proximal to the sustentacular tali. The FHL tendon is released and transferred to the posterior incision of the leg (Figures 2 and 3). The FHL tendon is approximated to the Achilles tendon and then passed via the calcaneal bone tunnel and sutured to itself (Figure 4).

Medial view of ankle. Skin incision for flexor hallucis longus harvest is marked; the first metatarsus and medial malleoli are landmarks for this incision.

After the flexor hallucis longus tendon is identified, it is cut from the distal depending on the length required.

The incision on the Achilles tendon after debridement and ostectomy. The flexor hallucis longus tendon was transferred.

The calcaneus tunnel is prepared to reattach the flexor hallucis longus tendon.
Postoperative Care
We used nonweightbearing plaster for 3 weeks followed by a weightbearing plaster for another 3 weeks. At the end of 6 weeks, a prefabricated shoe was used for walking. Patients were advised to start active and inactive exercises and calf strengthening at this time. At 6-8 weeks postoperatively, patients removed their boots and began standardized physiotherapy. At 3 months, a calcaneus lift was used, and patients were allowed to return to their previous activities gradually. Patients were prohibited from traumatic exercise at least 3 months postoperatively.
Statistical Analysis
Quantitative variables are reported as mean ± SE, and Mann-Whitney U test, t test, and paired-samples t test were carried out for the comparison of these variables between the 2 groups. The chi-square test was used for qualitative variables. The normality of the distribution of the quantitative data was investigated by the Kolmogorov-Smirnov statistic. Any difference was considered statistically significant between the groups if P < .05.
Results
Of 47 patients with Haglund deformity, 5 patients were excluded from the study before surgery because of their request to withdraw from the study, and 2 patients were not available for 1-year follow-up (1 patient from each group). A total of 40 patients were included in this study including 20 patients in the control group and 20 patients in the FHL transfer group. The mean age of the patients was 60.7 years (range 50-75 years). Patients included 24 females and 16 males. The mean body weight was 83.2 ± 8 kg. The 2 groups were not different in terms of demographic variables and preoperative AOFAS and VISA-A scores (Table 1).
Demographic Variables. a

Data are reported as mean ± SD (95% CI).
AOFAS and VISA-A scores improved significantly both in the control and FHL groups in one year of follow-up (Tables 2 and 3). However, this improvement was significantly better in the FHL group (P < .001) (Figures 5 and 6). No subjective or objective restriction on metatarsophalangeal and interphalangeal plantar flexion was observed neither in the FHL nor control group at the one-year follow-up. Moreover, none of the patients complained of any functional problems or weakness in the hallux. No neurological complications or deep vein thrombosis were reported. While there were no differences between the groups regarding significant complications, we identified 5 minor complications related to surgical wounds which included partial opening of superficial damage (1 patient in the FHL group), blistering or skin cellulite (2 patients, 1 in each group), and delayed wound healing (2 patients in the FHL group). Finally, all of the patients’ wounds healed without additional surgical intervention.
Pre- and Postoperative Variables. a

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle hindfoot score; FHL, flexor hallucis longus; VISA-A, Victorian Institute of Sports Assessment self-administered Achilles questionnaire.
Data are reported as mean ± SD (95% CI), unless otherwise noted.
Comparing pre- and postoperative data in each group.
Postoperative Data. a

Abbreviations: AOFAS, American Orthopaedic Foot & Ankle Society ankle hindfoot score; FHL, flexor hallucis longus; VISA-A, Victorian Institute of Sports Assessment self-administered Achilles questionnaire.
Data are reported as mean ± SD (95% CI), unless otherwise noted.
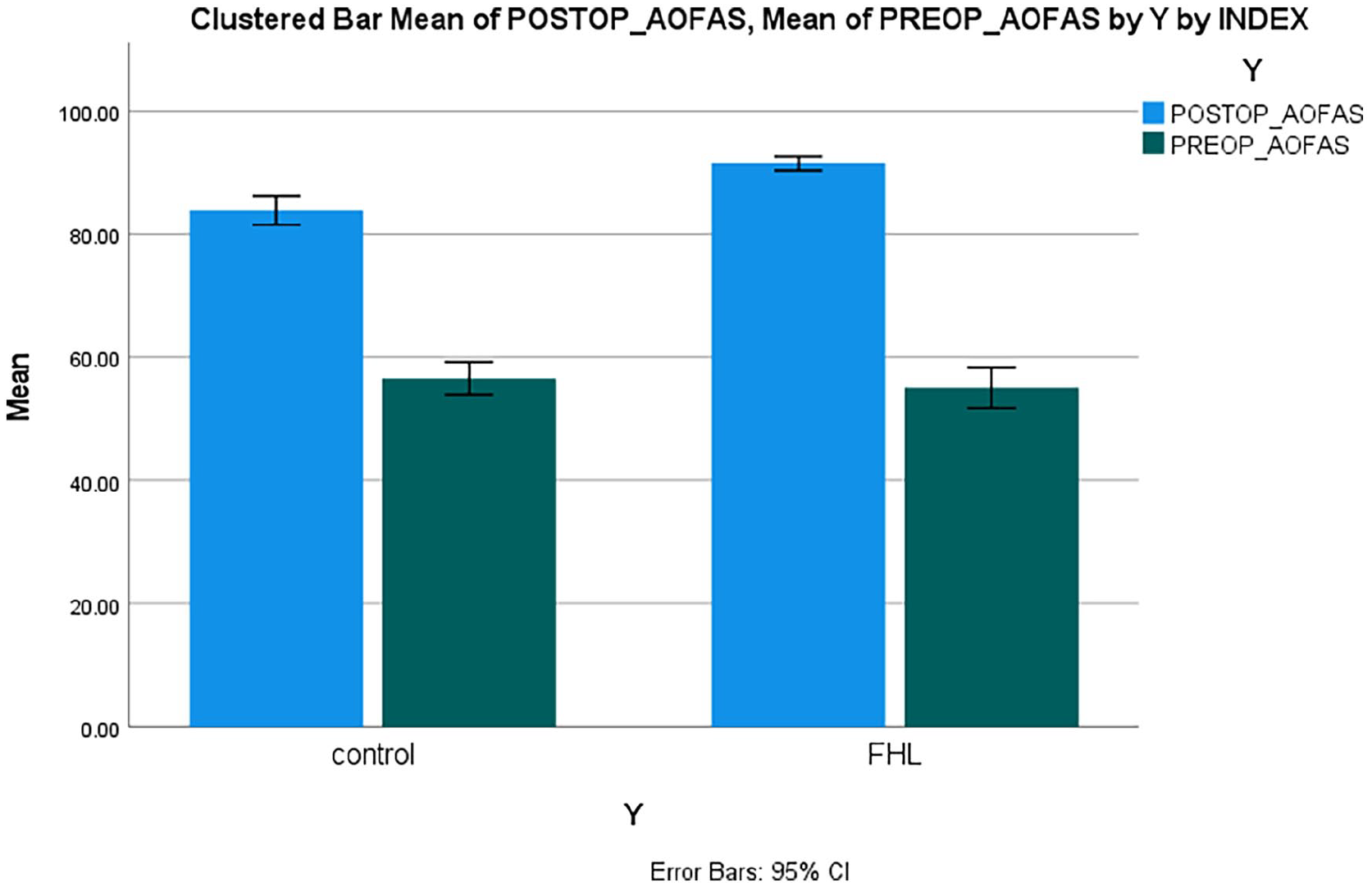
Comparison of pre- and postoperative American Orthopaedic Foot & Ankle Society (AOFAS) ankle hindfoot scores in patients.

Comparison of pre- and postoperative Victorian Institute of Sports Assessment self-administered Achilles questionnaire (VISA-A) scores in patients.
Discussion
However, tendon transfer may increase the time of surgery and create additional skin incisions, which may contribute to an increased risk for short-term complications of the wound. Although all wound-related issues healed without additional intervention and no neurovascular damage was reported, we feel that the extra skin incision and longer surgical time may play a significant role in increasing the risk of wound complications. FHL transfer did not appear to lead to poor flexion of the hallux foot compared with the control group according to clinical visits and patient reports.
Studies have introduced the FHL as an enhancer for chronic ruptures of the Achilles tendon.12,13 FHL has been shown to have more muscle mass and strength than the flexor digitorum longus (FDL) tendon and peroneal tendons, which have also been used to treat chronic Achilles disease. 1 Although many authors recommend FHL augmentation for Achilles tendinopathy, there are very few reports concerning patients aged >50 years.
Den Hartog et al 5 reported a higher recovery rate for 26 patients, including 18 who were aged >50 years. AOFAS scores in the ≥50-year age group showed good improvements. Our study, which also investigates the best option for patients older than 50 years, showed the same satisfaction with the performance improvement. However, unlike our study, the results of Den Hartog et al’s 5 study were retrospectively reviewed and were not compared with the control group. Elias et al reported 40 patients (mean age 57 years; range 39-76 years) who underwent Achilles debridement and FHL transfer for Achilles tendinopathy. 8
Improvement of VISA-A and AOFAS scores was observed without loss of plantarflexion strength. 8 Schon et al 21 reported significant improvement in physical function and pain relief in a group of 46 inactive, elderly, and overweight patients who underwent FHL transfer.
Theoretically, decreased strength of hallux plantar flexion may be a potential complication of FHL transmission that can affect balance, endurance, and gait.12,16,22 However, we did not find any clinical difference in hallux plantar flexion in patients who underwent FHL compared with controls in the 1-year follow-up period. This finding is similar to those reported in previous studies.1,2,16 One explanation for this unchanged flexion strength is that the power required for daily operation may be provided by the hallucis brevis flexor or distal connections between the FHL and FDL tendons. It is important to note that the patients we studied were 50 years of age or older and were obese on average. Younger and more active individuals may develop symptoms after FHL transmission, as the new evidence shows that these factors can contribute to Achilles tendinopathy.6,9
Although our patients had no neurologic complications and deep vein thrombosis, a relative rate of minor ulcer complications was reported. The present study’s complication rate (12.5%) is slightly higher than the rate reported in other studies, but no surgical intervention was needed.2,3,24 Using of tenodesis screw instead of a transosseous suture has been introduced as the less invasive FHL transfer that can reduce wound healing complications. 25 Using a single incision for short FHL transfer may be associated with lesser wound issues although this was not evaluated in the present study. 20
Tendon transfer increases the time of surgery and can create the need for additional or greater skin incisions. This will generally increase the risk of incisional complications, fortunately in our relatively small cohort, none of the patients needed secondary surgery.
Limitations
Our population was relatively small, so we suggest that future multicenter randomized studies should be carried out with a larger sample size than the present study to improve the study power. Another limitation was that our tools for this study were subjective to the patient and clinician and we were also unable to report the minimal clinically important difference, which has been reported to be between 12 and 20 for the VISA-A. So the value of the difference clinically remains unknown. 19 We suggest that future studies compare both techniques using specialized sports medicine equipment and measuring devices.
Conclusion
According to our results, FHL tendon transfer for Achilles tendon repair has better scores than debridement and ostectomy alone in patients >50 years of age although the actual clinical difference did not reach estimates of the minimum clinically important difference.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114241262783 – Supplemental material for Does FHL Tendon Transfer Alter the Outcome of Haglund Deformity Treatment by Using Debridement and Ostectomy in Patients Older Than 50 Years? A Single-Blinded Randomized Controlled Trial
Supplemental material, sj-pdf-1-fao-10.1177_24730114241262783 for Does FHL Tendon Transfer Alter the Outcome of Haglund Deformity Treatment by Using Debridement and Ostectomy in Patients Older Than 50 Years? A Single-Blinded Randomized Controlled Trial by Amir Sabaghzadeh, Naser Ghanbari, Hediye Gholamshahi, Amir Mohammad Zakeri, Saman Shakeri Jousheghan, Mohammadamin Aslani, Maryam Khoshkholghsima and Mohmmad Movahedinia in Foot & Ankle Orthopaedics
Footnotes
Ethical Approval
Ethical approval for this study was obtained from Institutional Review Board (IRB) of Shahid Beheshti Medical University (IR.SBMU.MSP.REC.1398.978)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosure forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.