
Abstract
Total knee arthroplasty (TKA) is an effective treatment for end-stage knee joint diseases. The debate over preserving or sacrificing the posterior cruciate ligament (PCL) in mobile-bearing TKA (MB TKA) still needs to be solved due to the lack of high-quality evidence, particularly meta-analyses comparing these techniques. This study aims to conduct a meta-analysis to compare the outcomes of PCL retention (CR) and PCL sacrifice (PS) in terms of clinical and functional knee scores, range of motion, complication rates, and revision rates and to validate these findings through animal experiments. A comprehensive search was conducted using MEDLINE, Cochrane, and Embase databases. Relevant studies were selected for the meta-analysis using RevMan 5.3. Additionally, an animal experiment using Sprague-Dawley rats simulated MB TKA to compare the effects of PCL retention and sacrifice surgeries. 12 studies were included in the meta-analysis. No significant differences were found between CR and PS techniques regarding HSS, KSS, KSFS, WOMAC, ROM, and medial/lateral instability. However, CR MB showed slight superiority in NKJS, while PS MB had better outcomes in complication and revision rates. In the animal study, CR rats exhibited significant early postoperative inflammation, but both groups’ knee structures gradually normalized. The meta-analysis indicates that PCL retention (CR MB) and sacrifice (PS MB) have similar effects on various clinical and functional knee scores. However, PS MB is significantly better at reducing complications and revision rates. The animal experiment confirms PS MB’s advantages in reducing inflammation and promoting joint recovery. Despite the strong evidence, long-term follow-up and larger-scale randomized controlled trials are necessary to confirm these findings.
Keywords
Introduction
Given the escalating aging trend in contemporary society, knee joint diseases have emerged as significant health issues adversely impacting the quality of life of elderly individuals worldwide.1–3 According to statistical data, tens of millions of patients worldwide suffer from knee joint diseases.4,5 Prolonged chronic pain and functional impairment not only cause physical distress to patients but also contribute to psychological problems like depression and anxiety.6–8 Hence, there is an urgent need for effective treatment methods to address this rapidly escalating public health issue.
Total knee arthroplasty (TKA) is a highly effective technique for managing advanced knee joint diseases.9–11 The debate regarding the involvement of the posterior cruciate ligament (PCL) in total knee arthroplasty (TKA) first centered on fixed-bearing (FB) primary TKA and has been the subject of extensive research over the years.12–15 The CR prosthesis can preserve joint proprioception, improve range of motion, and maintain joint function during movement by preserving the posterior cruciate ligament (PCL).16,17 Biomechanical studies have demonstrated that using PCL can effectively alleviate the pressure on the interface between implants and bones, thus enhancing implant durability by reducing polyethylene (PE) wear. 12 Nevertheless, some assert that prosthetic implants can enhance joint mobility. 18 This mechanism prevents issues such as slackness or excessive tension in the posterior cruciate ligament (PCL) and ensures a more dependable roll-back of the femur.19–22
The design movement mode of MB begins with pure rotation, which then transitions into pure translation and ultimately evolves into a combination of rotation and translation.13,23,24 The initial generation of the MB prosthesis, referred to as Low Contact Stress (LCS) and developed by Buechel and Pappas in 1977, was the invention of note. 25 Originally, its primary objective was to enhance the mobility and adaptability of the bearing surface while reducing constraint forces, contact stresses, and the risk of polyethylene wear and implant loosening in early implant designs. 24 Additionally, the axial rotation of the carrier enables self-adjustment of rotational misalignment in the tibial component. Later, other MB products appeared.26,27 All these systems consist of sub-components that can either preserve or sacrifice PCL. The research conducted on MB demonstrates both strong clinical efficacy and improved kinematic function.28–30
However, the differences between CR and PS in MB TKA are currently unclear due to limited literature supporting the superiority of CR MB over PS MB.31,32 A systematic review conducted in 2011 compared the overall clinical outcomes of medial ball-and-socket (MB) total knee arthroplasty (TKA). The review mainly included single-arm and indirect comparison trials, which limited the availability of sufficient data for directly comparing the effect of the posterior cruciate ligament (PCL) among various types of MB implants. 33 Therefore, more research is required to determine the clinical correlation differences between CR MB and PS MB. Since 2011, numerous randomized controlled trials and observational studies have been published, directly comparing the postoperative outcomes of CR MB and PS-MB.21,34–36 To resolve this controversy, this study aimed to directly compare the impact of preserving and excising the posterior cruciate ligament (PCL) on the postoperative outcomes in MB TKA.
Materials and methods
Guidelines for research design and methods
This study adhered to the PRISMA guidelines for conducting a systematic review and meta-analysis. 37 We established inclusion and exclusion criteria, gathered relevant studies from multiple databases, and subjected them to independent screening by two reviewers. The chosen studies conducted data extraction, computed effect sizes, and used a random effects model for meta-analysis, considering the heterogeneity among the studies. The analysis was conducted using specialized software, and the results were visualized following the PRISMA algorithm.
Research qualifications and standards
We conducted a screening of randomized controlled trials (RCTs) and comparative cohort studies involving adult patients who underwent total knee arthroplasty surgery. The surgical procedure should be specified as CR MB TKA or PS MB TKA, and the study should include follow-up data of more than 1 year. Additionally, it should report at least one of the following outcomes: clinical and functional knee joint scores, physical function, complication rate, or revision rate. We excluded case reports, commentaries, conference abstracts, and other non-original studies. Additionally, studies conducted in vitro or using biomechanical models were also excluded.
Furthermore, redundant publications and secondary analyses on identical datasets are also disregarded. Two independent reviewers conduct the filtering process. A third-party expert will be consulted for resolution in cases of differing opinions.
Literature retrieval, screening, and data extraction
We searched databases, including MEDLINE, Cochrane, Embase, and PubMed, to obtain published literature until October 2023. For the retrieval work, we employed keywords including ‘portable’, ‘total knee replacement’, ‘preservation of the posterior cruciate ligament’, ‘posterior stabilization’, ‘sacrifice of the posterior cruciate ligament’, ‘rotating platform’, ‘meniscal bearing’, and ‘anterior-posterior sliding rotation’, along with their corresponding synonyms. Furthermore, if there is a lack of literature, we also examined the relevant reference literature about comments.
Two independent reviewers did all the screening work. When authors encounter different opinions, they aimed to reach a consensus through discussions and negotiations. Initial screening aims to eliminate irrelevant literature and conduct preliminary screening through a review of the titles and abstracts. The remaining literature underwent additional full-text screening to determine its compliance with the above eligibility criteria. Furthermore, to prevent data duplication, we chose the literature presenting the most recent data and the longest follow-up when the author or institution reported multiple publications on the same patient group.
To gather comprehensive information, we conducted thorough examinations of each included study. The critical components of these studies encompass the principal author’s name, study design, prosthetic brand, ethnic background of the sample, follow-up duration, patient count, and number of knee joint implants. Additionally, the study examined the demographic characteristics of the patients, including gender, age, and BMI. Additionally, the research findings encompass various clinical and functional knee joint scores, including KSS, KSFS, NJKS, WOMAC, and HSS. They also encompass kinematic functions such as range of motion (ROM), knee joint flexion, flexion contracture, and varus-valgus laxity. Moreover, the study examined the complications and rate of repair during the final follow-up, all of which fell within the purview of this study. When encountering incomplete data in the research, such as when only medians, extremes, or quartiles are provided, we estimated the sample mean and standard deviation from the incomplete data only if we were unable to obtain the required original data by contacting the relevant authors. 38
Methodological quality assessment
In order to ensure the quality of the included studies, we systematically assessed the methodological quality of each study using the revised Coleman Methodology Score (MCMS). The MCMS was initially developed to assess the quality of randomized controlled trials (RCTs) for treating lateral epicondylitis. 39 Although originally designed for randomized controlled trials (RCTs) according to the CONSORT statement, it has been modified to incorporate other study designs, including case-control studies (CCS) and cohort studies (CS). The MCMS system utilizes a scoring range of 0 to 100 to thoroughly evaluate the methodological quality of research, encompassing 15 key criteria. High scores indicate that the research has a rigorous design, which can significantly decrease confounding factors and potential bias. The scoring system is categorized into four quality levels to enhance interpretation: scores ranging from 85 to 100 are deemed excellent, scores from 70 to 84 are considered good, scores from 55 to 69 are classified as reasonable, and scores below 54 are classified as poor. This evaluation method offers a clear and objective tool that aids our comprehension of each study’s relative strengths and potential limitations.
Evaluation of evidence level
To evaluate the reliability and quality of the studies included, we employed the 2011 grading system developed by the Oxford Centre for Evidence-Based Medicine to assess the level of evidence for each study. 40 This rating system categorizes evidence into four levels based on the strength and validity of the research design. Level I evidence represents the highest quality, typically derived from systematic reviews of randomized controlled trials undergoing extensive methodological screening and evaluation. Level II evidence comprises separate randomized controlled trials or observational studies. However, these observational studies should possess a significant effect size to guarantee the reliability of their findings. Grade III evidence is primarily obtained from non-randomized controlled cohort studies or other follow-up studies. Although these studies may have design limitations, they offer valuable evidence for addressing the research question. Level IV evidence is derived from case-control studies, case series, and historical control studies, which all have inherent limitations in establishing causal relationships. This method enables us to accurately and objectively assess the quality of evidence in each study, guaranteeing that the analysis is grounded on reliable scientific evidence.
Animal model construction
All animal experiments conducted in this study adhered to the guidelines for using and caring for animals provided by the NIH. Additionally, before they began, these experiments received formal approval from the Institutional Animal Ethics Committee. We guarantee that all animals receive appropriate care and humane treatment during experiments, and we make every effort to minimize pain and distress to the animals throughout the experimental process. A professionally trained team of veterinarians is responsible for the feeding and care of rats. We acknowledge the ethical responsibility of animal experimentation and are fully committed to adhering to the best practices when conducting experiments.
We formulated the following experiment to validate the conclusions derived from the meta-analysis concerning the rates of complications and revisions when comparing retained posterior cruciate ligament (PCL) versus sacrificed PCL in patients who underwent Mobile bearing total knee arthroplasty (MB TKA). A total of 60 adult Sprague-Dawley rats, weighing between 250 and 300 g, were selected for the study and sourced from China Viton Livestock Co., Ltd. All rats underwent a minimum 1-week adaptation period before the commencement of the experiment. The rats were divided randomly into three groups, each containing 20 rats. These groups include the control group without surgical intervention, experimental Group 1 with PCL retention (CR) surgery, and experimental Group 2 with PCL sacrifice (PS) surgery. This study aims to simulate MB TKA surgery using the miniature surgical tools manufactured by Aesculap AG. In the case of experimental Group 1, PCL preservation surgery was performed, while experimental Group 2 underwent PCL sacrificing surgery. The rats were anesthetized with 2% isoflurane from Baxter Healthcare throughout the surgical procedure. Additionally, local anesthesia was administered using 0.5% bupivacaine from Pfizer. 41
Methods for in vivo fluorescence imaging and microCT evaluation
The inflammation level, blood flow, and metabolic activity of surgical sites are assessed using PerkinElmer’s in vivo Imaging System (IVIS) through live animal fluorescence imaging. In this process, specific fluorescent dyes from Life Technologies are employed to label specific cells during inflammation and repair processes. Furthermore, the knee joint’s structure, particularly the bone and articular cartilage repair, was assessed utilizing Bruker’s Skyscan 1276 microCT. The scan parameters should be set to 50 kV and 200 μA using a 0.5 mm aluminum filter. The resolution of the reconstructed image is 10 μm/pixel. Post-operative appointments will be arranged at 1, 2, 4, and 8 weeks following the surgery. Fluorescence imaging and microCT scanning are conducted during each subsequent visit.42,43
Statistic analysis
We conducted a meta-analysis using RevMan 5.3 on the studies included. We employed heterogeneity tests, primarily utilizing indicators such as I2 and Chi2, to evaluate the differences among studies for the summary results. A high degree of heterogeneity between the studies is considered when the I2 value exceeds 50%. Given the potential heterogeneity among the studies, we opted for a random effects model to conduct the meta-analysis. Concurrently, employing comparable PCL processing methods, we conducted a sub-group analysis of data from different brands, focusing on CR MB or PS MB. The results of the meta-analysis present the effect sizes along with their corresponding 95% confidence intervals, representing the effects observed in each study and the summary results. In all statistical tests, we define statistical significance as a p-value less than 0.05. Additionally, we employed ANOVA to compare between groups and performed a post hoc analysis of group differences using Tukey’s multiple comparison test. 44
Results
Article screening and research inclusion
Basic characteristics of included studies.

BMI, Body Mass Index; CR, PCL-retaining group; PS, PCL-substituting group; ND, no data or unclear.
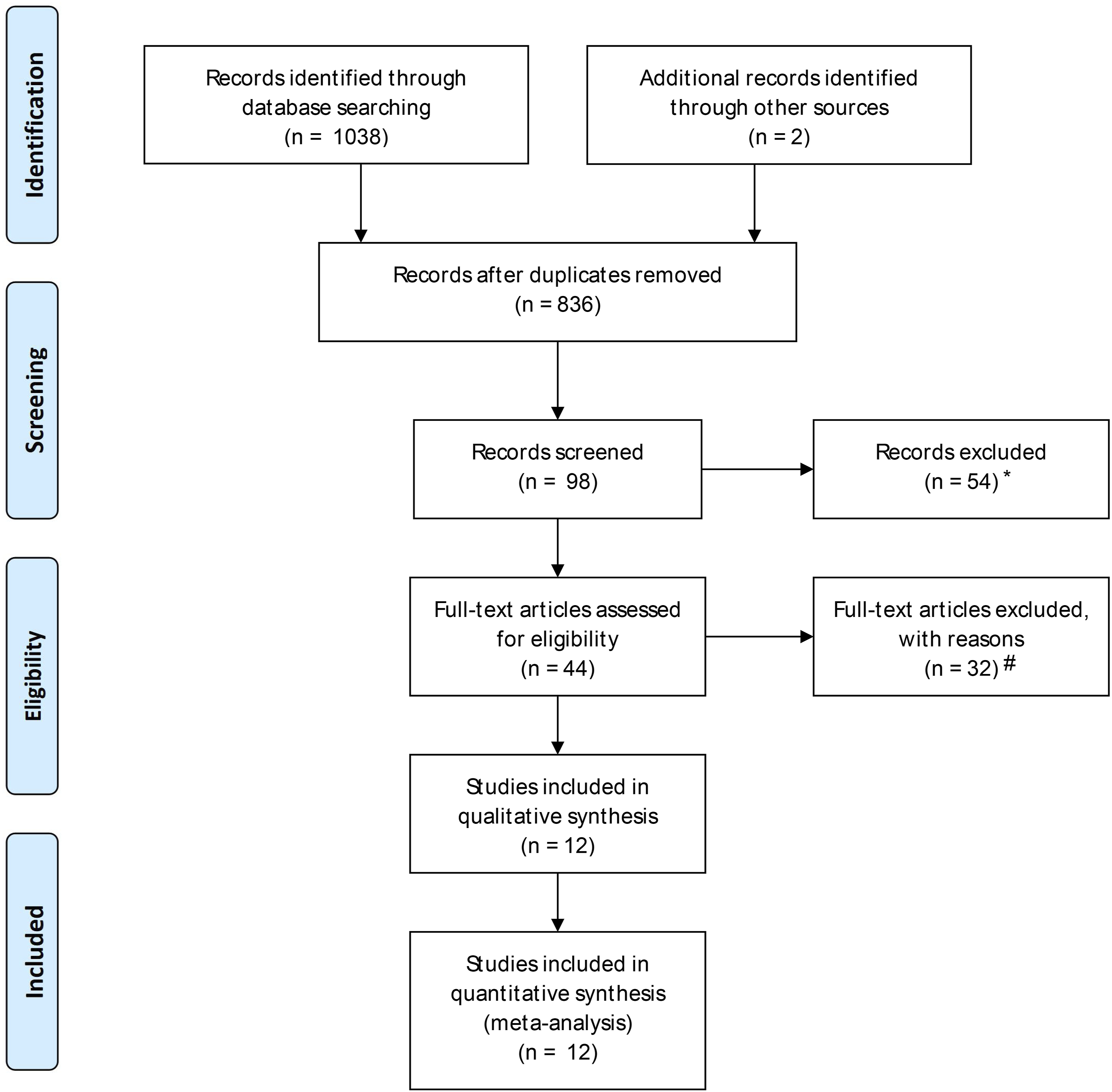
Flow diagram for the meta-analysis of included studies. Note: * Reasons for record exclusion include irrelevant topics and duplicate data. # Reasons for full-text exclusion include insufficient data, failure to meet inclusion criteria, and flawed study design.
Research quality and level of evidence
Outcomes of included studies.
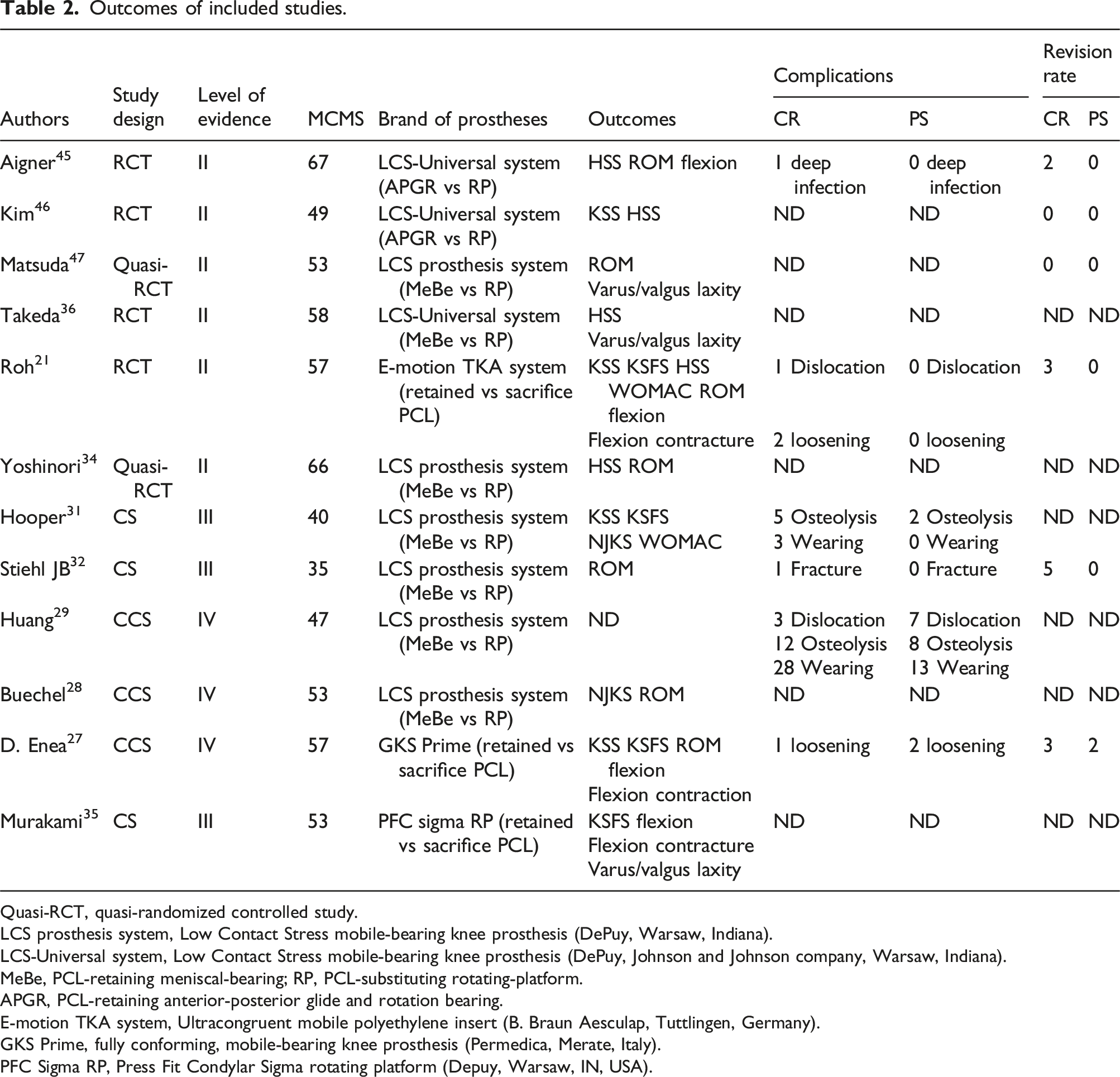
Quasi-RCT, quasi-randomized controlled study.
LCS prosthesis system, Low Contact Stress mobile-bearing knee prosthesis (DePuy, Warsaw, Indiana).
LCS-Universal system, Low Contact Stress mobile-bearing knee prosthesis (DePuy, Johnson and Johnson company, Warsaw, Indiana).
MeBe, PCL-retaining meniscal-bearing; RP, PCL-substituting rotating-platform.
APGR, PCL-retaining anterior-posterior glide and rotation bearing.
E-motion TKA system, Ultracongruent mobile polyethylene insert (B. Braun Aesculap, Tuttlingen, Germany).
GKS Prime, fully conforming, mobile-bearing knee prosthesis (Permedica, Merate, Italy).
PFC Sigma RP, Press Fit Condylar Sigma rotating platform (Depuy, Warsaw, IN, USA).
Furthermore, to obtain a more comprehensive comprehension of each study’s evidence level, we evaluated them using the 2011 grading system for levels of evidence established by the Oxford Centre for Evidence-Based Medicine. Of all the studies included, the evidence level for 6 studies was rated as level II, while 3 were rated as level III and another 3 were rated as level IV. The assessment results for these levels of evidence are also listed in Table 2, providing readers with a more transparent and more accessible reference.
The ROM data consists of 7 out of 12 studies, and it provides comprehensive analysis to generate a funnel plot for assessing publication bias. The funnel plot reveals asymmetry in the ROM data (I2 = 78%, p < 0.00001) (Figure 2). Therefore, RE models were used for statistical analysis. The asymmetry funnel plot for the knee ROM data.
Clinical and functional scoring
During our research, certain articles focused on scoring systems for clinical and functional knee joint conditions.21,27,28,31,34–36,45,46 This study utilized multiple scoring criteria, including the Knee Society Score (KSS), to assess the clinical and functional status of the knee joint comprehensively and systematically,21,27,31,46 KSFS,21,27,31,35 NJKS28,31 WOMAC score21,31 and HSS.21,34,36,45,46 Each of these rating systems possesses distinct evaluation criteria and focus, enabling us to gain a comprehensive and in-depth understanding of the functional status of the knee joint. The specific usage of each rating in different studies is described in Figure 3. Forest plots of the clinical and functional scores (Panel a-e). Note: (a) The meta-analysis of KSS; (b) The meta-analysis of KSFS; (c) The meta-analysis of NJKS; (d) The meta-analysis of WOMAC; (e) The meta-analysis, subgroup and sensitivity analyses of HSS.
Heterogeneity analysis of HSS scores
The meta-analysis of HSS revealed significant heterogeneity (χ2 value = 14.23, I2 = 72%, p = 0.007), as depicted in Figure 3(e). A random effects model was employed. We discovered Aigner 45 through subgroup and sensitivity analysis. The study is the primary reason for heterogeneity. However, excluding Aigner. 45 After the analysis, the heterogeneity results were as follows: Chi-square = 0.60, I-squared = 0%, p-value = 0.90 (Figure 3(e)-HSS subgroup) regarding Aigner. 45 After conducting a thorough research review, we discovered that the study’s shortest follow-up period may result in Aigner. 45 The HSS value is lower than in other related studies. CR MB performed slightly better than NJKS compared to PS MB (FE, MD = 2.58, 95% CI 0.25 to 4.90, p = 0.68). No significant differences were observed in terms of Harris Hip Score (HSS) (RE, MD = −0.23, 95% CI -1.86 to 1.40, p = 0.007), Knee Society Score (KSS) (FE, MD = 1.15, 95% CI -0.31 to 2.62, p = 0.98), Knee Society Function Score (KSFS) (FE, MD = 0.72, 95% CI -3.66 to 5.10, p = 0.90), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) (FE, MD = −0.69, 95% CI -3.92 to 2.55, p = 0.75).
Postoperative functional assessment
The functional activities were documented in nine studies, encompassing range of motion (ROM) (7, 12, 14, 15, 20, 22, 30), flexion (7, 12, 14, 23), flexion contracture (7, 14, 23), and varus-valgus laxity (22, 23, 24, 30). For detailed information on these results, please refer to Figure 4. The research findings demonstrate significant heterogeneity in the analysis of a range of motion (ROM) (Chi2 = 37.76, I2 = 84%, p < 0.00001) (Figure 4(a)-Total ROM) as well as flexion (Chi2 = 11.93, I2 = 75%, p = 0.008) (Figure 4(b)-Total flexion). The study utilized a random effects model, the RE model, to address this heterogeneity. Through subgroup and sensitivity analysis, Stiehl discovered that
32
heterogeneity is the primary factor contributing to the diversity observed in ROM analysis. After excluding this study, heterogeneity decreased significantly to Chi2 = 9.11, I2 = 45%, p = 0.10 (Figure 4(a) - ROM subgroup). In his research, Stiehl discovered that the CR group had a final postoperative range of motion (ROM) assessment of 120 ± 9.8, whereas the PS group had 108 ± 14.3. The mean difference (MD) value of this study is 11.4, which is significantly higher compared to findings in other studies on range of motion (ROM). Forest plots of kinematic function (Panel A-D). Note: (a) The meta-analysis, subgroup and sensitivity analyses of ROM; (b) The meta-analysis, subgroup and sensitivity analyses of knee flexion; (c) The meta-analysis of flexion contracture; (d) The meta-analysis and subgroup analyses of varus–valgus laxity.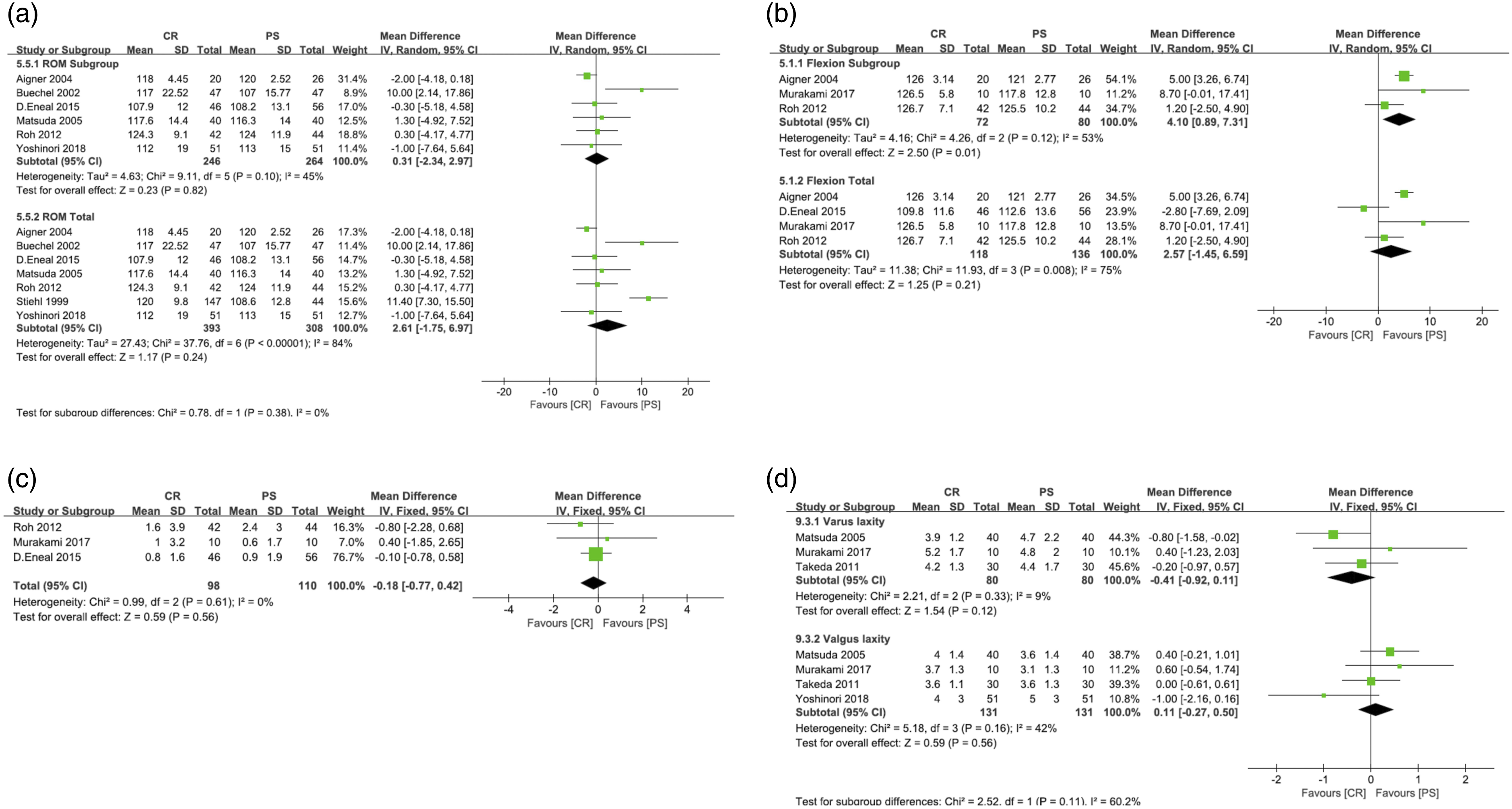
Reasons for heterogeneity in flexion analysis
Meanwhile, we found that D. Eneal’s study yielded similar results using the same method, 27 which contributing to the flexion analysis heterogeneity. After excluding this study, we observed a heterogeneity with Chi2 = 4.26, I2 = 53%, and p = 0.12 (Figure 4(b) Flexion subgroup). In D. Eneal’s study, 27 The author discovered that the prosthetic brand used was G.K.S. Prime, which exhibits distinctive characteristics in bending analysis. Various prosthetic designs can have varying effects on postoperative outcomes. Therefore, D. Eneal’s study 27 suggests that the distinctive design of the prosthetic limb is likely the primary factor contributing to the heterogeneity observed in flexion analysis.
Comparative analysis of sports functions
In summary, the results indicate that there is no significant difference between the two groups in terms of postoperative range of motion (ROM) (relative effect, mean difference = 2.61, 95% CI -1.75 to 6.97, p < 0.00001), knee flexion (relative effect, mean difference = 2.57, 95% CI -1.45 to 6.59, p = 0.008), knee flexion contracture (fixed effect, mean difference = −0.18, 95% CI -0.77 to 0.42, p = 0.61), medial laxity (fixed effect, mean difference = −0.41, 95% CI -0.92 to 0.11, p = 0.33), lateral laxity (fixed effect, mean difference = 0.11, 95% CI -0.27 to 0.50, p = 0.16), and subgroup difference tests: Chi2 = 2.52, I2 = 60.2%).
Comparison of complications and repair rate
The complication rate was reported in six studies,21,27,29,31,32,45 and the repair rate was reported in six studies.21,27,32,45–47 The incidence rate of complications is 2.09 times higher in CR MB compared to PS MB (Figure 5(a); p < 0.05, 95% CI 1.32 to 3.29). The repair rate ratio was 3.69 (Figure 5(B); p < 0.05, 95% CI 1.32 to 3.29). The results indicate that PS MB outperforms CR MB in terms of both complication incidence rate (FE, OR = 2.09, 95% CI 1.32 to 3.29, p = 0.89) and repair rate (FE, OR = 3.69, 95% CI 1.08 to 12.25, p = 0.82). Forest plots of complications rate and revision rate. Note: (a) The meta-analysis of complications rate; (b) The meta-analysis of revision rate.
The dynamics of inflammation and repair are illuminated through fluorescence imaging
In animal model experiments, we observed rat knee joints’ inflammatory response and repair dynamics at various time points after surgery using live animal fluorescence imaging. Figure 6(a) shows the results of fluorescence intensity (INF) normalization, indicating the measurement taken 30 min after the intravenous administration of TSC to the ankle joint before treatment. Group animals based on clinical arthritis scores. During the initial week following surgery, rats subjected to the CR technique exhibited notable inflammation at the knee joint. It was accompanied by significantly elevated fluorescence intensity compared to rats treated with the PS method and the control group that did not undergo surgery. By the second week, although the inflammation response in the CR group had reduced, its fluorescence intensity remained slightly higher than that of the PS group and the control group. By the fourth week, the inflammatory response in both the CR and PS groups had significantly decreased. However, the CR group still exhibited slightly higher fluorescence intensity. By the eighth week, the inflammation responses in both the CR and PS groups had subsided, resembling the control group that did not undergo surgery, indicating a favorable healing trend (Figure 6(b)). In vivo fluorescence imaging of the inflammatory response and repair dynamics in a mouse knee joint model after surgery. Note: (a) Line chart of normalized fluorescence intensity (INF) results from small animal in vivo fluorescence imaging; (b) In vivo fluorescence imaging of rat knee joints at different postoperative time points. After the first week, the inflammation induced by the CR method was evident, with significantly higher fluorescence intensity compared to the PS method and the control group. After the second week, the inflammation in the CR group reduced, but the fluorescence intensity remained slightly higher than in the PS and control groups. After the fourth week, both the CR and PS groups experienced a significant reduction in inflammation. However, the CR group still exhibited slightly higher fluorescence intensity. After the eighth week, the inflammatory response in both the CR and PS groups subsided, similar to the control group, indicating a repair trend.
Structural changes and repairs revealed by microCT
We investigated the structural changes and repair processes in the knee joints of rats at various time points post-surgery using microCT imaging (Figure 7). During the initial week following surgery, rats subjected to the CR method exhibited more significant structural alterations in the knee joint, particularly at the bone-cartilage junction, indicating the initial surgical impact and tissue stress. During the subsequent week, while some relief from the structural changes was observed in the CR group, these changes remained more substantial than those of the PS group. By the fourth week, a significant reduction in structural changes at the bone and cartilage junction of the CR group had occurred, although some minor irregularities can still be observed. In contrast, the knee joints of the PS group have exhibited satisfactory recovery at this specific time. In the eighth week of observation, the knee joint structure in the CR group has nearly returned to normal, although it still exhibits slight roughness compared to the PS group. The knee joint structure of the PS group has fully recovered, exhibiting robust biocompatibility and repair capability comparable to that of the non-surgical control group. Observation of structural changes and repair processes in rat knee joints after microCT surgery.
Discussion
Total knee arthroplasty (TKA) is widely recognized in the medical field as an effective intervention for end-stage knee joint disease. 48 This surgical procedure has the potential to greatly enhance patients’ quality of life, lessen pain, and restore joint functionality. Nevertheless, there remains a debate regarding the treatment of the posterior cruciate ligament (PCL) in mobile-bearing total knee arthroplasty (MB TKA).49–51 Several studies present arguments in favor of preserving the Posterior Cruciate Ligament (PCL) to ensure joint stability, while others advocate sacrificing the PCL to improve surgical outcomes and joint mobility. The study comprised 12 direct comparative research studies, with an additional 5 studies included.21,27,34–36 This method can be utilized to conduct a comprehensive comparison between CR MB and PS MB. Compared to previous meta-analyses, 33 This study directly explores the topic. Following a thorough analysis, we concluded that there were no significant differences between CR MB and PS MB in various scoring and functional measures, including HSS, KSS, KSPS, WOMAC, and ROM. Although CR MB has a higher NJKS score, PS MB and CR MB have demonstrated significant advantages in complication and repair rates.
Our study offers a more thorough analysis in comparison to the existing literature. Past studies, including the research conducted by Buechel and Huang, have demonstrated that PS MB offers benefits in terms of both postoperative complication rates and repair rates.28,29 It is consistent with our findings. However, the variation in follow-up duration and underreporting of complications and repair rates in certain studies can potentially affect the final analysis results.28,34–36,46,47 Our research has multiple clear advantages. An extensive literature search was performed, encompassing various databases such as MEDLINE, Cochrane, and Embase, to ensure the incorporation of all pertinent English studies. Secondly, we exclusively incorporated studies that directly compared CR MB and PS MB, eliminating the influence of single-arm trials and indirect comparative studies. Finally, this study presents a comprehensive and detailed meta-analysis that includes multiple data sources such as clinical and functional scores, kinematic characteristics, complication rates, and the success rate of MB TKA. Our animal experiments have provided substantial evidence to support clinical trials. We observed differences in the inflammatory response and joint structure recovery between the CR and PS methods through surgical procedures performed on Sprague-Dawley rats. This preliminary evidence further supports the conclusion of our meta-analysis, suggesting that the PS MB method may have certain advantages over the CR MB method.
Although our research holds significant scientific value, it is not without limitations. For instance, the initial limitation of our analysis is the relatively limited number of studies included, which may not provide a comprehensive representation of all patients undergoing total knee arthroplasty (TKA). Secondly, while animal experiments offer valuable data, it is important to acknowledge the existence of physiological and anatomical differences between rats and humans. These disparities could potentially affect the interpretation and application of experimental results. Not all high-quality studies were included in the meta-analysis. Current meta-analyses have been unable to provide reliable evidence due to the limited quality of evidence from some studies.
Furthermore, the choice of language could be biased due to exclusively including studies published in English. Moreover, various literature sources emphasize diverse methods of comparison, thus potentially influencing the interpretation and application of the findings. Based on current research evidence, we conclude that there are no significant differences in the knee joint scoring system and kinematic characteristics between the CR MB and PS MB. However, PS MB offers notable benefits in terms of complication and repair rates (Figure 8). To keep or to sacrifice: Assessing the impact of posterior cruciate ligament in mobile-bearing total knee arthroplasty.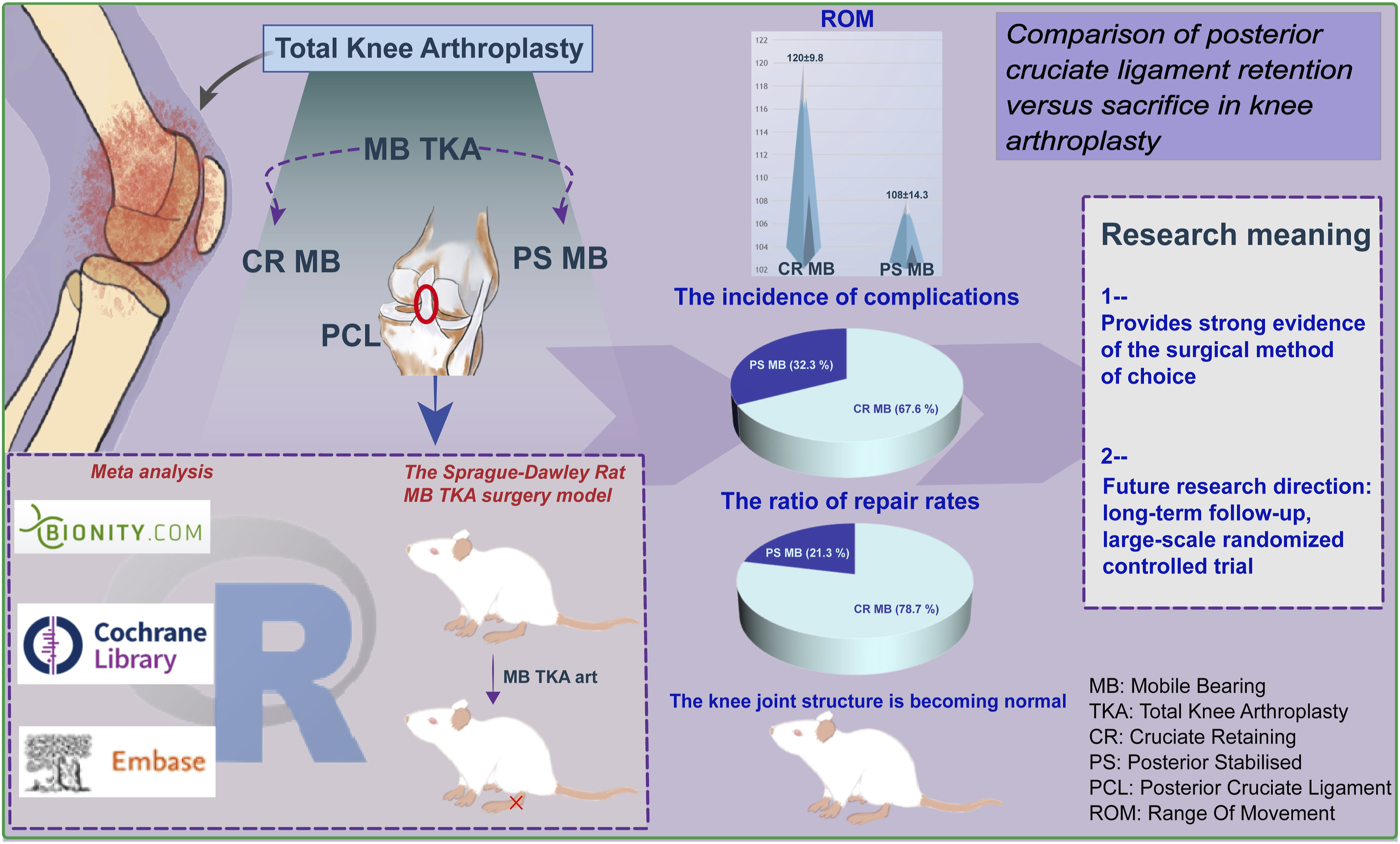
Overall, this study offers robust scientific evidence for managing the posterior cruciate ligament in total knee arthroplasty. These discoveries have not only enhanced our understanding of total knee arthroplasty (TKA) but have also provided valuable references for healthcare professionals. However, due to the limitations of this study, we advocate for additional long-term follow-up and high-quality randomized controlled trials to provide further insight into the most effective treatment approaches. Additional, thorough research will be necessary to establish the most effective treatment approach.
Footnotes
Authors’ contributions
Yuan-shi Zhang conceived and designed research. Hao-yu Li performed experiments. Lei Zhai interpreted the results of the experiments. Gui-zhou Zheng analyzed the data. Hong-bo Xing prepared figures. Shi-xin Du drafted the paper. Xue-dong Li edited and revised the manuscript. All authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and confidentiality agreements with the participants but are available from the corresponding author on reasonable request.