
Abstract
Purpose
The efficacy and safety of tourniquets use during total knee arthroplasty (TKA) in patients with osteoarthritis remain debated. This updated systematic review and meta-analysis aimed to further evaluate the role of tourniquets use in patients undergoing TKA for knee osteoarthritis by introducing trial sequential analysis.
Methods
PubMed, Embase, and the Cochrane Library were searched. We used the Cochrane risk of bias tool for quality assessment. Statistical heterogeneity across studies was evaluated using Cochran’s Q and I 2 statistic. Meta-analysis was performed using Stata/SE 14.0, and trail sequential analysis was performed using TSA software version 0.9.5.10 Beta. In addition, qualitative summary was also used to describe results.
Results
15 randomized controlled trials (RCTs) involving 1202 patients were included in the meta-analysis. The pooled results showed that tourniquet use during TKA significantly reduced intraoperative blood loss (mean difference (MD)= −123.84, 95% confidence interval (CI): −163.37 to −84.32, p < .001)and shortened operation time (MD = −4.71, 95% CI: −7.6 to −1.82, p = .001), but there were no significant differences in postoperative blood loss, calculated blood loss, total blood loss, transfusion rate (p = .939), and deep venous thrombosis (DVT) rate between the tourniquet and no-tourniquet groups. TSA confirmed that the result of operation time was false positive, but the results of other outcomes were conclusive. The results of qualitative summary showed conflicting findings in terms of pain, range of motion (RoM) and swelling ratio between the two groups.
Conclusions
Tourniquet use in patients receiving TKA for osteoarthritis benefits to reduce intraoperative blood loss but has no effect on postoperative blood loss, calculated blood loss, total blood loss, operation time, transfusion rate, and DVT rate. In addition, it remains unclear the difference between the tourniquet and non-tourniquet groups in terms of pain, RoM and swelling ratio.
Introduction
In 1973, the modern era of total knee arthroplasty (TKA) began with the introduction of the total condyle prosthesis designed by Insall et al. 1 With the development of technology and equipment, TKA has become one of the most used orthopedic procedures. Due to the increasing demand for TKA, there are an estimated 700,000 TKA cases per year in the United States alone. By 2030, this demand is expected to increase by more than 3.48 million cases. 2 TKA cases in mainland China increased from 53,880 in 2011 to 374,833 in 2019, revealing a 5.9-fold increase. 3
TKA is usually performed with the help of a tourniquet around the thigh. During the whole or part of the procedure, tourniquets are used to apply high pressure around the legs. Intraoperative tourniquet is a common practice during TKA because it improves visibility of the surgical field, reduces intraoperative blood loss, shortens operation time, and promotes bone cementing. Nevertheless, the efficacy and safety of tourniquets use in TKA remains controversial. Recent studies have not observed any significant differences between techniques, raising questions about advantages, such as reduced blood loss. 4 If a tourniquet is used for prolonged duration during the operation, it can lead to ischemia and mechanical trauma that can lead to serious complications such as nerve damage, postoperative wound hypoxia, joint stiffness, swelling, and postoperative pain. 5
Several randomized controlled trials (RCTs) with small sample sizes have compared the efficacy of tourniquet use with non-tourniquet during TKA, but have reached conflicting conclusions.5–9 To date, multiple meta-analyses10–12 have investigated the efficacy and safety of tourniquet use during TKA; however, combining data from patients with different primary diseases significantly compromised the reliability of their findings, as different primary diseases may contribute to the incidence of complications and bias. Therefore, Cai et al. 13 performed a meta-analysis to determine the efficacy and safety of using a tourniquet or not during TKA in patients with osteoarthritis, and found that tourniquet use significantly decreases intraoperative blood loss, calculated blood loss, and operation time but does not significantly decrease transfusion rate or the incidence of DVT. However, due to some limitations, the authors suggest that more studies are needed to further investigate this topic, and that several new RCTs7–9,14 with conflicting results have also been published following the publication of the previous meta-analysis.
Therefore, we performed this updated meta-analysis to further evaluate the efficacy and safety of tourniquet use during TKA in patients with osteoarthritis. Furthermore, we performed trial sequential analysis to assess whether definitive conclusions could be drawn based on currently available evidence.
Material and methods
Search strategy
According to the Guidelines for the Preferred Reporting Project for System Reviews and Meta-Analysis (PRISMA), two researchers independently conducted a systematic search in PubMed, Embase, and the Cochrane Library for eligible articles published before June 2022, using “total knee arthroplasty,” “TKA,” “total knee arthroplasty,” “TKR,” and “tourniquet.” When appropriate, additional relevant material checks were performed on all abstracts, studies, and citations. No language restrictions were imposed.
Selection criteria
Studies that met the following criteria were considered eligible: (1) patients were diagnosed with knee osteoarthritis; (2) patients were assigned to receive primary TKA; (3) patients in the study group received the use of tourniquet and those in the control group received non-use of tourniquet; (4) only RCTs published in English language were considered eligible. Abstracts, case reports, case series, opinion articles, and animal studies were excluded. In addition, we excluded repeated reports published by the same research group based on the same patients if they were determined to have poor quality and insufficient data.
Data extraction and quality assessment
Two researchers independently read the full text of selected eligible studies and extracted the following data from each study: author, country, publication year, age, proportion of males and females, sample size, body mass index, tourniquet pressure, and outcomes. The quality of eligible RCTs was evaluated using the Cochrane risk assessment tool with the following items: random sequence generation, allocation concealment, blinding of subjects and personnel, blinding of outcomes assessment, incomplete results, selective reporting of data, and other bias sources. The bias of individual study would be rated as “high’, “unclear’, or “low” risk according to the assessment criteria.
Statistical analysis
STATA 14.0 (StataCorp LP, College Station, TX, USA) was used for this meta-analysis. The effect sizes of the continuous variables were expressed as mean difference (MD) with 95% confidence interval (CI). The effect sizes of dichotomous variables were expressed as risk ratio (RR) with 95% CI. Cochran’s Q and I 2 statistics were used to examine statistical heterogeneity across studies. We selected the random-effects model for meta-analysis if statistical heterogeneity between studies was detected (p < .1 or I 2 ≥ 50%). On the contrary, we selected the fixed-effects model for meta-analysis if statistical heterogeneity was insignificant (p ≥ .1 or I 2 < 50%). In addition, sensitivity analysis was performed to ensure the robustness of the results using the leave-one-out method. In addition, we also used qualitatively strategy to summarize results when data were not applicable for quantitative synthesis. The Begg’s and Egger’s tests were used to evaluate the publication bias, and p > .05 indicated no significant publication bias.
Trial sequential analysis
Meta-analyses may accumulate too few participants to yield sufficient statistical power to reliably assess intervention effects. Even with statistically significant results, the credibility is poor when there are too few participants, and intervention effects may be overestimated or underestimated. Furthermore, repeated meta-analyses may increase the risk of type 1 errors. Therefore, to control the risk of random errors, trial sequential analyses (TSA) will be performed on all results. For continuous outcomes, we will use an alpha of 5%, beta of 20%, variance and diversity as suggested by the meta-analysis. For dichotomous outcomes, an alpha of 5%, beta of 20%, proportion at risk in the control group and diversity as suggested by the meta-analysis.
Results
Study selection and characteristics
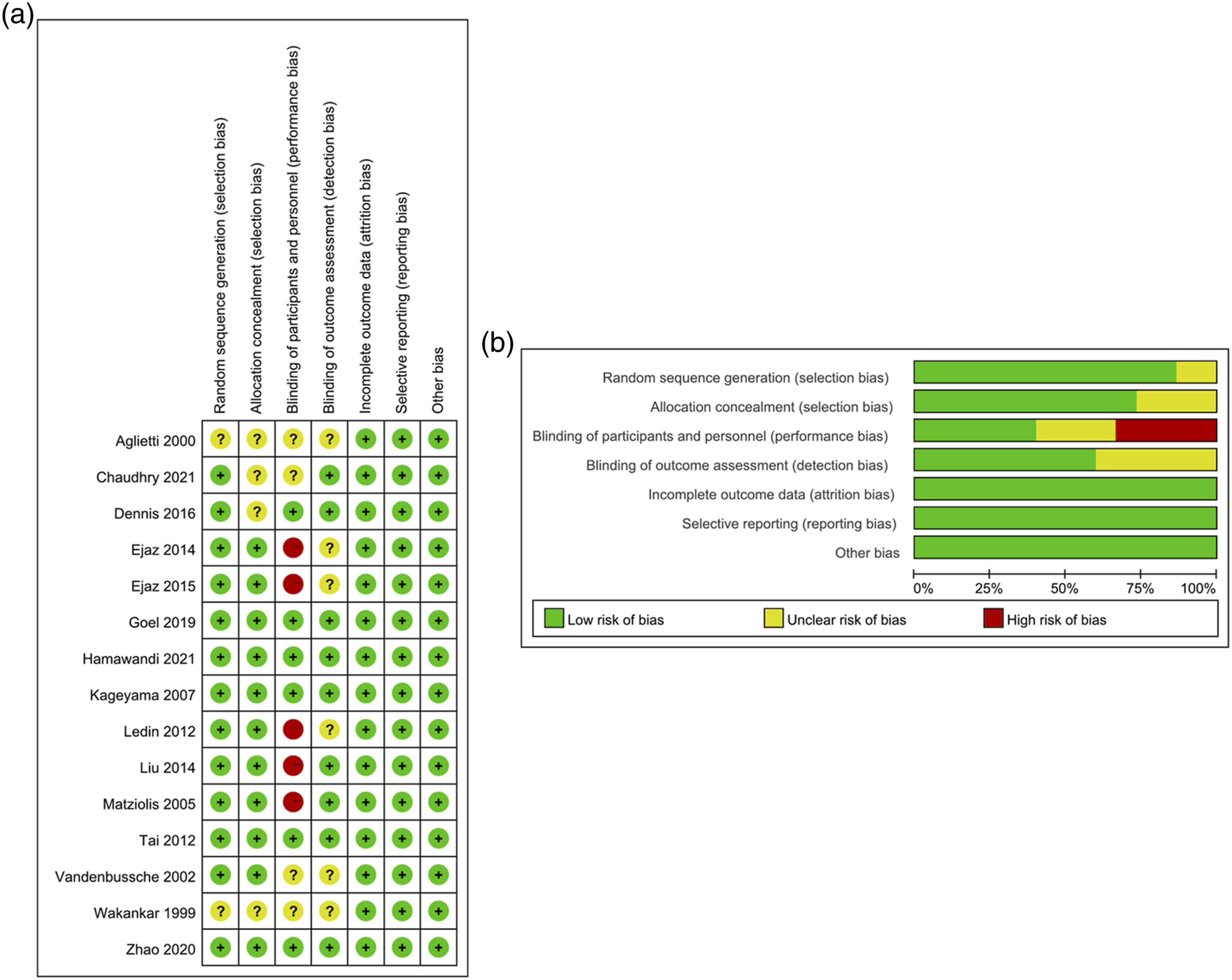
In the initial search, we identified 561 eligible articles. Three additional studies were identified through manual review of reference lists. After removing duplicate studies, 414 articles were screened by title and abstract. Then, 30 full-text reports were evaluated. Finally, after evaluating their eligibility of the remaining studies based on the full text screening, 15 studies were considered eligible.5–9,14–23 The literature search and screening process is shown in Figure 1. The characteristics of the RCTs are listed in Table 1. All eligible studies were conducted between 1999 and 2021, with a total of1202 patients (598 patients in the tourniquet group and 604 patients in the no-tourniquet group). Two RCTs were conducted in the UK, two in China, two in Denmark, two in the USA, and others in Italy, France, Germany, Japan, Sweden, Australia, and Iraq. In addition, a risk map of bias was generated to identify the risk of bias for each RCT, which was expressed as a percentage of all included studies and showed the risk of bias for each included study (Figure 2). The risk-of-bias graphs indicated that all studies had a low risk of bias in attrition, reporting, and other biases, while a high risk of bias was mainly observed in the performance in five studies, and an unclear risk of bias was observed in the selection, performance, and detection bias. Flowchart of the identification of the studies. Characteristics of the studies included in this meta-analysis. UK, the United Kingdom; T, tourniquet; NT, no tourniquet; SBP, systolic blood pressure; RCT, randomized controlled trial; IOBL, intraoperative blood loss; POBL, postoperative blood loss; CBL, calculated blood loss; TBL, total blood loss; OT, operation time; TT, transfusion rate; DVT, deep venous thrombosis; NA, not available. Risk of bias assessments for the randomized trials included in the meta-analysis. (a) Risk of bias summary; (b) Risk of bias graph. Symbols. (+): low risk of bias; (?): unclear risk of bias; (-): high risk of bias.

Quantitative synthesis
Intraoperative blood loss
Eight trials reported intraoperative blood loss with and without use of tourniquet during TKA. There was significant statistical heterogeneity between studies (p < .001, I
2
= 98.3%), therefore, a random-effects model was selected for meta-analysis. Pooled result showed that use of tourniquet significantly reduced intraoperative blood loss compared with nom-use of tourniquet (MD = −123.84, 95% CI: −163.37 to −84.32, p < .001) (Figure 3(a)). As shown in supplementary Figure 1(a), after adding the third study to the meta-analysis, the Z-curve crossed the TSA monitory boundary. Furthermore, the accumulative sample size also exceeded the required information size (n = 291). Therefore, no additional studies are required to further evaluate the effect of tourniquet use on intraoperative blood loss. Forest plots showing the blood loss in total knee arthroplasty with and without a tourniquet. (a) Intraoperative blood loss; (b) Postoperative blood loss; (c) Calculated blood loss; (d) Total blood loss.
Postoperative blood loss
Three trials reported postoperative blood loss with and without use of tourniquet during TKA. Significant statistical heterogeneity between studies was detected (p < .001, I 2 = 92.4%), therefore, a random-effects model was chosen for meta-analysis. Pooled result showed no statistical difference in postoperative blood loss between the use of tourniquet and the non-use of tourniquet groups (MD = 49.33, 95% CI: −54.53 to 153.19, p = .352) (Figure 3(b)). As shown in supplementary Figure 1(b), although the cumulative sample size was significantly smaller than the required amount of information (n = 3657), the Z-curve located in the infertile area. Therefore, no additional studies are required to further evaluate the effect of tourniquet use on postoperative blood loss.
Calculated blood loss
Six trials reported calculated blood loss with and without use of tourniquet during TKA. Significant statistical heterogeneity between studies was detected (p < .001; I 2 = 96.5%), so we selected the random-effects model for meta-analysis. Pooled result showed no statistical difference in calculated blood loss between the use of tourniquet and the non-use of tourniquet groups (MD = −57.34, 95% CI: −225.52 to 110.83, p = .504) (Figure 3(c)). As shown in supplementary Figure 3(c), trial monitory boundaries were ignored due to too little information was accumulated; however, the Z-curve located in the infertile area. Therefore, no additional studies are required to further evaluate the effect of tourniquet use on calculated blood loss.
Total blood loss
Three trials reported total blood loss with and without use of tourniquet during TKA. Significant statistical heterogeneity between studies was detected (p = .004; I 2 = 82%); therefore, we selected the random-effects model for meta-analysis. Pooled results did not show statistical difference in the total blood loss between the use of tourniquet and the non-use of tourniquet groups (MD = 17.56, 95% CI: −140.44 to 175.57, p = .828) (Figure 3(d)). As shown in supplementary Figure 4(d), trial monitory boundaries were ignored due to too little information was accumulated; however, the Z-curve located in the infertile area. Therefore, no additional studies are required to further evaluate the effect of tourniquet use on total blood loss.
Operation time
13 trials reported the operation time for TKA with and without use of tourniquet. Since significant statistical heterogeneity between studies was found (p < .001; I
2
= 88.4%), a random-effects model was chosen for meta-analysis. Pooled result showed that the use of tourniquet was associated with shortened operation time compared with non-use of tourniquet (MD = −4.71, 95% CI: −7.6 to −1.82, p = .001) (Figure 4(a)). As shown in supplementary Figure 2(a), although the accumulative sample size was significantly smaller than the required information size (n = 1906), the Z-curve did not cross the TSA monitory boundary after adding the latest study to the meta-analysis, indicating that conventional meta-analysis yielded a false positive result. Forest plots showing the effect of total knee arthroplasty with and without a tourniquet. (a) Operation time; (b) Transfusion rate; (c) DVT rate.
Transfusion rate
Eight trials reported the transfusion rate with and without use of tourniquet during TKA. There was no significant statistical heterogeneity between studies (p = .544, I 2 = 0%), so we selected the fixed-effects model for meta-analysis. Pooled result showed no statistical difference in transfusion rate between the two groups (RR = 1.02, 95% CI: 0.65–1.58, p = .939) (Figure 4(b)). As shown in supplementary Figure 2(b), although the accumulative sample size exceeded the required information size (n = 310), the Z-curve located in the infertility area, confirming that the use of tourniquet did not have effect on transfusion rate.
Deep venous thrombosis rate
Five trials reported the Deep venous thrombosis (DVT) rate with and without use of tourniquet during TKA. There was no significant statistical heterogeneity between studies (p = .784, I 2 = 0%), therefore, we selected the fixed-effects model to conduct meta-analysis. Pooled result showed no statistical difference in DVT rate between the two groups (RR = 2, 95% CI: 0.7–5.75, p = .197) (Figure 4(c)). As shown in supplementary Figure 2(c), although the accumulative sample size exceeded the required information size (n = 248), the Z-curve located in the infertility area, confirming that the use of tourniquet did not have effect on DVT rate.
Sensitivity analysis
The impact of the individual datasets was evaluated on the pooled effect by the sequential removal of each dataset and recalculating the pooled results of the remaining studies. The sensitivity analyses of the intraoperative blood loss, operation time, and transfusion rate showed that excluding any single RCT did not exert a significant impact, and the results were stable (Figure 5(a)–(c)). Sensitivity analysis for examining the influence of individual studies on pooled results of total knee arthroplasty with and without a tourniquet. (a) Intraoperative blood loss; (b) Operation time; (c) Transfusion rate.
Qualitative summary
Pain
Of all the tests included in this systematic review, 10 reported data on pain, and the time point at which pain was assessed ranged from the first postoperative day to 6 months postoperatively. Overall, 40% (4 trails) of these 10 trials showed no statistical difference in pain between the tourniquet and non-tourniquet groups throughout the assessment period; however, another 40% (4 trails) showed higher pain in the tourniquet group than in the non-tourniquet group in the short postoperative period (<6 weeks). In addition, 20% (2 trails) of trials showed that non-tourniquets were associated with pain in the short post-operative period (<6 weeks) compared to tourniquets; however, this difference between the two groups disappeared over time.
ROM
Of all eligible trials, 11 reported data on RoM, with the time point for evaluating RoM ranging from the first postoperative day to 2 years postoperatively. Specifically, 63.6% (7 trials) of the trials showed that patients in the tourniquet-free group had better RoM for a short period of time (<3 weeks) than the tourniquet group; however, the difference between the two groups became insignificant as the follow-up time increased. In addition, 27.3% (3 trials) showed no statistical difference in RoM between the two groups throughout the assessment period. Notably, 9.1% (1 trial) of trials showed that tourniquet application was associated with improved RoM compared to non-tourniquet application and this benefit was retained until 2 years postoperatively.
Swelling ratio
Of these eligible trials, six reported swelling rates, with the assessment of swelling occurring between the first postoperative day and 6 months. These six trials reported conflicting results. 66.7% (4 trials) assessed short-term swelling rates. Of these, two trials showed that no tourniquet was associated with a lower short-term swelling ratio compared to a tourniquet, but one of these trials showed that the benefit of no tourniquet would disappear at 3 months postoperatively. In addition, one trial showed similar short-term swelling ratios in both groups, but another trial showed that tourniquets were superior to non-tourniquets in terms of short-term swelling ratios. In addition, 33.3% (2 trials) showed comparable swelling ratios between the two groups throughout the assessment period of 1 week to 6 months postoperatively.
Publication bias
Publication bias was evaluated using Begg’s and Egger’s tests. Neither of the tests revealed any publication bias for intraoperative blood loss (p = .71 for Begg’s test, p = .97 for Egger’s test), postoperative blood loss (p = 1.00 for Begg’s test, p = .75 for Egger’s test), calculated blood loss (p = 1.00 for Begg’s test, p = .58 for Egger’s test), total blood loss (p = .30 for Begg’s test, p = .05 for Egger’s test), operation time (p = .50 for Begg’s test; p = .09 for Egger’s test), transfusion rate (p = 1.00 for Begg’s test; p = .45 for Egger’s test), and DVT (p = .46 for Begg’s test, p = .28 for Egger’s test).
Discussion
Herein, we conducted a comprehensive search of RCTs evaluating the effects of the tourniquet and no-tourniquet techniques in TKA for patients with osteoarthritis. Subsequently, 15 trials involving 1202 participants were included in the meta-analysis, and the pooled results showed that tourniquet use during TKA is associated with reduced intraoperative blood loss in patients with osteoarthritis. Nonetheless, tourniquet use does not have effect on postoperative blood loss, calculated blood loss, total blood loss, operation time, transfusion rate, and DVT rate. Furthermore, it remains unclear the difference between the tourniquet and non-tourniquet groups in terms of pain, RoM and swelling ratio.
Tourniquets are primarily used to reduce intraoperative blood loss and achieve better visualization during TKA. Reportedly, 58% of the members of the American College of Hip and Knee Surgeons (AAHKS) use tourniquets during TKA. 24 Although tourniquet is widely used, tourniquet-related complications have also been reported, including soft tissue and muscle injury, limb swelling, calcified vascular injury, paralysis, and nerve injury. 13 Notably, a study reported that tourniquet use can control intraoperative blood loss but cannot prevent postoperative blood loss or reduce total blood loss. 6 Meanwhile, this study also showed that tourniquets use reduce intraoperative blood loss and operation time but are not good for postoperative blood loss, calculated blood loss, total blood loss, and blood transfusion rate. The lost blood may escape into the soft tissues and cause swelling of the limbs, leading to thigh pain. The additional swelling may hinder the patient’s early functional recovery after surgery and increase soft tissue tension. Furthermore, after the tourniquet is loosened, when hemoperfusion is reestablished, ischemia-reperfusion (I-R) injury occurs, and due to venous blood stasis of the lower extremities and possible vascular damage, the risk of DVT is increased. In the present study, no significant differences were found in the DVT rate between the tourniquet and the no-tourniquet groups. Interestingly, two previous meta-analyses observed no differences in DVT incidence when tourniquets were used during TKA. 13
In 2011, a meta-analysis by Tai et al. 25 showed that tourniquets use during TKA shorten operation time but does not reduce blood loss. These results suggested that tourniquets should be used with caution during TKA due to the high risk of thromboembolic complications. In 2012, another meta-analysis by Alcelik et al. concluded that tourniquet use is beneficial; however, the results of long-term studies are needed. In 2014, a meta-analysis by Zhang et al. 26 showed that tourniquet use was superior to non-use of tourniquet during TKA with respect to thromboembolic events and other related complications. In 2019, a meta-analysis by Cai et al. 13 concluded that additional studies are essential to determine whether TKA has fewer complications without tourniquets. In this study, no significant differences were found in postoperative blood loss, calculated blood loss, total blood loss, transfusion rate, and DVT rate between the two groups.
Notably, to date, only the meta-analysis by Cai et al. 13 specifically assessed the role of tourniquet use in patients receiving TKA for osteoarthritis. Compared with the previous meta-analysis, the current meta-analysis has two main advantages. First, the inclusion of more eligible studies in this meta-analysis greatly increased statistical power (15 vs. 11), thus yielding more reliable and robust results in the current meta-analysis. Second, the current meta-analysis used trail sequential analysis to confirm whether definitive conclusions can be drawn based on currently available evidence. It is worth noting that although our meta-analysis found an effect of tourniquet use on intraoperative blood loss, which was consistent with previous meta-analysis, the current meta-analysis drawn a definitive conclusion that the effect of the use of tourniquets on intraoperative blood loss does not require additional studies. What’s more, the current meta-analysis confirmed that tourniquet use had no effect on operation time, suggesting that previous meta-analysis yielded false result. In addition, our meta-analysis also yielded definitive conclusions on other outcomes, including postoperative blood loss, calculated blood loss, total blood loss, transfusion rate and DVT rate, which could not be definitively drawn in previous meta-analysis.
This meta-analysis has some limitations. First, significant statistical heterogeneity was detected in the overall analysis; however, sensitivity analyses confirmed the robustness of the results by sequentially excluding studies because removing any one study did not significantly change the overall results. Second, neither the effect of different tourniquet applications on bone cement penetration and implant anchorage, nor the effect of prosthesis type, technique, surgical approach, or skin incision length, could be evaluated using the available data. These limitations could be attributed to the lack of data in the literature. Third, some studies had small sample sizes, which may reduce statistical power. Fourth, studies have shown differences in drainage methods, anticoagulation therapy, and timing of lower extremity tourniquets, which may lead to bias. Fifth, we need to admit that complications will certainly be affected by tourniquet pressure, but the tourniquet pressure varied from one to another among all eligible trials. So, we need to interpret our findings about this outcome with caution. Finally, the current findings are based on unadjusted assessment of RR, which may have influenced the results.
Conclusions
Based on the currently available evidence, we conclude that tourniquet use in patients receiving TKA for osteoarthritis can effectively reduce intraoperative blood loss but has no effect on postoperative blood loss, calculated blood loss, total blood loss, operation time, transfusion rate, and DVT rate. In addition, it remains unclear the difference between the tourniquet and non-tourniquet groups in terms of pain, RoM and swelling ratio.
Supplemental Material
Supplemental Material - Tourniquet use benefits to reduce intraoperative blood loss in patients receiving total knee arthroplasty for osteoarthritis: An updated meta-analysis with trial sequential analysis
Supplemental Material for Tourniquet use benefits to reduce intraoperative blood loss in patients receiving total knee arthroplasty for osteoarthritis: An updated meta-analysis with trial sequential analysis by Xiangjun Xu, Chao Wang, Qunshan Song, Zhifang Mou and Yuefu Dong in Journal of Orthopaedic Surgery.
Footnotes
Authors’ contributions
Conceptualization: Yuefu Dong, Data curation: Xiangjun Xu, Formal analysis: Chao Wang, Funding acquisition: Yuefu Dong, Investigation: Zhifang Mou, Methodology: Xiangjun Xu, Project administration: Yuefu Dong, Resources: Qunshan Song, Software: Qunshan Song, Supervision: Yuefu Dong, Validation: Chao Wang, Visualization: Chao Wang, Writing-original draft: Xiangjun Xu, Writing-review & editing: Yuefu Dong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Project of Lianyungang (Grant Number SF2205), Lianyungang Health Science and Technology Project (Grant Number 202101), Clinical Research Fund Project of the First People’s Hospital of Lianyungang (Grant Number LC14) and Scientific Research and Development Fund of Kangda College of Nanjing Medical University (Grant Number KD2021KYJJZD017).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.