
Abstract
Purpose
To perform a quantitative analysis of the amount of cancellous bone in the distal radius and olecranon process by segmentation of computed tomographic scans. As a secondary analysis, the bone density by Hounsfield units was evaluated at the same sites.
Methods
Computed tomography angiography images of the upper extremity were analyzed using 3-D Slicer™ medical imaging software. Bone volume (cm3) and density (Hounsfield units) from the cancellous bone between the distal radius and the olecranon process were compared by creating an advanced three-dimensional model. The images were analyzed in duplicate, and an intraclass correlation was performed to assess measurement consistency.
Results
Twenty subjects were included. A total volume of 5.01 ± 1.21 cm3 and 5.81 ± 1.61 cm3 for the distal radius and the olecranon process (p < .0001), respectively, was found. Regarding Hounsfield units, the density of the olecranon process was 303.1 ± 73.26, and the distal radius was 206.5 ± 63.73 (p < .0001). All intraclass correlation coefficients were >0.992.
Conclusion
These results suggest that the olecranon process has a greater volume and a higher bone mineral density than the distal radius. With these results, the surgeon will have the ability to decide the quantity and quality of bone grafts according to the surgical procedure.
Keywords
Introduction
Bone is the second most common tissue transplanted in the United States. 1 Autologous bone grafts continue to be the gold standard for non-unions, delayed union and bone loss, due to the unique biological properties of autografts (osteogenesis, osteoinduction, and osteoconduction).2,3 Multiple donor sites exist for autologous bone grafting; the anterior iliac crest (AIC) remains the graft choice for most orthopedic surgeons, although it has the highest complication rate among autologous bone grafts. 4
In certain upper extremity surgical procedures when a smaller amount of bone grafting was needed, the most common donor sites used has been distal radius (DR) or the olecranon process (OP). 5 The DR bone graft was first described by McGrath and Watson in 1981, including 78 cases with minimal complications. 5 It has been described that the volume obtained from the DR varies from 2.5 to 3.2 mL.6,7 The OP bone autograft has also been used with minimal complications. 5 In clinical and cadaveric studies, the approximate amount of bone that can be harvested varies from 2.8 to 5.7 cm3.7–9 A direct comparison between the volume of cancellous bone from DR and OP has been described in cadavers concluding that the OP has more volume than the DR. 7
Dual X-ray absorptiometry (DEXA) has been the gold standard for bone mineral density (BMD) quantification and correlates with the risk of fractures and treatment efficacy. 10 However, BMD can also be assessed through Hounsfield units (HU) with the aid of contemporary imaging softwares. 11 HU is a linear attenuation coefficient tissue measurement that provides bone quantity and quality information without additional costs or radiation. 11 Bone´s HU threshold value spans from 300 to 3,000. 11
The comparison of BMD between the distal radius and olecranon process sites has not been analyzed. The main objective of this study was to perform a quantitative analysis of the amount of cancellous bone that could be obtained in the DR and OP evaluated by segmentation of computed tomography angiography (CTA) images. Additionally, a comparison between these two areas was made as a secondary analysis. The working hypothesis was that the amount and bone density of the OP was greater than the DR.
Material and methods
The study included CTA images collected from the institutional database and was approved by the Research Ethics Committee of the same institution.
Image acquisition and volume rendering
The OP and DR images were acquired from CTAs of the upper extremity from the institutional radiological archive. Each CTA image (OP and DR) was from the same patient and extremity. Inclusion criteria were patients above 18 years and a complete CTA study (that included the complete upper extremity). Exclusion criteria were evidence of previous surgery, fracture, implants, congenital deformities, bone tumors, generalized bone disease (Paget´s disease, osteoporosis, osteogenesis imperfecta) or signs of infection at the region of interest (DR and OP).
All studies were performed on a LightSpeed ™ VCT CT 99 System (General Electric ®), with 1.25-mm to 2.5-mm slices. The images were uploaded and segmented through 3D Slicer ™ (version 5.2.1) software. This software enables multiplanar manipulation, reformation of images, and definition of a three-dimensional model of the region of interest. Then the software provides a result of the possible quantity (cm3) of cancellous bone graft that could be harvested 12 and a calculation of the BMD in HU from the region of interest. The HU data were interpreted as an indicator for BMD as previously demonstrated that HU correlates with DEXA scores .11,13 All studies were verified by a senior radiologist to meet inclusion criteria. Two orthopedic surgeons performed all image reconstruction measurements.
Distal radius quantification
The reconstruction and quantification of the DR were made exclusively on the metaphysis. The Muller square rule was used for long bones to delimit the metaphysis of the DR, ensuring a limit between the metaphysis and diaphysis
14
(Figure 1). Volume rendering and quantification of the distal radius. Multiplanar segmentation of the region of interest. (a) Coronal view. (b) Sagittal view. (c) Axial view of the distal radius.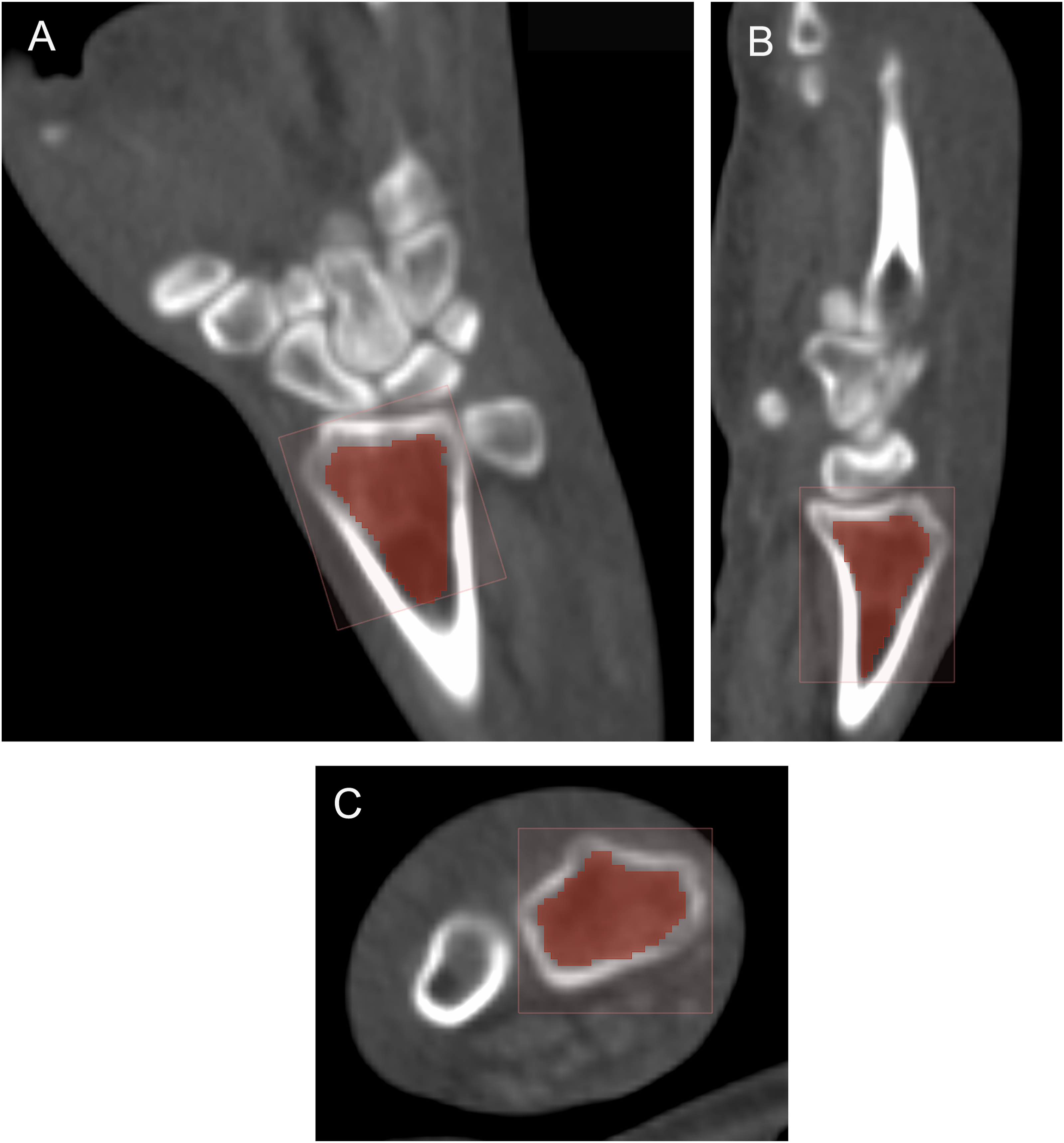
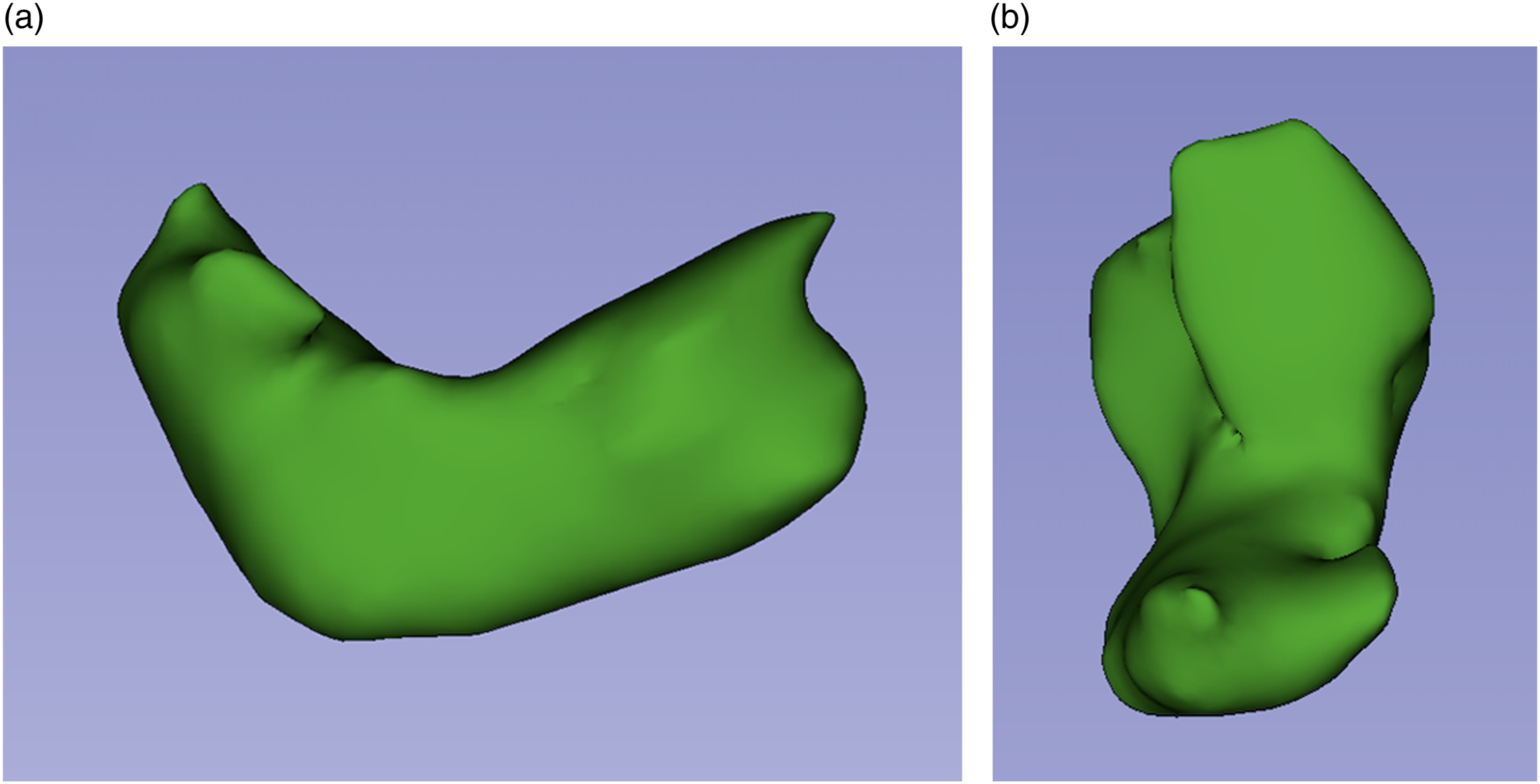
Then, using the software tools, a final three-dimensional model of the DR was obtained (Figure 2). Final three-dimensional scale of the distal radius. Three-dimensional distal radius. (a) Front three-dimensional view. (b) Lateral three-dimensional.
Olecranon process quantification
The reconstruction and quantification of the OP were addressed as follows. The cortical and corticocancellous interphase was excluded. Then the distal limit for volume rendering quantification was at the indentation of the radial head with the proximal cubitus (Figure 3). A final three-dimensional model of the OP was obtained, using the software tools (Figure 4). Volume rendering and quantification of the olecranon process. Multiplanar segmentation of the region of interest. (a) Sagittal view. (b) Axial view. (c) Coronal view of the olecranon process. Final three-dimensional reconstruction of the olecranon process. Three-dimensional olecranon process. (a) Lateral three-dimensional view. (b) Front three-dimensional view.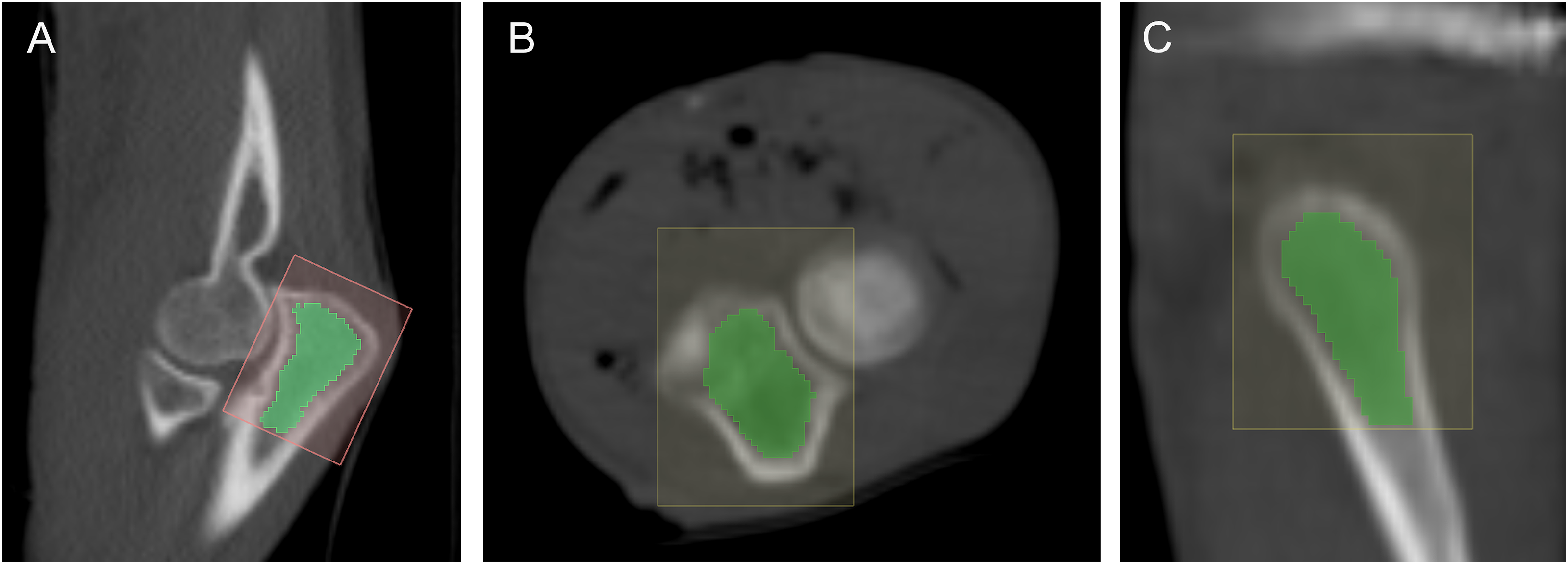
Statistical analysis
Means and standard deviations were used otherwise indicated. The data distribution was assessed with the D’Agostino & Pearson omnibus normality test. Then, the paired t test was performed to compare parametric variables. The variables age and graft volume (DR and OP) were analyzed using the Pearson correlation coefficient (r). A p-value <.05 was considered statistically significant. Data was processed with GraphPad Prism™ software version 5.00 for Windows (GraphPad Software, Inc.). To assess measurement consistency an intra-class correlation coefficient was performed, and a threshold value above 0.90 was considered excellent agreement. 15
Results
Demographic data of the included studies.

Results of volume and Hounsfield units of the olecranon and distal radius.
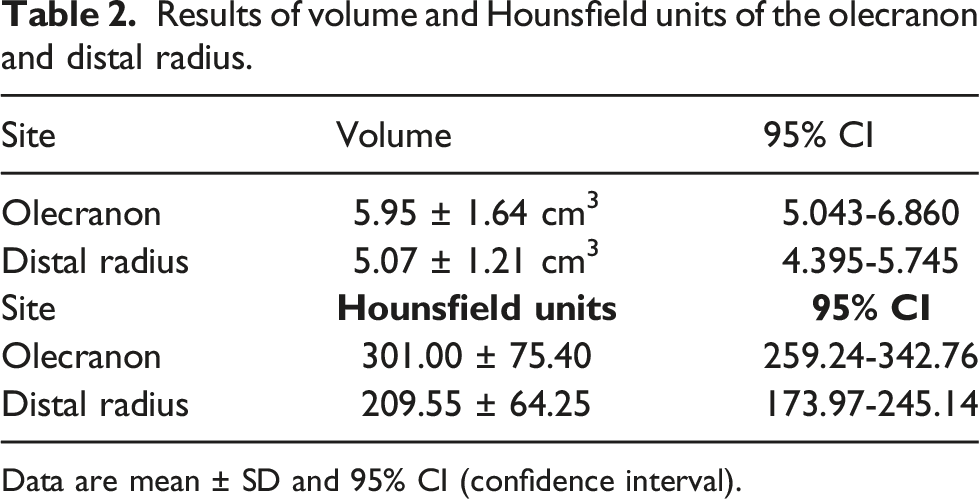
Data are mean ± SD and 95% CI (confidence interval).
The variables age and the estimated graft volume for DR and OP showed weak (r [18] = 0.29, p = .299) and moderate (r [18] = 0.57, p = .028) positive correlations, respectively. Notably, this correlation was significant solely for the OP.
The intra-class correlation coefficient values were 0.998 and 0.996 for volume (cm3) and 0.992 and 0.998 for HU measurements. This finding corresponds to excellent interobserver reliability for both measurements.
Discussion
The main finding of the study was that the OP has more volume of cancellous bone and a higher bone density than the DR. These characteristics support the OP as a good alternative for bone graft harvesting in the upper extremity.
The surgical approaches to obtain bone grafts were described by McGrath. For the DR, a dorsal transverse incision 4 cm proximal to the wrist crease is performed. Then, the fascia between the first and second compartment is incised and finally, an elliptical window to the DR is performed for curettage. 5 The bone graft of the olecranon is harvested through 3 cm on either side of the ulnar ridge, distal to the tip olecranon and bursa. Fascia is opened and an elliptical window is performed for curettage. 5 An important aspect of choosing the site for bone grafting was the quantity of bone in the area. In cadaveric studies, a total of 2.8 cm3 of bone graft was obtained from the DR and 2.7 cm3 to up to 3.9 cm3 for the OP.7,9 In clinical studies, 5.7 cm3 was obtained from the OP 8 and 3.0 mL from the DR. 6 Our CTA study consisted exclusively in an evaluation of images, without surgical approach, a mean of 5.81 cm3 and 5.01 cm3 was calculated from the OP and DR, respectively. The precision of each segmentation for the calculated region of interest could be the cause of the higher amount of cancellous bone reported in the study.
Another important issue was how much of the calculated bone graft could be harvested without causing a stress fracture. Horne et al. described that a maximum of 25% of the DR metaphysis could be harvested without causing a stress fracture. 16 According to the result of the reconstruction of the region of interest, 25% of the DR metaphysis would correspond to approximately 1.25 cm3. On the other hand, Anderson et al. reported harvesting a maximum of 2.1 cm3 to 2.2 cm3 before causing a load at failure in the OP. 17 It may seem that a greater amount of bone could be harvested on the OP without causing a stress fracture. This finding might be explained due to the differences in bone density between the OP and DR. According to the results in this manuscript, values of 303.1 HU and 206.5 HU were found in the OP and the DR zones, respectively.
A recent systematic review studied alternative imaging studies to evaluate BMD besides DEXA, and found that BMD can be measured through a CT scan by HU, these methods offer time and cost savings. 18 Currently, it remains unclear and undetermined how much BMD in HU translates clinically to a better bone autograft. In a clinical context, the BMD measured by HU has been studied in non-unions in ankle fracture and fusion rates in spinal surgery, the cut-off value of HU was 200, and they observed that patients with <200 HU had an increased rate of non-union in ankle fractures and a less fusion rate in lumbar surgery.19,20 In the upper extremity, one study found cut-off values of 121.3 HU, 103.4 HU, and 92.1 HU related with normal, osteopenic, and osteoporotic patients respectively. These results showed that patients with a lower value of HU are more likely they need a larger humeral stem. 21
The study had several limitations. The number of imaging studies available for complete analysis was small, with a broad age range and predominantly male gender of the analyzed specimens; however, significant statistical results were obtained when comparing the different anatomical zones evaluated for bone autograft harvesting. No previous DEXA studies have been performed on each patient to define a correlation between T scores and HU. There was also a lack of data normalization according to the size of the studied specimens. Finally, due to the precision of the region of interest calculated, some cancellous and corticocancellous areas not available for grafting were sometimes included, affecting the final volume and HU calculation. This bias was limited by uniformly performing the same protocol measurements and an intraclass correlation coefficient to assess measurement consistency.
These results suggest that the OP has a greater volume and a higher BMD than the DR. With these results, the surgeon will have the ability to decide the quantity and quality of bone graft according to the surgical procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.