
Abstract
Background
Arthroscopic resection of tenosynovial giant cell tumor (TS-GCT) presents favorable outcomes. However, there are reportedly higher recurrence rates in patients who had incomplete resection. To minimize incomplete resection, we established a multiple portal approach depending on the location of the disease. In this study, we aimed to retrospectively evaluate the clinical outcomes of arthroscopic resection for both localized and diffuse types of TS-GCT of the knee.
Methods
From 2009 to 2019, 13 patients who underwent arthroscopic synovectomy of the knee and were histologically diagnosed with TS-GCT were included in this study. The pre- and postoperative range of motion (ROM) of the knee was measured. The Japanese Orthopaedic Association (JOA) score and the Knee Injury and Osteoarthritis Outcome Score (KOOS) were assessed at the final follow-up examination. Magnetic resonance imaging was performed to detect incomplete resection or local recurrence.
Results
Among the 13 patients, seven and six had localized and diffuse type TS-GCT, respectively. Regarding the knee ROM, preoperative knee flexion in patients with the localized type was limited compared with that in those with the diffuse type. However, the ROM was significantly improved in patients with both types postoperatively. The JOA score and KOOS of patients with both types at the final follow-up were favorable, and there were no significant differences between both types. There was neither recurrence nor incomplete resection in any patient for both types.
Conclusion
All patients, regardless of the TS-GCT type, achieved favorable outcomes after arthroscopic surgery; especially, the failure rate was 0%.
Keywords
Introduction
A tenosynovial giant cell tumor (TS-GCT) of the knee is a rare, locally aggressive, benign tumor originating from the synovial joint, synovial bursa, and tendon sheaths. Clinical features of TS-GCT include swelling, effusion, pain, and locking sensation; these cause erosion of the articular cartilage, which could eventually progress to osteoarthritis. 1 TS-GCT is classified into two types: localized and diffuse. Both types have similar pathohistological findings; osteoclast-like multinucleated giant cells, mononuclear histiocytes, smaller round to spindle-shaped stromal cells, and hemosiderin-laden macrophages. 2 Grossly, the localized type appears to be a solitary, pedunculated lesion covered with synovium, whereas the diffuse type involves the joint or extra-articular parts of the knee with villonodular synovitis. 3
The standard therapy for TS-GCT is complete surgical resection. There are some reports of chemotherapy or radiotherapy as treatment options; however, a consensus has not yet been reached owing to a lack of evidence.4,5 Surgical treatments, including arthroscopic resection, open resection, and a combination of both, have been reported to have favorable outcomes. 6 However, arthroscopic resection may provide better visualization and is a less invasive treatment. 7 Conventional arthroscopic resection requires both anteromedial and anterolateral portals and small skin incisions. This procedure is less invasive; however, inadequate resection or tumor remaining may be noted, especially in the posterior part of the knee. Subsequently, local recurrence has been shown to develop with conventional arthroscopic resection. 5 There are higher recurrence rates in the diffuse type post-surgery (up to 50%) and in patients who had incomplete resection. 5 To minimize incomplete resection and promote adequate total synovectomy, we established a multiple portal approach in addition to the standard anteromedial and anterolateral portals, depending on the disease’s location.
Recently, modified arthroscopic resections using multiple portals for the TS-GCT have been reported, aiming to perform complete or extended resection. 8 In those reports, favorable oncological outcomes had been achieved. However, functional outcomes of the knee remain unclear.
Therefore, this study aimed to evaluate the oncological outcomes of modified arthroscopic resection of the TS-GCT of the knee using multiple portals and to assess the functional outcomes both preoperatively and postoperatively.
In this study, the rates of incomplete resection and local recurrence, deemed as failure of local oncological treatment, were the primary endpoints. Pre- and postoperative range of motion (ROM) of the knee and postoperative subjective clinical outcome scores were the secondary endpoints.
Materials and methods
Patient selection
We retrospectively identified 19 patients who underwent arthroscopic resection from January 2009 to December 2019 at our institution and had a histologic diagnosis of TS-GCT. This study included patients with localized and diffuse intra-articular TS-GCT who had completed postoperative assessments at the final follow-up examination. Patients with follow-up periods <3 months, an incomplete postoperative evaluation, and extra-articular invasion were excluded. Of the 19 patients, 13 met the inclusion criteria. Six patients were excluded: four were lost to follow-up and two had posterior extra-articular invasion. The indications for surgery were as follows: symptoms of knee arthritis, limitations of knee ROM, and disease progression.
As part of the objective clinical outcomes, the ROM of the knee was compared before surgery and at the final follow-up examination. Assessment of the knee using the Japanese Orthopaedic Association (JOA) score was also performed at the final follow-up examination.
9
As a subjective clinical outcome, the Knee Injury and Osteoarthritis Outcome Score (KOOS)
10
was evaluated at the final follow-up examination. Pre- and postoperative magnetic resonance imaging (MRI) examinations were performed and reviewed by the radiologist in our institute to detect recurrence. Regarding postoperative follow-up MRI, the patients visited the outpatient clinic once every 3 months for 2 years postoperatively and underwent MRI; subsequently, the patients underwent MRI once every year at the outpatient clinic. The resection status was assessed based on the MRI findings and operation records and classified as either complete or incomplete resection. Incomplete resection was defined as residual disease detected on MRI performed 3 months postoperatively. The progression of incomplete resection and the presence of local recurrence following complete resection were defined as local failure. Intraoperative and postoperative complications, such as infection, joint stiffness, and neurovascular injury, were investigated retrospectively. The study flowchart is presented in Figure 1. The study flowchart.
This observational research study was approved by the Institutional Review Board of our hospital. Written informed consent was obtained from all the patients before surgery.
Surgical technique
We performed arthroscopic resection for the patients with intra-articular TS-GCT. To achieve complete arthroscopic resection of intra-articular forms of the disease, we used several portals, namely, the superomedial, superolateral, accessory posteromedial, and posterolateral portals, in addition to the standard anteromedial and anterolateral portals, depending on the location of the disease.
8
For diffuse type TS-GCT, we used the aforementioned portals and performed adequate total synovectomy through anterior, posterior, and trans-septal posterior approaches (Figure 2(a)–(c)). No adjuvant treatments, such as irradiation and administration of colony-stimulating factor-1 receptor inhibitors, were performed postoperatively. Representative intraoperative photographs. (a) Arthroscopic synovectomy via posterolateral and posteromedial portals. (b) The posterior septum is perforated through a radiofrequency ablation via the posterolateral portal. (c) A trans-septal approach allows safe resection of the tumor in the posterior compartment of the knee.
Statistical analysis
A paired t-test was used for the comparison of pre- and postoperative ROM of the knee. In addition, the ROM, postoperative JOA score, and postoperative KOOS were compared between the localized type and diffuse type using Student’s t-test. Fisher’s exact test was used to compare the number of incomplete resections and local recurrence between the localized type and diffuse type. Statistical significance was set at p < .05.
Results
Oncological outcomes
Patient characteristics.

*Fisher’s exact test, †Student’s t-test.
Functional outcomes
Pre- and postoperative ROM of the knee
In localized type TS-GCT, the mean postoperative knee extension angles were improved to 0° (standard deviation [SD], ±0; range, 0) compared to those before surgery (−1.4°; SD, ±2.4; range, −5–0) (Figure 3). Moreover, the mean postoperative knee flexion angles were significantly improved from 116.4° (SD, ±19.7°; range, 90–140°) to 137.9° (SD, ±8.1°; range, 120–145°) (p < .01). In diffuse type TS-GCT, the mean pre- and postoperative knee extension angles were both 0° (SD, ±0°; range, 0°), while the mean pre- and postoperative knee flexion angles were both 139.2° (SD, ±4.9°; range, 120°–145°). Patients with the localized type had significantly worse preoperative knee flexion angles than those with the diffuse type (p = .02); however, there were no significant differences in the postoperative knee flexion angles between the localized and diffuse types. Range of motion (ROM) of the knee. The preoperative knee flexion in the localized type is significantly worse than that in the diffuse types of TS-GCT (p < .05). The postoperative knee flexion in the localized type is significantly better than that before surgery. (p < .01). TS-GCT: tenosynovial giant cell tumor.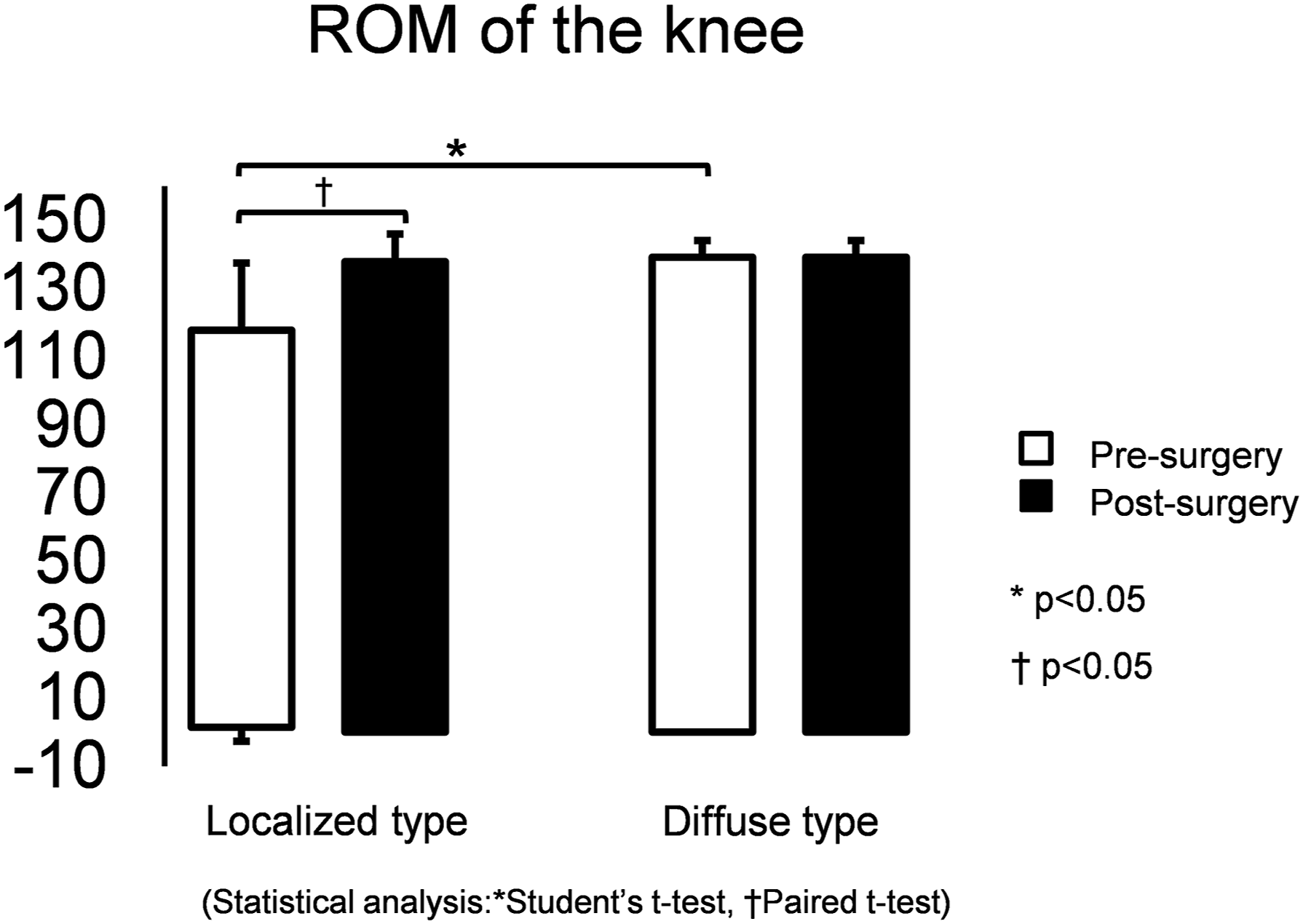
Postoperative JOA score
The JOA scores at the final follow-up examination were 100 (SD, ±0; range, 100) and 94.2 (SD, ±6.6; range, 85–100) points in patients with localized and diffuse TS-GCT, respectively (Figure 4). Patients with localized TS-GCT had significantly higher JOA scores than those with diffuse TS-GCT (p < .05). JOA scores. The JOA scores at the final follow-up demonstrate significant differences between the patients with localized and diffuse type TS-GCT (p < .05). Despite this significant difference, all scores were otherwise favorable. JOA: Japanese Orthopaedic Association; TS-GCT: tenosynovial giant cell tumor.
Postoperative KOOS
The average overall KOOS at the final follow-up examination for patients with localized TS-GCT were 92.5% (SD, ±12.4; range, 69.4–100) in pain; 92.3% (SD, ±12.1; range, 71.4–100) in symptoms; 94.7% (SD, ±12.1; range, 67.7–100) in activity of daily living (ADL); 85.7% (SD, ±20.0; range, 55–100) in function in sports and recreation (Sport/Rec); and 83.9% (SD, ±26.0; range, 37.5–100) in knee-related quality of life (QOL) (Figure 5). Patients with diffuse TS-GCT had averages of 91.2% (SD, ±7.3; range, 83.3–100) in pain; 87.8% (SD, ±7.0; range, 78.6–96.4) in symptoms; 96.3% (SD, ±3.8; range, 91.2–100) in ADL; 82.5% (SD, ±18.6; range, 55–100) in Sport/Rec; and 82.3% (SD, ±18.3; range, 56.3–100) in QOL (Figure 5). There were no significant differences between the two types of TS-GCT. KOOS. The KOOS at the final follow-up in patients with both types of TS-GCT show favorable values; there are no significant differences between the localized and diffuse types. KOOS: Knee Injury and Osteoarthritis Outcome Scores; TS-GCT: tenosynovial giant cell tumor.
Discussion
We retrospectively analyzed the clinical outcomes of arthroscopic resection using multiple portals in patients with localized and diffuse type TS-GCT at our institution. This treatment modality yielded favorable outcomes, as shown by oncological outcomes, improved knee ROM, and functional outcomes.
First, concerning the oncological outcomes, we defined “failure” as the presence of a recurrence or the progression of incomplete resection, as stated in previous literature.5,11 Regarding the failure rate after conventional arthroscopic resection of each type of TS-GCT, the diffuse type is likely to have a higher recurrence rate than the localized type. Palmerini et al. described that the 5-year local failure-free survival rate was higher for the localized type (84%) than for the diffuse type (59%). 5 Furthermore, according to Kim et al., arthroscopic resection is more likely to be incomplete in an extra-articular invasion case of diffuse type TS-GCT. 12 Contrary to several studies, Chang et al. reported that a modified arthroscopic resection that uses additional posteromedial and posterolateral portals could achieve adequate resection with minimal risk of complications. 8 In our study, the patients who underwent modified arthroscopic resection did not experience recurrence and incomplete resection for both localized and diffuse type TS-GCTs. Similar to the results reported by Chang et al., we used the superomedial and superolateral portals or a trans-septal approach via the posteromedial and posterolateral portals to improve visualization in the suprapatellar bursa and posterior compartments of the knee. Regarding intraoperative and postoperative complications, caution is advised when creating posteromedial and posterolateral portals to prevent saphenous neurovascular injury and common peroneal nerve injury, respectively. Moreover, there are risks involving the popliteal neurovascular structures when using the trans-septal approach. 8 In our study, we achieved careful arthroscopic resection to ensure safety of the neurovascular bundle, specifically when we approached the posterior compartment of the knee. Throughout the follow-up period, there were no incidences of intraoperative and postoperative complications.
Regarding the ROM, postoperative knee stiffness was considered to be a problem associated with a parapatellar incision of open synovectomy in diffuse type TS-GCT. 13 In contrast, arthroscopic synovectomy was reported to reduce the incidence of loss of ROM of the knee in both localized and diffuse types. 11 In our study, preoperative knee flexion angles in patients with the localized type were significantly lower than in patients with the diffuse type. We inferred that a localized tumor, which was located mostly below the patella or around the cruciate ligament of the patients, affected the knee flexion angle. Indeed, the knee flexion angles were significantly improved after arthroscopic resection, and there were no significant differences in postoperative knee flexion between the localized and diffuse type TS-GCT. Moreover, patients with diffuse TS-GCT did not experience worsened ROM postoperatively. These results indicate that one of the advantages of this modified arthroscopic resection is its postoperative improvement of knee ROM.
Previous reports have shown that conventional arthroscopic resections of both localized and diffuse types resulted in better functional outcomes than those of open resection. Loriaut et al. described that a postoperative Lysholm score, a subjective scale to measure symptoms and function in patients with knee injuries, of patients who underwent conventional arthroscopic resection with localized TS-GCT was 85.5 points. 14 Gu et al. reported that the postoperative Lysholm score and the International Knee Documentation Committee score, a subjective knee evaluation scale, in patients who had conventional arthroscopic surgery for diffuse TS-GCT were 88.4 and 84.7, respectively, which were better than those of patients who had an open surgery. 7 In our study, we achieved favorable functional outcomes after performing the modified arthroscopic resection, similar to previous studies where the conventional arthroscopic resection was performed.
The limitations of our study include the small number of patients and the short follow-up period. A larger number of patients is needed to clarify the failure rate of both localized and diffuse type TS-GCT. Diffuse type TS-GCT often involves extra-articular parts of the knee; however, we did not include patients with extra-articular invasion. The reason was that we used a combined arthroscopic and open surgical approach for the patients who had extra-articular invasion to reduce the risk of incomplete resection, which possibly became the bias of our study as we focused on the arthroscopic excisions of TS-GCTs. The patient selection criteria should be defined to conduct future studies with clarity. Moreover, this study should be extended in the future, and longer follow-up periods can add more scientific clarity. Additionally, our study lacked preoperative functional outcome scores. Although we could not compare pre- and postoperative functional outcome scores, the postoperative ROM of the knee and functional outcome scores were shown to be favorable in both types of TS-GCT. Finally, in analyzing the failure in this study, recurrence was detected through MRI findings but was not histologically proven. However, MRI provides sufficient information to promptly detect recurrent cases by depicting the joint effusion, synovial proliferation, bone erosion, and deposits of hemosiderin in the tumor. 15
Conclusion
We evaluated the retrospective clinical outcomes of localized and diffuse types of TS-GCT after arthroscopic resection using multiple portals. Favorable surgical outcomes were achieved in both types of TS-GCT. Recurrence and incomplete resection did not occur among patients with localized and diffuse type TS-GCTs. Overall, arthroscopic resection with multiple portals described in this study may be one of the surgical options for intra-articular TS-GCT, even though the diffuse type has a high recurrence rate.
Footnotes
Acknowledgements
We would like to thank Dr. Takashi Toma and Dr. Hiroki Yabiku for useful discussion. We also would like to thank Editage (www.editage.com) for the English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.