
Abstract
Purpose
To determine whether a double anchor is more effective than a single anchor in the surgical repair of the anterior talofibular ligament (ATFL) in patients with ankle instability.
Methods
This study searched PubMed, Embase and the Cochrane Library to identify potential studies that compared the clinical outcomes of double anchors and single anchors for ATFL repair from inception to July 31st, 2023. The study aligned with the 2020 Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines and checklist. The Risk of Bias in Nonrandomized Studies-of Interventions (ROBINS-I) tool was used to evaluate methodologic quality and risk of bias. The meta-analysis was performed with random effects. Outcomes, including American Orthopaedic Foot & Ankle Society Score (AOFAS), Karlsson Ankle Functional Score (KAFS), Tegner activity score, return to sport rate, complications and revision surgery events, were recorded.
Results
A total of 845 articles were identified after an initial search of the three databases. Four retrospective studies involving 231 individuals were included for further analysis. There was no significant difference between the single-anchor group and the two-anchor group in terms of the AOFAS (risk ratio, −0.44, [−2.22; 1.34]) or KAFS (mean difference, −2.81, [−6.87; 1.25]). However, in terms of the Tegner activity score and the return to sport rate, the single-anchor group had significantly lower scores and longer times than the double-anchor group. No complications or revision surgery events were reported.
Conclusions
In patients with chronic ankle instability, both single anchors and double anchors can provide good functional outcomes. For patients who participate in physically demanding sports, double anchors may be a superior option.
Level of Evidence
Level Ⅲ, meta-analysis of Level Ⅲ
Introduction
Chronic ankle instability (CAI), which is often caused by ankle sprain, is one of the most common sports injuries encountered by foot and ankle surgeons.1,2 CAI is characterized by repeated sprains, prolonged and persistent pain and ankle subluxation. 3 Common risk factors include high BMI, midfoot cavus, hindfoot varus, and generalized laxity neuromuscular stability deficits.4,5 Although there is a paucity of literature analysing the cost of treating patients with CAI, it is financially burdensome as a common sequela of ankle sprains.6–8 Methods to treat CAI has become an important topic of discussion.
Effectively treatment for CAI relies on addressing both mechanical and functional instability. 9 Surgical treatments are often performed when nonoperative treatments are ineffective.10,11 One of the current surgical procedures is to repair the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL). However, there is no consensus on whether to use a single anchor or double anchor for the ATFL.
A single anchor is a cheaper option, but double anchors theoretically provide more contact area. The clinical efficacy of the two different options deserves further exploration.
The aim of this study was to explore whether double anchors are more effective than single anchors in the surgical repair of the ATFL via a meta-analysis of cohort studies. The hypothesis was that double anchors are not superior to single anchors in ATFL repair in terms of AOFAS, KAFS, Tegner activity score, return to sport rate and complication rate.
Method and materials
Study protocol
The study was registered on PROSPERO (CRD42022328173) and aligned with the 2020 Preferred Reporting Items for Systematic Reviews (PRISMA) guidelines. 12
Search strategy
Two independent researchers explored three databases, PubMed, Embase and the Cochrane Library, from inception to July 31, 2023. The authors searched the databases with the following terms: ((talofibular ligament) OR (ankle)) AND ((anchor) OR (suture anchor)). Only English studies were included during this process.
Inclusion criteria
Studies were included when they met the following criteria: • • •
Exclusion criteria
The exclusion criteria were as follows • Cadaver experiment study or cell experiment • Technical note • Cross-sectional or case‒control study
Data extraction process
Two independent researchers gathered data from eligible studies. Basic characteristics were collected as follows: author, year, age, country, sex, body mass index (BMI), concomitant injuries, operation method, fixation technique, postoperative management, outcome, and level of evidence (LOE). Additionally, AOFAS, KAFS, Tegner activity score, return to sport rate (a level equal to or higher than preinjury activity), complications (including wound infection, numbness, nerve injury, and vascular injury) and revision surgery events were extracted for further analysis. When there was a disagreement between the two researchers, a third researcher made the final decision.
Data synthesis and statistical analysis
This study focuses on the meta-analysis conducted through R software (version 4.3.1) with a meta package. Heterogeneity of the meta-analysis results was assessed with I2 and tau, 2 and a random-effects model was performed for all analyses. Continuous outcomes were evaluated by mean differences (MDs) with 95% confidence intervals (95% CIs), and dichotomous outcomes were calculated via risk ratios (RRs) with 95% CIs. The diamond represents the final synthetic effect of data from included studies being presented in a forest plot. All outcome comparison analyses were two-tailed, with a significance of 0.05.
Risk of bias evaluation and quality assessment
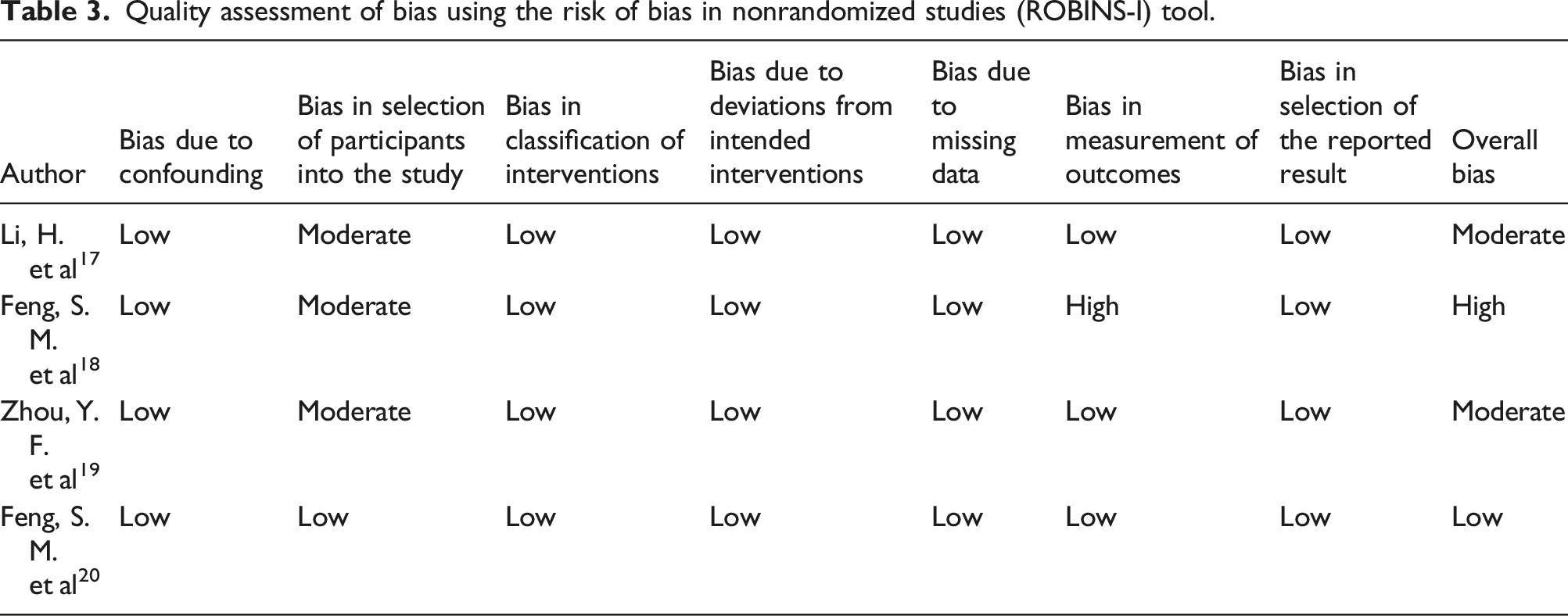
For cohort studies, the ROBINS-I tool, which included 7 evaluation domains (bias due to confounding, bias in the selection of participants chosen for the study, bias in the classification of interventions, bias due to deviations from the intended interventions, bias due to missing data, bias in the measurement of outcomes and bias in the selection of the result reported), was used to assess the risk of bias. 16
Results
Literature search and selection process
A total of 845 studies (PubMed = 523, Embase = 265, Cochrane = 57) were included after an extensive search of the three databases. A further search identified 215 duplicates, and the remaining 630 studies were screened. After excluding studies on unrelated topics, a total of five studies remained to be searched further. Eventually, 4 studies17–20 met the inclusion criteria (Figure 1). 2020 Preferred Reporting Items for Systematic Reviews (PRISMA) flow chart.
Study characteristics
Characteristics and details of the included studies.

Abbreviations: BMI: body mass index; F: female; DA: double anchor; M: male; NA: not available; OCD: osteochondral defect; SA: single anchor; STS: sinus tarsi syndrome.
*This study excluded patients with osteochondral lesions of the talus.
Operation details.

Abbreviations: ADT: Anterior drawer test; AOFAS: American Orthopaedic Foot & Ankle Society Score; FAOS: Foot and Ankle Outcome Score; KAFS: Karlsson Ankle Functional Score.
Risk of bias evaluation and quality assessment
Three studies17–19 were considered to have a moderate risk of bias in terms of the selection of participants for the study due to the inclusion of patients with concomitant injuries. One study 18 was considered to have a high-risk of bias in terms of the measurement of outcomes due to differences in patient immobilization time during rehabilitation, which may have an effect on postoperative outcome assessment. (Table 3).
Meta-analysis
AOFAS
Four studies17–20 involving 231 individuals reported AOFASs, and the results were not significantly different between the single-anchor group and the double-anchor group (RR, −0.44, [-2.22; 1.34]). The heterogeneity was high (I2 = 7%; τ2 = 0.988, p = .36). (Figure 2) Forest plot showing the difference in the American Orthopaedic Foot & Ankle Society Scores between the single-anchor and double-anchor groups. CI, confidence intervals; MD, mean difference; SD, standard deviation.
KAFS
Four studies17–20 involving 231 individuals reported KAFSs, and the results were not significantly different between the single-anchor group and the double-anchor group (MD, −2.81, [-6.87; 1.25]). The heterogeneity was high (I2 = 76%; τ2 = 11.878, p < .01). (Figure 3). Forest plot showing the difference in Karlsson Ankle Functional Score between the single-anchor and double-anchor groups. CI, confidence intervals; MD, mean difference; SD, standard deviation.
Tegner activity score
Two studies17,19 involving 97 individuals reported Tegner activity scores, and the results showed that the single-anchor group had a lower Tegner activity score than the double-anchor group (MD, −0.87, [-1.30; −0.45]). There was no heterogeneity (I2 = 0%; τ2 = 0, p = .49). (Figure 4). Forest plot showing the difference in the Tegner activity scores between the single-anchor and double-anchor groups. CI, confidence intervals; RR, risk ratio.
Return to sport rate
Four studies17–20 involving 231 individuals reported the return to sport rate, and the results showed that the single-anchor group had a lower proportion of patients who were able to return to sports than the double-anchor group (RR, 0.60, [0.40; 0.92]). Heterogeneity was not high (I2 = 66%; τ2 = 0.107, p = .03). (Figure 5) Forest plot showing the difference in the return to sport rate between the single-anchor and double-anchor groups. CI, confidence intervals; RR, risk ratio.
Complication
A total of 3 studies17–19 involving 172 individuals reported complications, and none of the patients experienced postoperative complications.
Revision surgery event
Discussion
The main findings of this study are that the efficacy of the single-anchor is not inferior to that of the double-anchor.
The AOFAS for pain, function and voluntary movement, stability, and foot force lines provide a more comprehensive assessment of daily function in patients after ATFL repair. At the same time, the KAFS is an assessment of pain, swelling, stiffness, and other aspects of daily activities. There was no significant difference between the single-anchor group and the double-anchor group in terms of these two outcome measures, which indicates that both surgical methods are suitable for meeting the daily life needs of the patient. There were no reported complications or secondary surgical events, demonstrating the safety of both procedures. In an insertional Achilles tendon surgery study, DeVries, J. G et al. 21 reported a noticeable difference in cost between single anchor repair (US$391.18 ± US$272.10) and double row repair (US$1811.2 9 ± US$169.47). Therefore, for most patients, satisfactory results can be achieved regardless of the type of surgery performed.
The Tegner activity score is more reflective of work and physical activity. In this study, the return to sport rate represents the number of people who return to preinjury or higher levels of sport. The results show that 2 anchors perform better in meeting the demands of higher intensity sports. Cottom JM et al. 22 also showed that when the number of proximal suture anchors was increased, there was a statistically significant increase in strength with respect to maximum failure loads. In addition, theoretically, 2 anchors can provide a larger contact area in the footprint area, which facilitates the patient's postoperative recovery. Therefore, 2 anchors are a more appropriate choice for patients who participate in high-intensity exercise.
Implications for practice
For patients
For patients who participate in low-intensity exercise, a single anchor can be sufficient for daily life and is cost-effective.
For clinicians
A single anchor improves the clinical prognosis of patients who participate in low-intensity exercise and is cost-effective.
For patients who exercise intensely, especially athletes, double anchors facilitate the return to their respective sport.
Limitations
There are three major shortcomings of this study. First, the small number of eligible studies and smaller sample sizes undoubtedly affect the reliability of the outcome effects. The second point is that the type of fixator used during surgery varied among operators and there were inconsistencies in the postoperative rehabilitation programs, all of which may have had some impact on the final results. In addition, all the included studies were retrospective, which contributes to the low level of evidence.
Conclusions
In patients with chronic ankle instability, both single anchors and double anchors can provide good functional outcomes. For patients who participate in physically demanding sports, double anchors may be a superior option.
Footnotes
Author contributions
DYF conceived the design of the study. DYF and LXH collected the data, performed the data analysis and contributed to the design of the study. DYF analysed the data. DYF and LZ prepared and revised the manuscript. The authors read and approved the final content of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The present study was a review of the previously published literature.