
Abstract
Background
Bicondylar tibial plateau fractures are complex injuries that commonly require surgical repair. Long-term clinical outcome has been associated with discrepancies in leg alignment, instability and condylar width abnormalities. While intuitive, the degree of articular damage at time of injury has not been linked to outcomes in patients with bicondylar tibial plateau fractures. The aim of this study was to quantify percentage of articular surface cross sectional area disruption and assess for correlation between the degree of articular injury and patient reported physical function.
Methods
Retrospective cohort study at two level 1 trauma centers. 57 consecutive patients undergoing surgical repair for bicondylar tibial plateau fractures between 2013 and 2016.
Main outcome measure
Preoperative CT scans were reviewed, and the percentage of articular surface disruption cross sectional area was calculated. PROMIS® scores were collected from patients at a minimum of 2 years.
Results
57 patients with an average age of 58 ± 14.3 years were included. The average PROMIS® score was 45.5. There was a correlation between percentage of articular surface disruption and total PROMIS® scores (0.4, CI: 0.2–0.5, p = .007) and the physical function of the PROMIS® score (0.4, CI: 0.2–0.6, p < .001).
Conclusion
Our method for calculating articular surface disruption on CT is a simple, reproducible and accurate method for assessing the degree of articular damage in patients with bicondylar tibial plateau fractures. We found that the percentage of cross-sectional articular surface disruption correlates with patient reported outcomes and physical function.
Keywords
Highlights
• Bicondylar plateaus are challenging injuries associated with poor outcomes. • Current classification systems for assessing plateau fractures have poor to fair reliability and reproducibility. • Using CT scans we have developed an easy and reliable method for quantifying articular surface damage of tibial plateau fractures. • We found that articular surface damage of tibial plateau fractures correlates with functional outcomes.
Introduction
Tibial plateau fractures are common injuries in adults 30–60 years old. They account for approximately 1% of all fractures and have an incidence of 10.3–13.3/100,000 annually.1,2 Similar to other intra-articular injuries, tibial plateau fractures can result in arthritis, joint instability, deformity and restricted range of motion. 3 There is a wide variety of tibial plateau injuries, ranging from simple unicondylar fractures to more challenging bicondylar fractures. Tibial plateau fractures are classified using either the Schatzker classification system, 4 or the AO/OTA system described by Müller. 5 Classifying these fractures is key for determining the epidemiology, severity, treatment, and outcomes.
Despite their value, these classification systems are not without drawbacks used in clinical practice. Interobserver reliability and intraobserver reproducibility of tibial plateau radiographic fracture classification is only fair. Little work has been done linking injury severity with outcomes and results are variable. Articular step off has been correlated with poor outcomes, and the quality of reduction achieved has been linked to the severity of articular injury. 6 The greater the displacement and comminution in these fractures, the worse the reduction after fixation might be. In addition, fractures with more comminution lead to worse satisfaction and worse clinical outcomes.7–9
Bicondylar tibial plateau fractures (AO/OTA classification type 41-C) are complex injuries that commonly require surgical repair. Bicondylar plateau fractures have been typically associated with worse reductions and outcomes. 10 Optimal long-term clinical outcome is challenging due to leg alignment abnormalities, articular surface congruity, instability and difficulties restoring condylar width. 8 While intuitive, the degree of direct articular injury has not been linked to outcomes in patients with bicondylar tibial plateau fractures.
The primary aim of the study was to quantify articular surface disruption by obtaining a percentage of cross sectional area of articular damage to assess for any correlation between the degree of articular injury and patient reported physical function via PROMIS® scores.
Materials and methods
We examined patients that had surgical repair for a bicondylar tibial plateau fracture (AO/OTA classification type 41-C) at two level 1 trauma centers from 2013 to 2016. Patients with bicondylar plateau fractures were consecutively selected within that time period and were treated only by trauma fellowship trained surgeons. 60 patients were identified and selected, however three did not have appropriate CT scans and were excluded, resulting in a total of 57 patients analyzed.
All preoperative CT scans were evaluated by a musculoskeletal radiology fellow (PGY-6), who was blinded to clinical data. Additionally, 20 cases were selected at random and independently and blindly evaluated by a musculoskeletal radiologist with 6 years of experience. The intraclass correlation coefficient was calculated and Bland-Altman analysis was performed to determine inter-reader agreement.
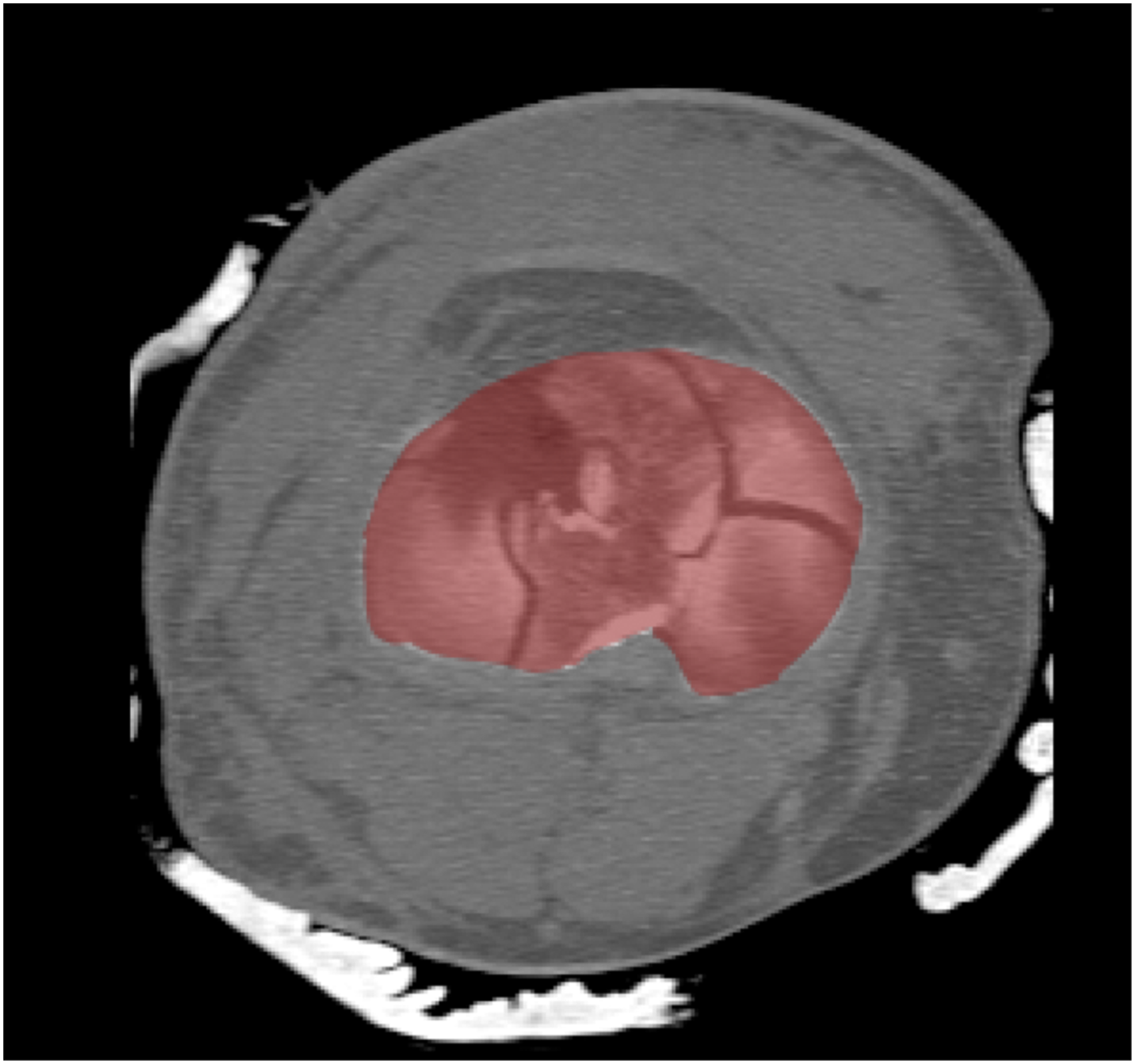
Each radiologist performed the following: Oblique median root prior (MRP) reconstructions were made perpendicular to the axis of the tibial shaft, and an en face view of the tibial plateau was selected. A maximum intensity projection was used to create a best-fit surface with a 3 mm slice thickness, the top slice aligned with the superior most tibial joint surface (Figure 1). The resultant axial-oblique images were then opened in PhotoshopTM (Adobe Systems, San Jose, CA, USA; Figure 2). The expected amount of tibial subchondral bone plate was traced, and the exact area was measured (Figure 3). Any absent, depressed or fractured parts of the joint were selected, and the articular surface disruption was calculated as the percentage of the expected intact tibial plateau (Figure 4).
11
PROMIS® scores were collected from patients in clinic at a minimum of 2 years post-operative. Pearson correlation was performed to assess associations between percentage of disrupted articular surface and PROMIS® scores. A representative oblique MPR reconstruction perpendicular to the axis of the tibial shaft. A representative resultant oblique image of the joint surface. A representative image of the articular surface of the tibial plateau traced and measured. A representative image with all absent and depressed portions of the articular surface removed.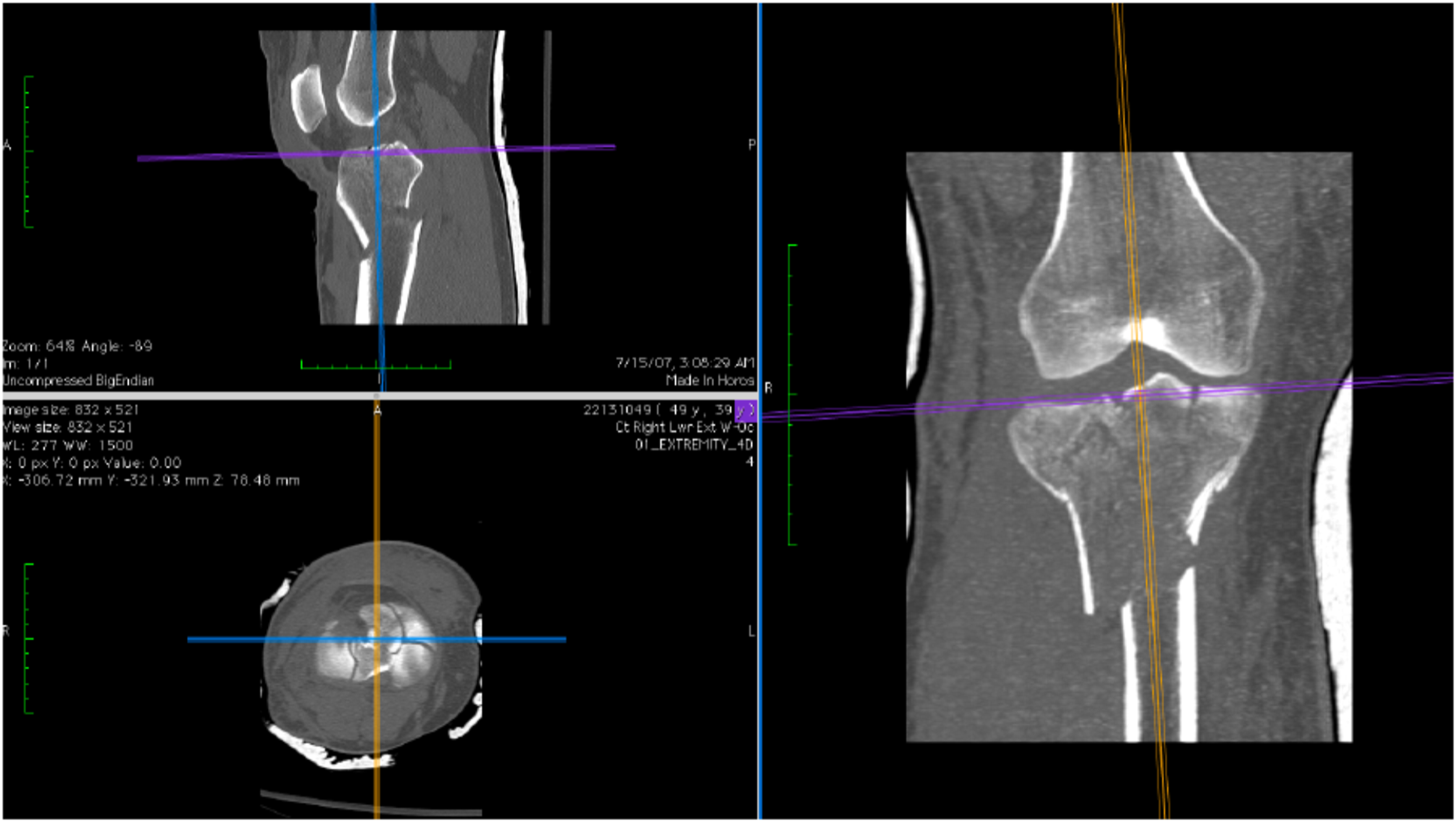


Results
Demographics.

Correlation of RPOMIS scores to articular damage. Table represents the total PROMIS scores and its physical function (pfa01, pfc36, pfc37, pfa05, pfa03, pfa11, pfa16, pfb26, pfa55, and pfc45).

Outcomes.

Discussion
Bicondylar tibial plateau fractures are complex fractures often associated with poor reductions and outcomes. 12 Outcomes have been correlated to residual deformity, persistent post operative instability, and expanded condylar width.7–9 This is the first study correlating quantity of articular surface damage with patient reported functional outcomes.
Studies of tibial plateau fractures have typically looked post-fixation. In these a small percentage of patients have persistent functional limitations that can last for three to 4 years. 13 Steven et al. found higher functional outcome scores post-fixation as measure by SF-36 and WOMAC, and there was no correlation in fracture pattern. 7 These studies were underpowered for assessing fracture pattern, which may explain this lack of correlation. In a series of Schatzker V and VI fractures treated operatively, Pun et al. measured extensor lag, range of motion, thigh atrophy and joint stability, and found that 13 patients had good outcome scores, 7 patients had fair outcome scores, and 1 patient had poor outcome scores. They also found that all but 2 patients in their series had excellent walking and stair climbing. 14 None of these studies assessed pre-operative damage and functional outcomes. We found a correlation between degree of articular surface damage and functional outcomes. Articular damage correlated with total PROMIS® scores (0.4, CI: 0.2–0.5, p = .007), and the physical function of the PROMIS® scores (0.4, CI: 0.2–0.6, p < .001). This strongly suggests that we should educate patients with bicondylar plateau fractures that have severe articular displacement that they should expect worse functional outcomes. In general, The PROMIS PF is scored on a 0-point to 100-point scale, with a population mean of 50 and SD of 10.
We measured tibial plateau articular surface damage on CT scans in a method similar to previously described for glenoid bone loss. 11 Interobserver reliability and intraobserver reproducibility of assessing intra-articular fractures has historically been quite poor.15–17 The reliability of assessments based on radiographs and CT scans of the tibia vary widely. Location of fracture lines had the greatest reliability (κ = 0.68), and stability had the poorest reliability (κ = 0.37) on radiographs. CT scans improved reliability, but not significantly. Condylar widening and maximal articular depression had an interclass correlation coefficient of 0.72 and 0.66. 18 Evaluating interobserver and intraobserver agreement for treatment plan and fracture classification of tibial plateau fractures the mean kappa classification for treatment plan increased from 0.58 to 0.71 when using CT over plain radiographs alone. There was no difference in classification. 19 This study suggests that CT has a role in treatment planning alone. The addition of MRI improved kappa values from 0.68 with plain radiographs, and 0.73 with the addition of CT to 0.85 with MRI for assessing the Schatzker classification system. 20 In the current study we had an excellent intraobserver and interobserver reliability with an interclass coefficient of 0.913. Given its high agreement this CT measurement technique may be beneficial for future applications assessing classification and treatment options.
Tibial plateau fractures, particularly bicondylar plateau fractures are associated with high complication rates. Major complication rates of high energy plateau fractures range from 27% to 31%.21,22 Weigel and Marsh reported on 31 fractures, 21% of knees had evidence of grade 2 or higher arthritis. 23 Early reports on high grade tibial plateau fractures showed infection rates as high as 80%,24,25 with newer surgical techniques infection rates are now reported between 10 and 14%. 26 In this series 21% of the patients had a major complication. Minor complications included, post-traumatic arthritis (21.1%), painful implant (14%), infection (8.8% superficial, 7% deep). Secondary joint replacement has been reported at 5.3% at 5 years and 7.3% at 10 2years. The probability for TKA significantly increased with higher age, increased co-morbidities, and bicondylar fractures. 27 Similar to previously reported, there was an 8% conversion rate to TKA.
Our limitations in this study include the fact that we do not have postoperative imaging to assess articular reduction and compare it to long-term functional outcomes and is planned as a new research study. Another limitation is that there were eight orthopaedic trauma surgeons that performed surgery for the proximal tibia fractures, however all of them where fellowship trained with similar philosophies.
Conclusion
Bicondylar tibial plateau fractures present multiple treatment challenges. The novel method of quantifying articular surface damage as a percentage of cross sectional area on CT in this study is easy and demonstrates high inter-reader reliability, and correlation with PROMIS® scores at minimum 2-years follow-up. It has potential to help determine classification, fixation strategies, and outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.