
Abstract
Background
To compare the mid-term follow-up clinical efficacy among three treatment approaches for lumbar degenerative diseases (LDD): standalone oblique lumbar interbody fusion (SF), oblique lumbar interbody fusion combined with lateral screw fixation (LF), and oblique lumbar interbody fusion combined with posterior screw fixation (PF).
Method
This retrospective study included a total of 71 cases of single level LDD that underwent OLIF in Hospital of Chengdu University of Traditional Chinese Medicine were retrospectively collected between March 2016 and September 2017. Patients were divided into three groups: 24 cases in the SF group, 24 cases in the LF group and 23 cases in the PF group. Various parameters, such as operation time, hospitalization time, and complications, were recorded. The fusion condition was assessed at last follow up. Clinical outcomes were evaluated using the Visual Analogue Scale (VAS) and Oswestry Disability Index (ODI) from pre-operation to 5 years post-surgery.
Results
Significantly lower mean operation time and hospitalization time were observed in the SF and LF groups compared to the PF group (p < .05). However, no significant difference in fusion rate was found among the three groups. Regarding clinical outcomes, there was no statistically significant difference in VAS scores between the three groups during all follow-up periods. At the 6th month and 1st year after surgery, the SF and LF groups had significantly lower Oswestry Disability Index (ODI) scores compared to the PF group (p < .05). There was no significant difference in perioperative complication rates among the three groups (p > .05). In the LF group, one case of instrument displacement and urethra injury were reported, while in the SF, LF, and PF groups, 10, 9, and 3 cases of cage subsidence were reported, respectively.
Conclusion
The study findings suggest that oblique lumbar interbody fusion (OLIF) is a safe and effective treatment for mid-term management of lumbar degenerative diseases (LDD). Compared to the posterior screw fixation (PF) group, both the standalone OLIF (SF) and OLIF combined with lateral screw fixation (LF) groups showed advantages in terms of reduced operation time, shorter hospitalization, and faster symptom alleviation in the short-term. However, OLIF combined with PF demonstrated comparable symptom relief in the mid-term and had the additional benefit of lower cage subsidence rates while improving fusion rates as well.
Introduction
Lumbar degenerative diseases (LDD) encompass a range of conditions, including pure disc herniation, spinal stenosis, and degenerative lumbar spondylolisthesis, and are among the most common afflictions affecting the lumbar spine. The most prevalent clinical manifestations of LDD include low back pain and radiculopathy. LDD has become a significant societal issue, with a global incidence rate surpassing 43.1 percent of the population and continuing to rise each year.1,2 When conservative treatments fail to provide satisfactory results, surgical intervention is often considered as the optimal choice. Neural decompression and interbody fusion are the main surgical principles employed in the treatment of lumbar degenerative diseases. These surgical approaches aim to alleviate symptoms by decompressing nerves and stabilizing the affected spinal segment through fusion procedures.
With the rapid development of minimally invasive spine surgery techniques, various fusion approaches such as the tubular retractor technique, spine endoscopy, and microscope-assisted procedures have emerged.3–5 Among these approaches, Oblique Lumbar Interbody Fusion (OLIF), introduced in 2012, has become one of the most widely accepted surgical methods.6,7 OLIF offers several advantages, including preservation of lumbar spine stability, non-invasion of the spinal canal, and the ability to achieve indirect decompression by implanting a larger-sized cage to expand the foraminal area and straighten the buckled posterior longitudinal ligament and ligamentum flavum. 8 However, literature reports indicate that stand-alone OLIF procedures may lead to cage subsidence post-surgery, which can impact clinical efficacy.9,10 To address this issue, OLIF combined with internal fixation techniques has been developed to improve fusion rates, maintain lumbar biomechanical stability, and reduce stress on the end plates. 11 As a result, OLIF combined with lateral screw fixation and posterior screw fixation has gained more popularity in the surgical treatment of LDD. However, previous studies have mainly focused on the short-term clinical effectiveness of OLIF with different fixation methods. 12 To date, there have been no reports on the mid-term outcomes of OLIF with distinct fixation methods. Therefore, the present study aims to evaluate and compare the mid-term clinical efficacy of OLIF combined with three different fixation methods.
Methods
Study design
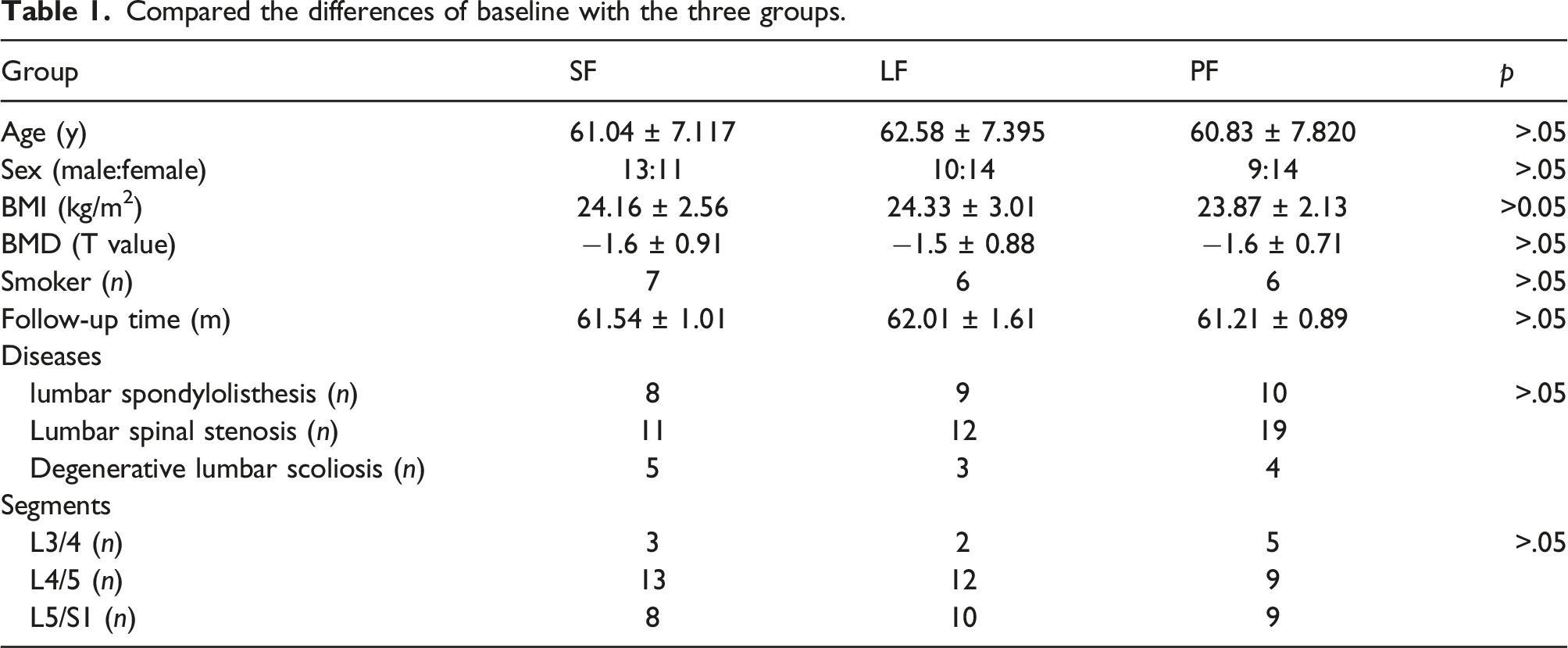
Compared the differences of baseline with the three groups.
Surgical procedure
SF group
In the OLIF procedure, patients were placed in a right decubitus (side-lying) position after receiving general anesthesia. The targeted level for surgery was identified using a C-arm for surface marking. Following routine disinfection and draping of the surgical site, a 2 cm incision was made using a scalpel. The layers of abdominal muscle were dissected using a Bovie cautery and hemostatic forceps, allowing access to the corridor between the psoas muscle and peritoneum where the tubular retractor could be docked. Once the corridor was established, the targeted intervertebral space was cleared using a pituitary grasper and curette to create a suitable graft bed. Finally, a cage with an appropriate size, filled with allograft bone, was inserted into the targeted intervertebral space. This step completes the OLIF procedure.
LF group
The preliminary steps were same to SF group. Additionally, the screws and plate was implanted at the lateral side of targeted upper and lower vertebras.
PF group
Following the initial steps of the OLIF procedure, the patient’s position was switched from the right decubitus position to the prone position. This change in position allows for access to the posterior aspect of the spine. Using C-arm fluoroscopy, the target pedicle (vertebral bone) was confirmed, and a guide wire was inserted into the pedicle. Through the guide wire, pedicle screws and connecting rods were then placed to provide stability and support to the treated segment of the spine.
Evaluation measures
During the study, the operation time and hospitalization time of the patients were recorded. Vertebral fusion was assessed by evaluating the presence of consecutively bridging trabecular bone connecting the target centrums on CT scans. 15 The fusion condition was evaluated independently by two residents and confirmed by an experienced attending surgeon during the final follow-up at the 5th postoperative year.
The clinical presentation of the patients was assessed using the Visual Analogue Scale (VAS) and the Oswestry Disability Index (ODI) from pre-operation to 5 years after surgery. These scales were used to evaluate pain levels and functional disability, respectively. 16 The study also monitored and recorded any complications that occurred, such as postoperative infections, instrument displacement, cage subsidence, and injuries to nerves, urethra, and peritoneum after surgery. These complications were closely observed and documented for further analysis and evaluation.
Statistical analysis
The collected data were analyzed using SPSS 25.0 software. Continuous variables were described using means and standard deviations. Statistical tests, such as analysis of variance (ANOVA), were employed to compare the differences in continuous variables among the different groups. The Chi-square test was used to compare the differences in categorical variables among the groups. In order to determine statistical significance, a p-value of less than 0.05 was considered as statistically significant, indicating that the observed differences were unlikely to occur due to chance alone.
Results
Operation time and hospitalization time
The mean operation time in the SF group was 49.42 ± 7.58 min, in the LF group it was 65.50 ± 4.21 min, and in the PF group it was 75.70 ± 3.62 min. There were statistically significant differences in mean operation time among the three groups (p < .05). The SF group had a shorter mean operation time compared to the LF group, and the LF group had a shorter mean operation time compared to the PF group. These differences in operation time suggest that the surgical complexity and the additional steps involved in the LF and PF groups increased the overall duration of the procedure.
Compared the differences of operation time and hospitalization with the three groups.

aCompare with the SF group, p < .05.
bCompare with the LF group, p < .05.
Fusion rate
Compared the differences of fusion rate with the three groups.


The follow-up radiological dates of the three groups. ((a)/(b), (e)/(f), (i)/(j)) The 3rd month after surgery in the three groups. ((c)/(d), (g)/(h), (k)/(l)) The 5th year after surgery in the three groups.
Clinical presentation
Visual analogue scale
Compared the differences of VAS with the three groups.

aCompare with the pro-operation, p < .05.
bCompare with the 3 months after surgery, p < .05.
cCompare with the 6 months after surgery, p < .05.
dCompare with 1 year after surgery, p < .05.
Oswestry disability index
Compared the differences of ODI with the three groups.

aCompare with the pro-operation, p < .05.
bCompare with the 3 months after surgery, p < .05.
cCompare with the 6 months after surgery, p < .05.
dCompare with 1 year after surgery, p < .05.
eCompare with 3 years after surgery, p < .05.
fCompare with the SF group, p < .05.
gCompare with the LF group, p < .05.
Complication
No cases of postoperative infection or nerve/peritoneum injury were reported in any of the three groups. However, in the LF group, one case of instrument translocation and urethra injury was observed (Figure 2). Additionally, cage subsidence occurred in 10 cases in the SF group, 9 cases in the LF group, and 3 cases in the PF group. No statistically significant differences were found in the occurrence of these complications among the three groups (p > .05), as indicated in Table 6. It is important to note that all patients who experienced complications received appropriate management and rehabilitation before being discharged from the hospital. The instrument translocation. Compared the differences of complications with the three groups.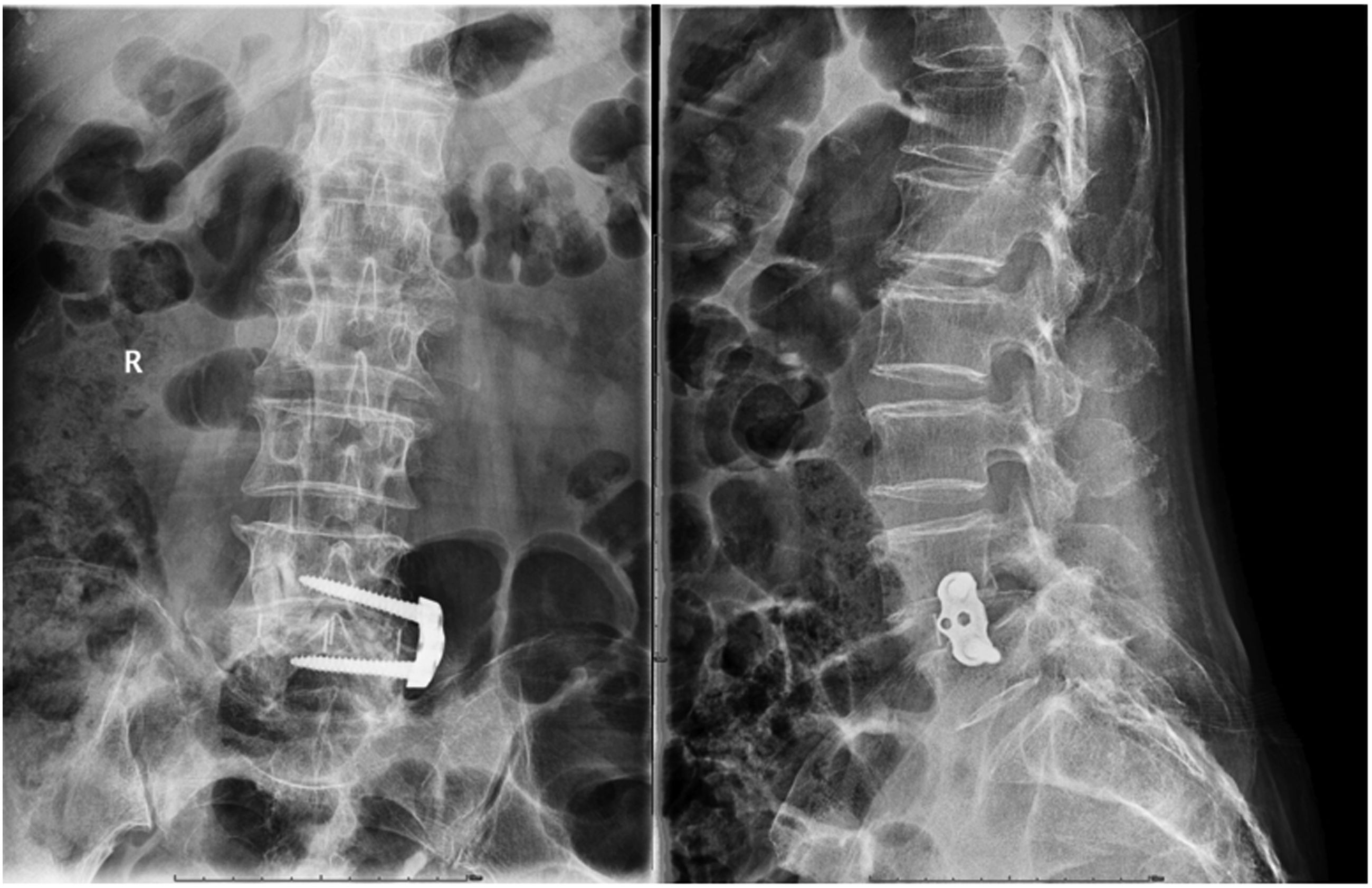

Discussion
The global aging population has led to a significant increase in the number of individuals diagnosed with LDD, reaching approximately 266 million worldwide. 1 As a result, LDD has become one of the most pressing public health concerns. While various lumbar interbody fusion techniques have been developed and applied successfully, they are also associated with a range of perioperative complications such as nerve injury and postoperative infection. 17 In comparison to traditional lumbar interbody fusion techniques, the OLIF technique offers several advantages. It reduces damage to the posterior spinal structures and allows surgeons to clear the intervertebral space more thoroughly. This enables the use of larger-sized cages for better indirect decompression and potentially increases the fusion rate to some extent.8,18,19 However, there has been ongoing controversy regarding the choice of fixation methods for OLIF. In a retrospective study by Song et al., 20 109 patients who underwent OLIF with either SF or PF were analyzed. The study demonstrated that SF had the advantage of saving operation time due to the maintenance of the patient’s position throughout the entire procedure. This finding suggests that SF may offer benefits in terms of surgical efficiency compared to PF in OLIF procedures. However, it is important to consider other factors such as postoperative outcomes and complication rates when evaluating the overall effectiveness and safety of different fixation methods in OLIF surgery.
On the other hand, SF has been validated as an acceptable fixation method from a biomechanical standpoint. 21 Lin et al. 22 conducted a prospective study involving 46 patients who underwent SF and reported a fusion rate of 81.9% at the first year postoperatively. Ge 23 conducted a retrospective study with a 1-year follow-up of 30 patients who underwent SF, and observed significant improvements in VAS and ODI scores compared to preoperative values. These studies confirmed that SF has a favorable fusion effect and can effectively alleviate clinical symptoms in the short-term. Guo et al. 24 assessed the stability of OLIF combined with various fixation methods using three-dimensional scanning models. They demonstrated that LFcou ld enhance the segmental stability at the fusion level and reduce contact stress on the endplates. Li et al. 25 retrospectively observed 37 patients who underwent LF for the first year postoperatively, showing significant improvement in VAS and ODI scores compared to preoperative values. They concluded that LF has the potential to alleviate clinical symptoms in patients. However, the high rate of cage subsidence associated with LF has raised concerns, leading to the consideration of posterior screw-rod system fixation.10,26 Fang et al. 11 compared SF with PF in an OLIF biomechanical study, demonstrating that PF could significantly disperse endplate stress, improve fusion rates, and reduce cage subsidence. Kim et al. 27 conducted a 1-year retrospective study and found that the fusion rate for OLIF with PF was 92.6%, with significant improvement in VAS scores in the first year postoperatively. They concluded that PF had an advantage in increasing fusion rates and relieving patient pain in the short-term. However, there are few clinical studies that directly compare the three commonly used fixation methods in OLIF, and long-term follow-up data are particularly limited. Further research is needed to comprehensively evaluate and compare the efficacy and safety of these fixation methods, especially in the long-term outcomes.
In the study, we conducted a comparison of the three most frequently used fixation methods in OLIF. The results revealed that the SF group had significantly shorter mean hospitalization and operation times compared to the PF group, which is consistent with previous literature. This indicates that SF offers advantages in terms of both time efficiency during the surgical procedure. Furthermore, our study demonstrated a consistent decline in postoperative VAS and ODI scores over the follow-up period compared to the pre-operative baseline. This indicates that all three fixation methods were effective in addressing the clinical symptoms associated with LDD in the mid-term. However, at the 6th month and 1st year after the surgery, the ODI scores of the SF and LF groups were significantly lower than those of the PF group. This suggests that both SF and LF fixation methods have short-term advantages in alleviating clinical symptoms compared to PF. Overall, the study suggests that all three fixation methods (SF, LF, and PF) can effectively address the clinical presentations of LDD patients and lead to favorable outcomes in the mid-term. However, SF and LF fixation methods appear to have short-term advantages in relieving clinical symptoms. These findings contribute to the existing knowledge and understanding of the different fixation methods used in OLIF procedures.
Cage subsidence has been widely recognized as the most common complication associated with OLIF.9,10,13 Despite preoperative assessments of cage size based on intervertebral space height, cage subsidence still occurred. The incidence of cage subsidence has been previously reported to be 22.41% for stand-alone cages and 5% for PF at the 1-year postoperative follow-up. 28 However, the results of our current study demonstrated a higher incidence of cage subsidence in both the SF and PF groups compared to the previous literature. 28 This difference could be attributed to the variation in observation time points. Our findings indicated that PF had advantages in terms of a lower rate of cage subsidence and maintaining stable regional fusion levels. Furthermore, no cases of postoperative infections or nerve/peritoneum injuries were observed in this study, which further supports the previous findings regarding the minimal invasiveness of OLIF and its ability to protect nerve tissue. However, one case of urethral injury observed in the LF group may have been caused by instrument extrusion during the operation. Additionally, one case of instrument translocation occurred in the LF group, potentially due to the improper size of the inserted cage. Therefore, it is crucial to place emphasis on careful preoperative measurements using CT scans and X-rays, as well as optimal intraoperative trials, to ensure the stability and success of the procedure.
Limitation
Indeed, the current study has several limitations that should be considered in future research. Firstly, being a long-term retrospective study tracing back to the time OLIF was initially implemented in practice, the sample size included was limited. This aspect may have implications for the generalizability of the findings. It would be beneficial to conduct larger-scale studies with a more diverse patient population to validate the results. Furthermore, unlike a randomized controlled trial, the retrospective nature of the study does not employ a randomized and blinded approach. This could potentially introduce selection bias and affect the accuracy of the results. Future studies could consider adopting a prospective design with randomization and blinding to minimize bias and enhance the validity of the findings. Addressing these limitations in future research would provide a more comprehensive understanding of the outcomes and potential complications associated with OLIF procedures.
Conclusion
The study findings suggest that oblique OLIF is a safe and effective treatment for mid-term management of LDD. Compared to the PF group, both the SF and LF groups showed advantages in terms of reduced operation time, shorter hospitalization, and faster symptom alleviation in the short-term. However, OLIF combined with PF demonstrated comparable symptom relief in the mid-term and had the additional benefit of lower cage subsidence rates while improving fusion rates as well.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent to participate was obtained from all of the participants in the study.