
Abstract
Background
Clavicle fractures are traditionally treated non-operatively. This study determines the functional outcome of midshaft clavicle fractures treated non-operatively, the factors influencing it, and the incidence of acromioclavicular joint (ACJ) arthrosis.
Methods
Patients with midshaft clavicular fractures treated non-operatively between 16 and 50 years old with no prior AC joint problems were assessed. Demographics, hand dominance, type of occupation, and smoking status were documented. Functional scoring using DASH score, CM score, and radiological evaluation was done with special tests to diagnose AC joint arthrosis. Two or more positive special tests were considered significant for this study.
Results
101 patients were recruited, 83 male and 18 female patients. The average age of 34.7 ± 13.93 years. The average follow-up was 32.7 months (range: 24–75; SD ± 9.9 months). 48.5% were blue-collar workers, and 60.4% involved the dominant upper limb. 44.6% were cigarette smokers. There was 20 mm and more shortening in 21.8% of subjects. 40.6% had a significant special test, and 36.6% had radiological changes of AC joint osteoarthritis. Positive two or more special tests were significantly associated with radiological evidence of arthrosis (p = .00). The mean DASH score was 28.28 ± 17.4, and the mean CM score was 27.58 ± 14.34. Most have satisfactory to excellent scores. Hand dominance, smoking, and blue-collar work were significantly associated with poorer CM scores, and hand dominance was significant for Dash scores.
Conclusion
There is an equal distribution poor, satisfactory and excellent functional outcomes in patients with midshaft clavicle fractures treated non-operatively. The poor outcomes may be attributed to ACJ arthrosis. Hand dominance, smoking and blue-collar work affected the functional outcome. Shortening of the clavicle had no bearing on the clinical and radiological findings of osteoarthritis and functional scores. The presence of two or more positive special tests is an accurate predictor of AC joint arthritis.
Introduction
A clavicle fracture is a common fracture that accounts for 5% of all adult fractures. 1 Clavicle fractures are generally treated non-operatively with a simple arm sling or figure of eight bandaging, but this trend is gradually changing towards surgical fixation. Non-operative treatment has been the standard accepted treatment. The primary objective was union and restoration of range of motion.2–5 However, many reports, including clinical trials, have emerged over the last two decades, associating poor functional outcomes in patients treated non-operatively. These reports showed a 31% unsatisfactory outcome, mainly attributed to the clavicle’s non-union and malunion.1,2,6–15
Therefore, addressing the non-union would likely improve functional outcomes, but these results are mixed and based on some small case series.4,14–16 We postulate that one of the reasons contributing to the poor outcome is the development of acromioclavicular joint (ACJ) arthrosis.
Acromioclavicular joint is a diarthrodial joint with an intervening fibrocartilaginous disc and is stabilised by the articulating surfaces and joint capsule shape. The joint capsule is reinforced by the superior and inferior acromioclavicular ligaments and coracoclavicular ligaments.4,17 Shoulder movements occur in ACJ and three other joints around the shoulder, namely the glenohumeral, sternoclavicular, and scapulothoracic joints. They can occur alone in each joint or synchrony to provide a smooth and accurate upper limb movement. Disruption in any of these joints may cause an abnormal shoulder motion and affect the performance of upper limb activities.4,18 The disruption of ACJ can be secondary to septic arthritis, rheumatoid arthritis, distal clavicle osteolysis, ACJ instability, and posttraumatic arthropathy. 18 In clavicle fractures, the most common mechanism of injury is compressive loading, and this may, in turn, affect the integrity of the intervening disc.1,4,18 Acting like a meniscus in the knee, a large enough load may cause it to fray and form holes, eventually exposing and degenerating the cartilage of articulating surfaces.18–20 Moreover, a clavicle fracture that has healed not at its anatomical position could create a lower force-generating capacity over the shoulder girdle muscles and increase stress on the ACJ and glenohumeral joint, leading to lower force-generating power for early degeneration across the joint. 21
This study determines the functional outcome of midshaft clavicle fractures treated non-operatively, the factors affecting them, and the incidence of posttraumatic acromioclavicular joint (ACJ) arthrosis.
Methodology
Study design and sample population
This cross-sectional study involves patients who sustained mid-shaft clavicle fractures due to trauma. We included patients with united clavicle fractures aged 16 to 50 who received non-operative treatment and had been followed up for at least 24 months after the primary injury. We excluded patients with pathological fractures, ACJ instability, bilateral clavicle fractures, shoulder pain before the clavicle fracture, and those with underlying inflammatory conditions such as rheumatoid arthritis or systemic lupus erythematosus. The hospital’s ethical committee approved this study (MECID No: 201511-1863). The patients were recruited from the outpatient clinic for consultation for a different medical problem, and those who came for assessment for insurance-related medical reports. Consent was obtained once they fulfilled the inclusion criteria.
Diagnosing ACJ arthrosis
These patients generally present with progressively worsening shoulder pain during strenuous activities or minor trauma, which may cause acute exacerbation of the pain. The pain is usually localised over the ACJ region but can affect a wider area between the shoulder’s superolateral aspect and the anterolateral aspect of the arm. Occasionally, the pain might radiate into the base of the neck or forearm.22,23 Pain at the shoulder’s posterior part is usually associated with pathologies from the cervical spine. 23 Overhead activities, weightlifting, and cross-body movements using the affected arm are often associated with worsening symptoms.16,23 In addition to that, patients might also complain of catching, grinding, or popping the ACJ. 16
Several special physical examinations and clinical diagnostic tests have been developed to diagnose ACJ pathologies. These include eliciting local tenderness at the acromioclavicular joint and having patients’ pain exacerbated by specific provocative tests such as cross-arm adduction test (Scarf’s Test), active compression test, or O’Brien’s Test, acromioclavicular resisted-extension test, and Paxino’s test.24,25 Scarf's test has the highest sensitivity at 77%, whilst O’Brien’s test has the highest specificity at 95%. 24 For this study, we considered two or more positive tests as clinically significant.
A plain radiograph was carried out in radiological assessment to diagnose ACJ arthrosis. The formation of osteophytes, subchondral cysts, reduced joint space, and subchondral sclerosis suggest ACJ arthrosis. 26 A comprehensive radiographic assessment of the shoulder joint should include an anterior-posterior view of the chest and shoulder, including Grashey’s, Zanca, and axillary lateral view. 18 Other modalities that could reveal ACJ pathologies include magnetic resonance imaging (MRI), computed tomography (CT), and ultrasonography. However, these should not supersede excellent clinical judgment.18,26 In this study, we did not conduct ultrasound, CT and MRI due to cost and logistic reasons.
Data collection
We recorded patients’ demographics, hand dominance, type of occupation (blue-collar or white-collar workers) and smoking status as potential factors affecting their outcomes. Patients were then assessed both clinically and radiographically for ACJ arthrosis. We used radiographs to evaluate degenerative changes of the ACJ and any shortening of the united clavicle. The method proposed by Smekal et al.
27
was used to measure the united clavicle’s proportional length based on a posteroanterior thorax radiograph, as shown in Figure 1. For this study, we divided our subjects into two groups: those with a shortening of less than 2 cm and those with a shortening of 2 cm and greater. This is based on reports by McKee et al.
11
and Hill et al.,
13
who reported unsatisfactory results in subjects with clavicular shortening greater than 20 mm in cases treated non-operatively.
28
Proportional length differences by taking a posteroanterior thorax radiograph to look for clavicular shortening. This radiograph shows that the right clavicle is 10 mm shorter than the left clavicle.
Shoulder function was assessed using the Disabilities of the Arm, Shoulder and Hand (DASH) and Constant Murley (CM) scores. The DASH score was divided into Excellent (score 0–5), Good (score 6–45), Satisfactory (score 15–35) and Poor (score >35). 20 Both shoulders were evaluated for CM scoring to compare the normal and affected sides. 29 Shoulder function was graded as poor (score >30), fair (score 21–30), good (score 11–20), and excellent (score <11).
Statistical analysis
The statistical analysis was done with SSPS (Statistical Package for the Social Sciences) version 27. Frequencies and percentages were used to describe the study population, incidence of special test and radiological findings, and functional scores (DASH and CM scores). The functional scores' normality was analysed with Kolmogorov-Smirnov and was not normally distributed. Hence, the Mann-Whitney Rank U test was used to analyse the relationship between special tests and radiological changes, DASH and CM. Chi-square statistics describe the association between risk factors and functional scores. A similar analysis assessed the association between special tests, radiological changes and clavicle shortening. As for the continuous data set, the means, standard deviation, and range were reported. The statistical significance is a p-value less than 0.05 (p < .05).
Results
Patients demographics
Demographic profile (N = 101).

Special test
Shows the incidence of special test and radiological findings.

Shows association between Special test and clavicle shortening.

Shows association between special test and radiological changes of AC joint osteoarthritis.

Shows the relationship between special tests and DASH/CM scores.

Shows association between shortening and radiological changes of AC joint osteoarthritis.

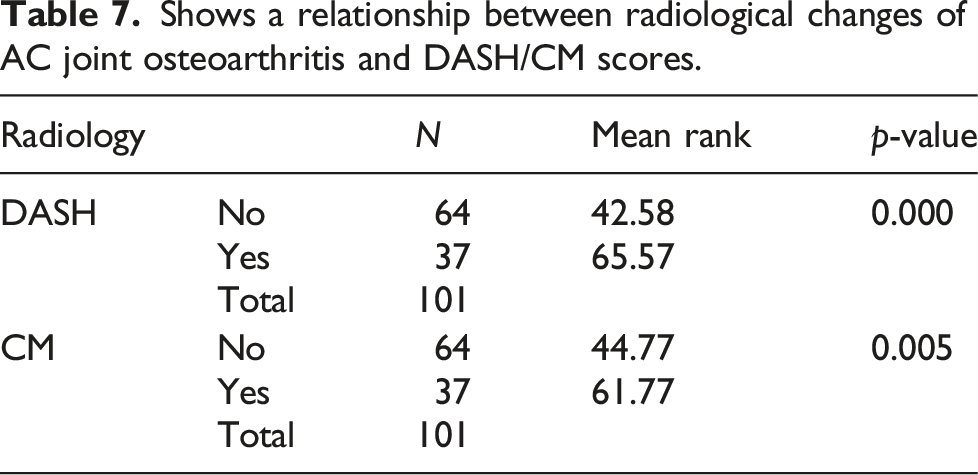
Shows a relationship between radiological changes of AC joint osteoarthritis and DASH/CM scores.
Patient-oriented outcomes
The disabilities of the arm, shoulder and hand (DASH) outcome score.

The constant-murley shoulder outcome score.

Association between risk factors and constant-Murley shoulder score grading.

Significant: *p < .05, **p < .01.
Association between risk factors DASH score grading.

Significant: **p < .01.
Discussions
This study shows an almost equal distribution of patients with poor, satisfactory and excellent outcomes based on DASH and CM scores. The mean DASH score in this study was 28.6 (±17.5), which is higher than a “normal” population. 24 McKee et al. studied 30 patients who were followed up for at least 1 year and detected residual deficits in shoulder strength and endurance among patients with displaced mid-shaft clavicle fractures. The mean DASH score in his study was 24.6, indicating a certain amount of residual disability. 11 He had also reported a higher DASH score in an earlier study on malunited clavicle fractures (32 points). He attributed it to various degrees of pain, including radiating type pain to the forearm, weakness, and difficulty doing prolonged physical activities. 30 We found that the involvement of the dominant hand was related to a poor DASH score. Other factors, such as the location of the fracture, smoking, clavicular shortening, and type of occupation, did not show a significant association.
We observed a similar pattern with the CM score. We found that smoking, blue-collar workers, and involvement of the dominant hand were related to poor CM scores. The functional outcome assessed with the CM scores in clavicle fractures treated non-operatively is sparse in the literature, with many case series only reporting post-operative CM scores. 4 Therefore, we are unable to make a direct comparison.
Our study concurs with literature reports showing a poor functional outcome in malunited clavicle fractures.4,14 These poorer outcomes may be attributed secondary to AC joint arthrosis. However, the incidence of ACJ arthrosis after clavicle fractures is not well documented.
Studies to determine the association between clinical outcomes and clavicle shortening have also been inconsistent. Eskola et al. reported that patients with shortening or primary displacement of more than 15 mm had significantly more pain than those without shortening or displacement. 31 Lazarides S et al. found that final clavicle shortening of more than 18 mm in male and 14 mm in female patients was associated with significantly unsatisfactory results. 32 However, Oroko et al. could not prove any significant link between clavicle shortening and shoulder function. They did note that three of the lowest CM scores came from patients with severe clavicle shortening. 33 As stated earlier, McKee et al. 11 and Hill et al. 13 reported unsatisfactory results following clavicular shortening of greater than 20 mm following displaced midshaft clavicle fractures treated non-operatively. However, we found that 20 mm shortening or more does not correlate to two or more positive special tests, worsening of the functional outcome represented by the DASH and CM shoulder score or radiological evidence of AC joint osteoarthritis.
In our study, there is a significant association between the presence of two or more Special tests and radiological evidence of arthrosis with poor functional outcomes represented by the DASH and CM scores, establishing the accuracy of predicting the presence of AC joint arthritis with two or more positive special tests.
We are the first to report incidence, severity, and risk factors for posttraumatic ACJ arthrosis in young adults who achieved the clinical and radiographic union of clavicle fractures treated non-operatively. In our series, 40.6% of subjects had two or more positive special tests overall. And 36.6% of subjects had radiological changes of AC joint osteoarthritis. This is in keeping with the findings by Cadogan et al., who showed that ACJ arthrosis is higher in patients with clavicular fractures than in individuals without clavicle fractures. The prevalence of ACJ degeneration in patients who presented with shoulder pain in a primary care setting was 17%. 34 Akbar et al. reported a slightly higher prevalence of 26%. 21
Study limitations
Since this study is cross-sectional, we could only exclude patients with prior shoulder injuries based on history. Before the injury, no shoulder radiograph was taken to rule out preexisting acromioclavicular joint (ACJ) arthrosis. Furthermore, ACJ arthrosis diagnostic criteria may not be accurate as there may be a mismatch between radiology and clinical findings. ACJ arthrosis also occurs in middle-aged subjects who do not have clavicle fractures.
Another limitation of this study is the patient response bias. Patients with poor functional outcomes were more likely to respond to the questionnaire, given their ongoing frustrations related to shoulder dysfunction. The diagnosis of ACJ arthrosis is based on history, clinical examination, and plain radiographs. However, radiological diagnosis of AC joint arthritis may not translate to clinically symptomatic arthritis. Although studies demonstrated combinations of physical tests to improve the accuracy of diagnosing ACJ lesions, they could only achieve a sensitivity of 81% and specificity of 89% by combining two or more positive tests. However, the negative predictive value of combining two or more tests is 99%. 26 MRI, CT scans, and Ultrasound could have been used to improve the accuracy of ACJ joint arthritis, but it was not carried out in this study due to cost constraints. Lastly, we considered both simple and comminuted midshaft fractures in the group and did not distinguish between the two. This may have a bearing on the outcome where the comminuted fractures theoretically can give a worse outcome than simple fractures due to the force of the injury.
In summary, there is an equal distribution of patients with midshaft clavicle fractures treated non-operatively with poor, satisfactory and excellent functional outcomes. This may be attributed to ACJ arthrosis. Hand dominance, smokers and blue-collar workers were the only factors that affected the functional outcome. The presence of two or more positive special tests is an accurate predictor of AC joint arthritis. Shortening of the clavicle had no bearing on the clinical and radiological findings of osteoarthritis and functional scores.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.