
Abstract
Purpose
Knee osteoarthritis (OA) may be comorbid with diabetes mellitus (DM), and physical activity is a recommended lifestyle strategy for both diseases. The present study investigated the physical activity differences by intensity between knee OA patients with or without DM, and evaluated if physical activity was associated with the presence of DM in knee OA patients.
Methods
A total of 183 patients (mean age 74.9 ± 6.4 years) with moderate-to-severe knee OA underwent evaluation of knee function (i.e., knee flexion/extension range-of-motion, knee-extension muscle strength, and knee pain), the timed up-and-go (TUG) test, and physical activity measurement using an accelerometer. Physical activity by intensity was compared between knee OA patients with and without DM. The association between physical activity, including knee function and the TUG test time, and DM was assessed.
Results
The 2 groups (with or without DM) did not differ significantly in knee OA severity or age. Compared to knee OA patients without DM, knee OA patients with DM had a significantly lower average daily step count (p < 0.001), and significantly shorter times spent performing light-intensity physical activity (LPA; p < 0.001) and moderate-to-vigorous-intensity physical activity (MVPA; p = 0.006). After adjusting for age, sex, and body mass index, we found that a lower average daily step count and shorter LPA time significantly correlated with DM (β = −0.200, p = 0.006; β = −0.216, p = 0.004, respectively) and a longer TUG test time (β = −0.196, p = 0.014; β = −0.208, p = 0.011, respectively). A shorter MVPA time significantly correlated with lower contralateral knee-extension muscle strength (β = 0.187, p = 0.032).
Conclusion
Knee OA patients with DM had significantly lower physical activity levels than those without DM. Furthermore, the presence of DM correlated with a lower step count and a shorter LPA time in knee OA patients.
Introduction
Knee osteoarthritis (OA), a major cause of pain, disability, and socioeconomic loss, is the most common degenerative joint disease, and contributes to the increasing burden of disease worldwide.1,2 The severe pain experienced by knee OA patients often limits their daily physical activities. Based on objective measurements, most patients, especially those with moderate-to-severe knee OA, are physically inactive, spending the majority of their day sitting,3,4 with only ∼13% achieving the generally recommended level of activity. 3 Total knee arthroplasty (TKA) is considered the most effective treatment for end-stage knee OA. 5 TKA is expected to restore joint function, while reducing severe pain and functional disability, 6 thereby improving quality and quantity of physical activity of knee OA patients, and decreasing the number of years with disability. Contrary to expectations, a recent systematic review of physical activity in patients with knee OA, however, demonstrated that physical activity remains at the preoperative level 1 year after surgery in most patients who undergo TKA.7,8
In recent years, research on knee OA has emphasized the potential involvement of metabolic syndrome risk factors, including dyslipidemia and type 2 diabetes mellitus (DM). 9 A phenotype specific to knee OA patients with DM, “diabetes-induced OA”, has been defined. 10 Both DM and knee OA are extremely common conditions globally; approximately 260 million individuals of all ages are affected by knee OA and approximately 250 million people have type 2 DM; 11 14.4% of knee OA patients have DM. 12 Although obesity confounds these 2 diseases, there are no reports of the involvement of obesity in the association between knee OA and DM. 13
Patients with type 2 DM often do not adequately engage in physical activity.14,15 The physical activity levels may thus be even lower in patients with both type 2 DM and moderate-to-severe knee OA than in those with either DM or knee OA alone. Studies of patients with DM who have undergone TKA reported no change in blood glucose and hemoglobin A1c (HbA1c) levels.16,17 In these studies, however, physical activity was investigated using only questionnaires or was not investigated at all. Boulé et al. 18 found that the HbA1c level decreases in type 2 DM patients as exercise intensity increases. Frimpong et al. 19 reported that light-intensity physical activity (LPA) in knee OA patients improved 6 months after TKA, whereas moderate-to-vigorous-intensity physical activity (MVPA) did not. To the best of our knowledge, the impact of DM on physical activity levels in patients with knee OA has not been reported. Physical activity should be increased in knee OA patients with DM after TKA, especially at moderate-to-vigorous-intensity. For comparison of physical activity levels after TKA, it is important to determine pre-TKA levels.7,8
The present study investigated the physical activity differences by intensity between knee OA patients with or without DM, and evaluated if physical activity was associated with the presence of DM in older patients with moderate-to-severe knee OA before TKA. We hypothesized that patients having both knee OA and DM would be less physically active than those without DM, and that the level of MVPA would be decreased in knee OA patients with DM.
Materials and methods
Patients
This exploratory, cross-sectional study enrolled older patients who were radiographically diagnosed with knee OA (i.e., Kellgren‒Lawrence [KL] grade ≥2 in 1 or both knees)
20
from the TKA scheduling list at the Orthopaedic Clinic. Patients were included if (1) they were scheduled to undergo TKA from July 2018 to July 2019; (2) they were able to walk independently on a flat surface with or without an assistive device; and (3) those with DM had an HbA1c level ≤8.0%, no macrovascular comorbidities (coronary artery disease, myocardial infarction, stroke, congestive heart failure, and peripheral vascular disease) or microvascular comorbidities (retinopathy, nephropathy, and neuropathy), and were not receiving insulin injections (i.e., the criteria for eligibility for TKA). The side with the highest KL grade (in cases with the same grade, the most symptomatic side) was considered the “affected” side in patients scheduled to undergo bilateral TKA. The exclusion criteria were as follows: (1) cognitive impairment, (2) neurologic problems, (3) history of surgical treatment for a fracture in the lower extremity and/or spine, or (4) no consent. In total, 227 patients met the inclusion criteria from July 2018 to July 2019. The process for inclusion in the analysis is shown in Figure 1. A total of 183 patients (mean age 74.9 ± 6.4 years, 28 men, 155 women) were included in the analysis, and 44 patients were excluded: 1 patient had a neurologic problem, 3 patients had a history of surgical treatment for a fracture in the lower extremities, and 40 patients were unable to provide consent. Flow diagram of the inclusion/exclusion criteria for the analysis.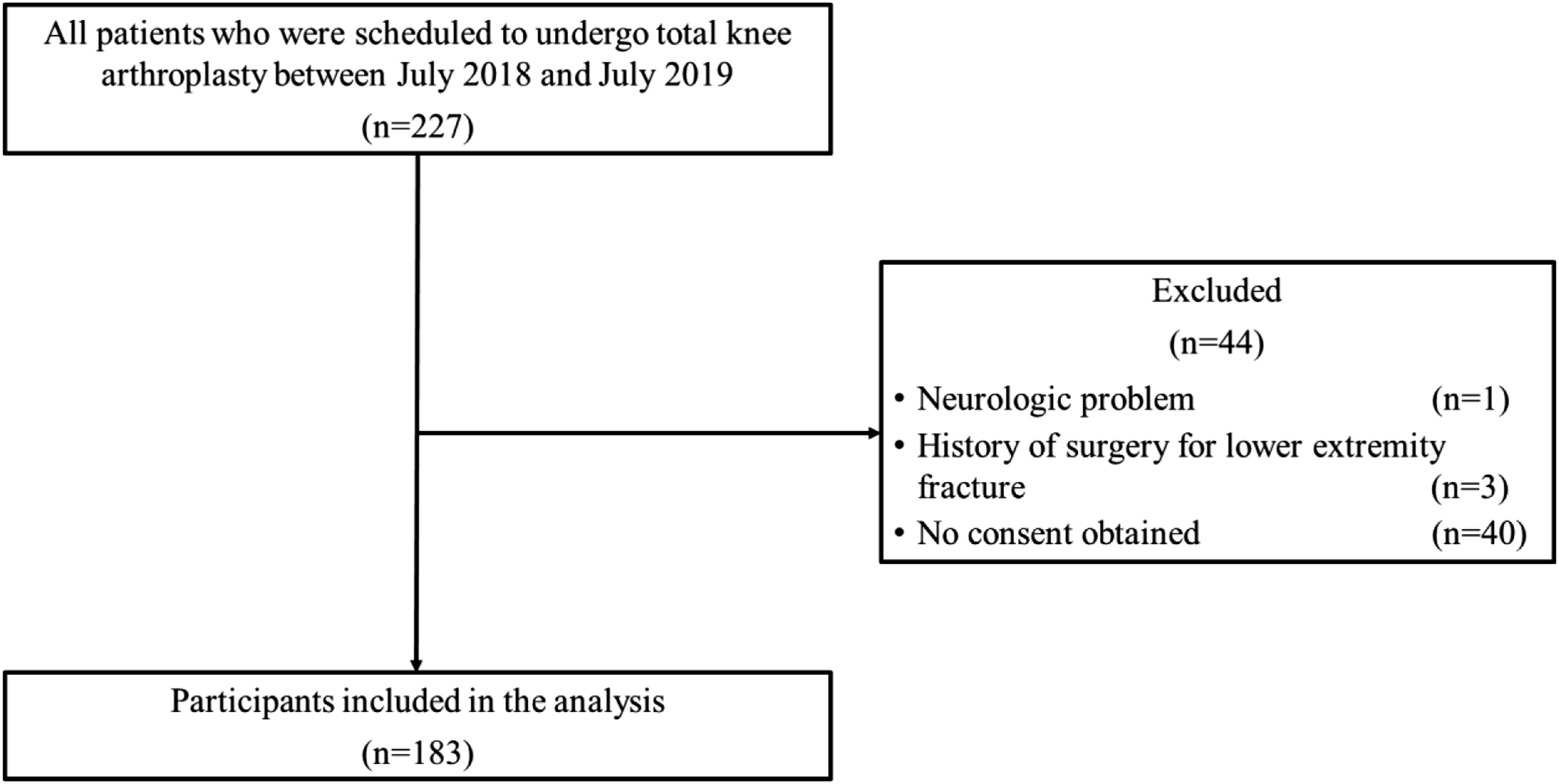
The Ethics Committee of Seijoh University (approval no. 2018A0006) and Nagoya University (approval no. 20-521) approved the study. All patients provided written informed consent.
Measures
All clinical data were collected 1‒4 weeks before TKA. Outcome measurements evaluated for all patients were as follows: knee function (i.e., knee flexion and extension range-of-motion [ROM], knee-extension muscle strength, and knee pain), performance-based physical function (measured with the timed up-and-go [TUG] test), and objectively measured physical activity.
Knee function
Knee flexion and extension ROM were assessed as the angle formed by the intersection of the mechanical axes of the femur (i.e., the line from the greater trochanter to the lateral femoral epicondyle) and lower leg (i.e., the line from the head of the fibula to the lateral malleolus of the fibula). With patients positioned supine, passive knee flexion and extension ROM were measured using a standard goniometer.
Knee-extension muscle strength was measured during isometric contractions using an isometric dynamometer (Isoforce GT-360; OG Wellness Technologies Co., Ltd., Okayama, Japan). Patients were seated upright on the dynamometer while flexing the knee of the tested limb at a 60° angle. Chair depth, height, placement, and length of the attachment arm were adjusted for each patient. Patients were secured with straps at the distal shank, mid-thigh, pelvis, and trunk. Maximum contractions were attained within 3 s and maintained for 5 s. Standardized verbal encouragement was provided to elicit maximal effort from each patient, and the maximum knee-extension muscle strength values were recorded. Each patient underwent 2 trials. The maximum muscle strength of the 2 trials was then normalized to the body weight and used for data analysis. A 100-mm visual analog scale for pain was used to measure the pain intensity in the affected and contralateral knees during the preceding week.
Performance-based physical function measure
Performance-based physical function was objectively assessed according to an activity recommended by the Osteoarthritis Research Society International: time taken to perform the TUG test (i.e., ambulatory transitions). The TUG test 21 is a simple, commonly used, and reliable test for clinical application in patients with suspected knee OA.22,23 Patients were instructed to stand from a seated position (seat height of 40 cm), walk out and back 3 m at a normal speed, and then return to a seated position without physical assistance (although assistive devices could be used, if necessary). The time to perform this test was measured once using a stopwatch.
Physical activity
Physical activity was measured for 14 consecutive days with a uniaxial accelerometer (Lifecorder; Suzuken Co., Ltd., Nagoya, Japan) widely used in Japan and worldwide.24–26 Patients were given both oral and written explanations regarding proper use of the accelerometer. The accelerometer was attached at waist level just above 1 leg and kept on throughout the day. It was to be removed only for sleep and water-related activities, such bathing, showering, and swimming. To be included in the study, the participants had to wear the accelerometer for 10 h/d for ≥4 days (including 1 weekend day). 27 “Nonwear time” was defined as a period of at least 60 consecutive minutes when body movement data were not recorded, except for up to only 2 min of limited movement. 27 The accelerometer data were edited and aggregated using physical activity analysis software (LifeLyzer05 Coach; Suzuken Co., Ltd., Nagoya, Japan). Based on the 11 exercise intensity levels from the accelerometer data (the device records a signal at an intensity level of 0, 0.5, or 1–9 every 4 s while being worn), physical activity intensities were classified as light (i.e., intensity level 1–3; ≥1.5 to <3 metabolic equivalents [METs]), moderate (i.e., intensity level 4–6; ≥3 to <6 METs), or vigorous (i.e., intensity level 7–9; ≥6 METs). 24 The average daily step count (in steps/d) and time spent in physical activity at the respective intensity were calculated. Nearly 70% of the patients accumulated no time spent in vigorous-intensity physical activity; therefore, a single variable was constructed combining the time spent in moderate activity with the time spent in vigorous-intensity physical activity. 28
Demographic characteristics and laboratory data
Data on age, sex, height, weight, radiographic OA severity, and laboratory data (e.g., HbA1c, fasting plasma glucose, triglycerides, total cholesterol, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol) were collected from the clinical records. Body mass index (BMI) was calculated by dividing the weight by the square of the height. The radiographic OA severity in the tibiofemoral joint based on KL grades 20 was assessed for each patient in the anteroposterior and weight-bearing position by a trained examiner (orthopedist). DM was defined as an elevated fasting plasma glucose level ≥126 mg/dL, HbA1c level ≥6.5%, history of a physician’s diagnosis of DM, or the use of antidiabetic medications. 29
Data analyses
The sample size was calculated as the number of all eligible patients visiting the clinic during the study period. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, NY, USA). All patients were categorized into 2 groups (with DM or without DM) and the outcome variables were each compared between groups using Student’s t-test for comparison of parametric continuous variables and the Mann‒Whitney U test for comparison of nonparametric continuous variables. The chi-square/Fisher’s exact test were used for comparisons of dichotomous/categorical variables. The normality of the continuous variables was determined by the Shapiro‒Wilk test. Levene’s test was used to confirm the homogeneity of variance of all parametric continuous variables between groups. Descriptive statistics were calculated as the mean±standard deviation for continuous variables and as proportion for dichotomous/categorical variables.
Additionally, the effect size (ES) of the differences between the 2 groups was calculated. ES calculated by Student’s t-test was interpreted as follows: <0.2 = trivial, 0.2–0.5 = small, 0.5–0.8 = medium, and >0.8 = large. 30 ES calculated by the Mann‒Whitney U test was interpreted as follows: <0.1 = trivial, 0.1–0.3 = small, 0.3–0.5 = medium, and >0.5 = large. 31
A hierarchical multiple linear regression analysis was conducted with physical activity parameters (e.g., average daily step count, and time spent in LPA and MVPA) as the dependent variables to evaluate the effect of DM on physical activity in patients with knee OA, while adjusting for age, sex, and BMI. These adjustment variables were selected a priori based on clinical judgment due to their potential influence on physical activity. 32 The independent variable was DM (0 = without DM, 1 = with DM), and knee pain, knee flexion/extension ROM, and knee-extension muscle strength were simultaneously included in the model. The independent variables were selected a priori based on clinical judgment due to their potential influence on physical activity and knee OA.33,34 Each model had 2 steps. In step 1, the adjustment variables were included using the forced-entry method. In step 2, DM, knee pain, knee flexion/extension ROM, and knee-extension muscle strength were further included using the stepwise method. All independent variables were screened for multicollinearity by calculating the variance inflation factor. The independence of residual errors was assessed using the Durbin‒Watson statistic, which revealed independence in the range of 1.5‒2.5. The standardized partial regression coefficient (β) was used to interpret the significance of correlations. A p value <0.05 was considered statistically significant.
Results
Among the 183 knee OA patients, 46 (25.1%) patients had DM with an HbA1c level of ≤8.0%. Furthermore, 43 (23.5%) patients had an operated knee on the contralateral side.
Summary of the characteristics of knee osteoarthritis patients with and without diabetes mellitus.

Note: Statistically significant p values are shown in bold font. Effect size (ES): <0.1 = trivial effect, 0.1–0.3 = small effect, 0.3–0.5 = medium effect; and >0.5 = large effect.
BMI, body mass index; OA, osteoarthritis; DM, diabetes mellitus; HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-density lipoprotein; ROM, range-of-motion; VAS, visual analog scale; TUG, Timed Up-and-Go; LPA, light-intensity physical activity; MVPA, moderate-to-vigorous-intensity physical activity; SD, standard deviation.
aBased on unadjusted analysis (Student’s t-test [weight, BMI, HbA1c, and knee-extension muscle strength on both side] or Mann‒Whitney U test [age, height, fasting plasma glucose, triglycerides, total, HDL and LDL cholesterol, knee flexion and extension ROM on both side, knee pain on both side, TUG test time, average daily step count, time spent in LPA, and time spent in MVPA] or the chi-square test [sex]) between OA patients with and without
DM. Non-normality of continuous variables was assessed using the Shapiro‒Wilk test (p < 0.05); these variables were analyzed using the Mann‒Whitney U test.
Effect of diabetes mellitus on the average daily step count.

Note: B is the partial regression coefficient and β is the standardized partial regression coefficient. Statistically significant p values are shown in bold font.
BMI, body mass index; DM, diabetes mellitus; TUG, Timed Up-and-Go.
Effect of diabetes mellitus on the time spent in light-intensity physical activity.

Note: B is the partial regression coefficient and β is the standardized partial regression coefficient. Statistically significant p values are shown in bold font.
BMI, body mass index; DM, diabetes mellitus; TUG, Timed Up-and-Go.
Effect of diabetes mellitus on the time spent in moderate-to-vigorous-intensity physical activity.

Note: B is the partial regression coefficient and β is the standardized partial regression coefficient. Statistically significant p values are shown in bold font.
BMI, body mass index.
The variance inflation factor was <10, indicating that no collinearity existed among the variables and that none of the significant relationships were inflated by correlations between independent variables. 35 Residual plots indicated a random distribution pattern. Independence was observed among the residual errors of average daily step count, time spent in LPA, and time spent in MVPA (Durbin–Watson statistic was 1.937, 1.912, and 1.936, respectively). These findings demonstrated the validity of the multivariate regression analysis results in the present study.
Discussion
In the present study, we compared the physical activity levels in patients with moderate-to-severe knee OA and with or without DM to determine whether the physical activity level and DM were associated. Physical activity was lower among knee OA patients with DM than among those without DM. After adjusting for age, sex, and BMI, a lower average daily step count and a shorter LPA time correlated with the presence of DM and a longer TUG test time, whereas the MVPA time correlated with knee-extension muscle strength on the contralateral side.
The prevalence of DM in patients with knee OA was 14.4% in a meta-analysis that included studies published before 2010, but the prevalence reported in individual studies since 2010 range from 5.2% to 38.0%. 12 The prevalence in the present study was 25.1%, which is higher than the 14.4% reported by Louati et al., 12 but within the range of prevalence in the studies reported after 2010. Thus, the patients in this study were similar to participants in other studies of knee OA and DM.
The LPA time was 32.9% lower and the MVPA time was 44.4% lower in knee OA patients with DM than in those without DM. Individuals whose activity is limited to remaining inside the home take approximately 4000 steps/day and engage in less than 5 min/d of MVPA.36–38 In this study, the average daily step count was 4656 steps among patients without DM and 3122 steps among those with DM. Moreover, the MVPA time was 4.5 min/d among patients without DM and 2.5 min/d among those with DM. Both groups engaged in MVPA <5 min/d, and MVPA time was particularly low for patients with DM. These findings highlight the high level of inactivity of knee OA patients with DM.
The TUG test time correlated with the step count and LPA time in addition to DM. The TUG test time is an appropriate clinical measure of functional mobility and balance. 39 Patients with balance-related disabilities most often exhibit impairments in standing balance, have slow walking speeds, and/or are unable to perform the chair stand test. 40 In patients with knee OA, mobility and gait limitations are factors that can lead to insufficient activity. 41 Based on the TUG test results in the present study, patients with knee OA tend to decrease their step count and LPA time as their mobility and balance decrease.
On the other hand, in contrast to our hypothesis, the MVPA time correlated with knee-extension muscle strength on the contralateral side, and not with DM. A previous study on the effect of knee-extension muscle strength on MVPA time reported that increased MVPA time, but not LPA time, correlated with higher knee-extension muscle strength in middle-aged women. 42 Aoyagi et al. 24 reported that knee-extension muscle strength significantly positively correlated with the daily step count and MVPA time in older people. Later research demonstrated that lower-limb muscle mass was more closely associated with MVPA time than with the daily step count. 43 Furthermore, the patients in this study had higher knee-extension muscle strength on the contralateral side than on the affected side (Table 1), suggesting that activities focused on the contralateral side could improve the activity levels of these patients. These findings indicate that patients with both knee OA and DM have difficulties maintaining MVPA because of reduced knee-extension muscle strength on the contralateral side rather than because of DM.
Comparison of the groups with and without DM revealed that among knee functions, only ROM was significantly more limited in the group with DM than in the group without DM, despite the absence of significant differences in severity (KL grade) or age. The main factors affecting joint mobility in DM are increased stiffness of the joint capsules, ligaments, and tendons for which the underlying mechanism involves nonenzymatic glycosylation of collagen, accompanied by the formation of advanced glycated end-products. DM is also associated with increased collagen in the muscles and reduced contractility of the muscle fibers, 44 suggesting that DM limits knee ROM. Miner et al. 45 reported that satisfaction and quality of life of patients who underwent TKA did not correlate with knee ROM. Robertson et al. 46 reported that knee ROM at 1‒10 years after TKA was worse in patients with DM, even though the Knee Society Scores did not change. These findings may explain why knee ROM did not correlate with physical activity in the hierarchical multiple regression analysis in the present study.
Recommended nonsurgical treatments for knee OA are exercise therapy such as muscle strengthening, aerobic exercise, and balance training; the use of walking aids; and patient education, including advice on achieving a healthy lifestyle, such as maintaining regular physical activity.47,48 In TKA patients, physical activity at 1 year after TKA reportedly remains at preoperative levels.7,8 In particular, knee OA patients with DM have significantly lower physical activity levels, which raises concerns about postoperative physical inactivity. Rehabilitation to increase physical activity in knee OA patients with DM is important, both before and after TKA.
A strength of this study is that the physical activity of patients with knee OA and with and without DM was objectively measured using an accelerometer. Most previous studies investigated physical activity using questionnaires or not at all. We believe that our study is the first to investigate the physical activity of patients with moderate-to-severe knee OA and DM. Nevertheless, this study has several limitations that must be considered. First, the study included patients with moderate-to-severe knee OA and not those with mild OA. Second, some patients had undergone TKA on the contralateral side. Third, control of DM is a criterion for TKA; therefore, patients with severe DM (e.g., HbA1c >8.0%), macrovascular and microvascular comorbidities that met the criteria for exclusion, and those being treated with insulin injections were not included. Further, all patients with DM in this study were taking DM medication (type and dose of medication unknown), were well controlled (mean HbA1c 6.4%), and had a mean BMI of 27.1. While all patients in the present study met the standard for obesity (BMI ≥25) in Japan and other Asian countries, 49 comparison with Western patients, for whom the standards for obesity differ (BMI ≥30), may not be useful. In addition, the presence of mild comorbidities not meeting the criteria for exclusion and the duration of DM were not adequately investigated. Fourth, accelerometers cannot track certain types of physical activity (e.g., water-related activities and cycling) or distinguish posture. Fifth, physical activity correlated with psychologic, psychosocial, and environmental factors, as well as age, sex, and physical factors.32,37,50 Psychologic, psychosocial, and environmental factors, however, were not investigated in this study. Sixth, this study was a cross-sectional study and could not identify causation.
In this study, we found that older patients with moderate-to-severe knee OA scheduled for TKA that had DM, even mild DM, had lower physical activity than those without DM. Further longitudinal studies will help to clarify the factors affecting physical activity in patients with knee OA.
Conclusion
Among older patients with moderate-to-severe knee OA scheduled for TKA, those patients with DM had lower physical activity than those without DM. The presence of DM, and decreased mobility and balance correlated with a lower step count and a shorter LPA time. Knee-extension muscle strength on the contralateral side correlated with MVPA time. Due to the importance of physical activity for several health parameters, including knee OA and DM, targeted instruction and therapies to improve balance and strengthen knee-extension muscles are needed to increase physical activity levels in patients with moderate-to-severe knee OA planning to undergo TKA and, in the case of comorbid DM, additional instruction to increase physical activity is needed.
Footnotes
Acknowledgements
We would like to thank the study participants. We also acknowledge Naomichi Matsunaga, PT, MS; Jun Mizusawa, PT, MS; Nao Masaoka, PT; and staff members of the Nagoya Orthopaedic and Joint Replacement Clinic (Kitanagoya, Japan) for their assistance with the data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Grants-in-Aid for Scientific Research (JSPS KAKENHI; grant no. JP19K19749).