
Abstract
Purpose
It was aimed to reveal the relationship between CRP level after knee arthroplasty and gender difference and arthroplasty type.
Methods
Preoperative and postoperative (1st and 7th day, 1st and 3rd months) CRP values of the patients who underwent TKA or UKA were examined. The data were compared by categorizing them into primary male-female, secondary TKA-UKA groups.
Results
967 patients were included in the study (151 male, 685 female in the TKA group and 25 male, 106 female in the UKA group) In the TKA group, the mean age was 67.38 in males and 65.54 in females. In the UKA group, the mean age was 58.72 in males and 57,63 in females. CRP values were found to be statistically significantly lower in females compared to males in the preoperative period, postoperative 1st and 3rd months in patients who underwent TKA (p < .05). In the UKA group, it was found to be significantly lower in females in the preoperative period and at the postoperative 3rd month, p < .05). When the CRP values and their effect on the course of arthroplasty were evaluated according to the type of arthroplasty, there was no significant difference between the CRP values of the preoperative patients (p = .686). In addition, in the comparison made on the postoperative 1st day, 1st week, 1st month, and 3rd month, CRP values of the patient who underwent UKA were found to be significantly lower (p < .05). When analyzed separately by arthroplasty type, postoperative CRP values decreased to normal limits in 96.3% of patients who underwent TKA and 98.5% of patients who underwent UKA in the third month.
Conclusions
Our study showed that the uncomplicated course of CRP after TKA and UKA is gender-specific, and higher CRP values are observed in males than in females. The UKA group exhibited significantly lower postoperative CRP levels than the TKA group.
Introduction
Despite surgical and technological advances, postoperative infections are one of the most devastating complications of knee arthroplasty and affect approximately 1%–3% of all total knee arthroplasty (TKA) cases.1–4 Even if the infection is eradicated after the treatment of periprosthetic joint infections (PJI), it may result in decreased knee or hip joint function and a decrease in the patient's quality of life. If revision joint prosthesis cannot be applied in the treatment of PJE, arthrodesis, amputation, and permanent resection arthroplasty are other treatment options. 5 PJE is a disease with high morbidity and may even result in mortality. 5 The most important way to reduce morbidity and mortality is early diagnosis and treatment. 6 There are many tests used both preoperatively and peroperatively for the diagnosis of PJE, but no diagnostic method has high sensitivity and high specificity. 7 Serum C-reactive protein (CRP) is the most commonly used test in the diagnosis of PJE, as it is in all infections because it is simple and inexpensive.8–12 In addition, CRP has been shown to be one of the most sensitive parameters in the evaluation of infection treatment outcomes. 13
There is no clear consensus in the literature on the effect of patient-dependent and patient-independent factors on CRP values after knee arthroplasty. In particular, the potential effect of patient gender on CRP values after TKA is unclear.14,15 In a study investigating the gender specificity of CRP values after unicondylar knee arthroplasty (UKA), no difference was demonstrated between males and females. 16 Conversely, Windisch et al. 17 showed for the first time that CRP values were gender-specific in the first 10 days after TKA. In addition, it may be difficult to distinguish between elevated CRP caused by postoperative infection and elevated CRP caused by surgery. The time-dependent course of CRP is important for the detection of early postoperative infection. For this reason, knowing when CRP values return to normal in the postoperative period may be important in differentiating PJE from surgery-related CRP elevation. This study was aimed primarily to investigate the effect of gender difference on CRP values and course and, secondarily, the effect of knee arthroplasty type (TKA and UKA) on CRP values and course.
Materials and methods
The study was designed as a retrospective cohort study after local ethics committee approval (No:KAEK-2022-12/19). The data recording file system of 2076 patients diagnosed with knee osteoarthritis and underwent either total knee arthroplasty (TKA) or unicompartmental knee arthroplasty (UKA) between January 2010 and December 2021 was examined. Out of these patients, 1823 underwent TKA, while 253 underwent UKA. Preoperative and postoperative (1st and 7th day, 1st and 3rd months) CRP values of the patients examined. Patients with inflammatory arthritis or inflammatory disease, a history of cancer, no CRP values, and patients with complications were excluded from the study. Preoperative and postoperative (1st and 7th day, 1st and 3rd months) CRP values of the patients examined. Patients with inflammatory arthritis or inflammatory disease, underwent revision arthroplasty, a history of cancer, no CRP values, and patients with complications were excluded from the study. Major surgical complications can be listed as recorded late and early joint infections, surgical site infections, revision surgery, perioperative fractures, urinary or intestinal infections, and pulmonary embolism. A standard surgical technique was applied to the patients by a single surgeon. Spinal block and spinal anesthesia were used as routine anesthesia methods, but when these methods were ineffective, general anesthesia was added. A standard parapatellar approach with a tourniquet was applied to each case. Femoral, tibial, and patellar components were fixed using polymethylmethacrylate cement containing gentamicin. A negative pressure hemovac drain was used and removed on the first day after surgery. All patients were mobilized on the first postoperative day.
CRP was measured using the latex particle-enhanced nephelometric immunoassay on the BN ProSpec analyzer (Dade Behring, Germany) and expressed in milligrams/deciliter (mg/dl). The CRP normal reference range of the device used in our center is 0–25. Primarily, the effect of gender difference on CRP values and course, and secondarily, the effect of knee arthroplasty type (Total or Unicondylar knee arthroplasty) on CRP values and course were examined.
Statistical analysis
Statistical analysis was performed using SPSS version 22 (SPSS Inc., IBM, NY, USA). Categorical variables were given as frequency and percentage, while numerical variables were given as mean values. After the normalization tests, the Mann-Whitney U test was used to compare the means of numerical data between the two groups. p values less than .05 were considered statistically significant.
Results
Comparison of the mean age of the patients according to the type of arthroplasty applied.

Man Whitney U test.
TKA:Total Knee Arthroplasty, UKA:Unicompartmental Knee Arthroplasty.
Comparison of age values of groups by gender.

Man Whitney U test.
TKA:Total Knee Arthroplasty, UKA:Unicompartmental Knee Arthroplasty.
Comparison of CRP values of patients who underwent TKA by gender.

Man Whitney U test.
TKA:Total Knee Arthroplasty, M:male, F:female.
Normal CRP value:0-25.
Comparison of CRP values of patients who underwent UKA by gender.
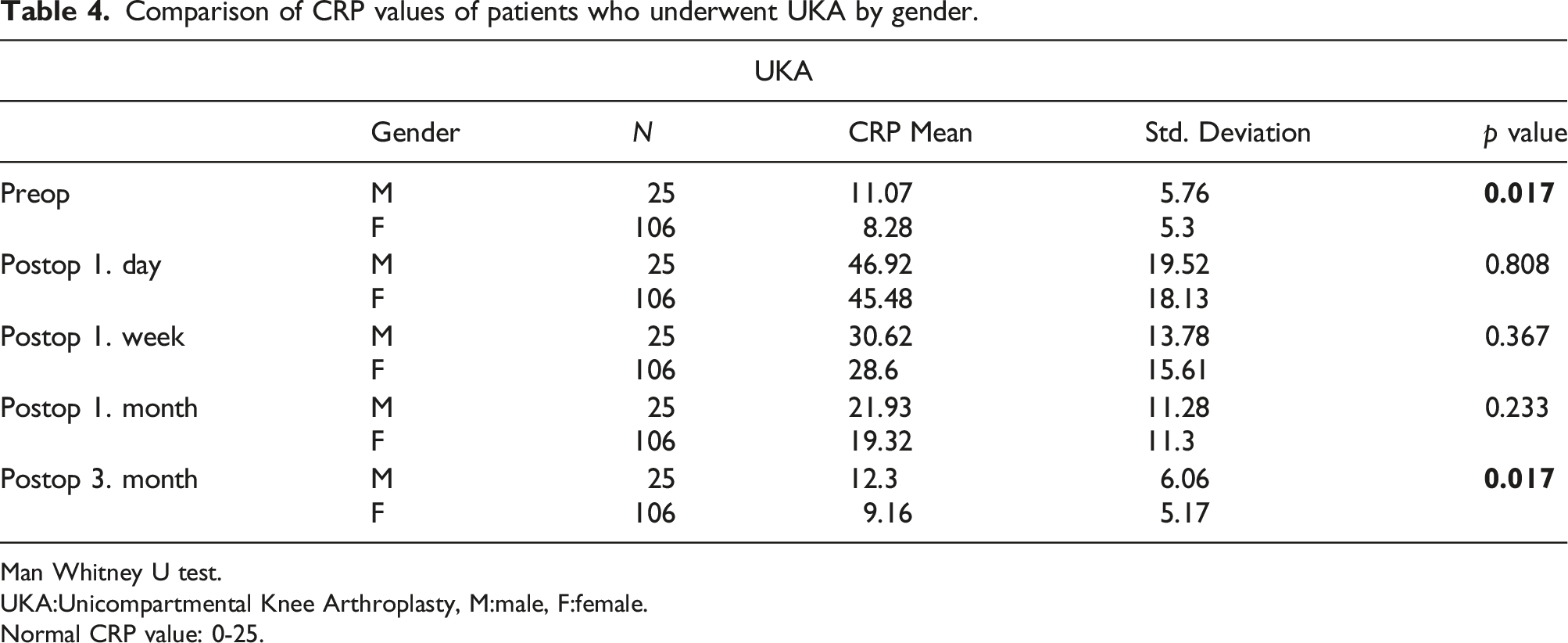
Man Whitney U test.
UKA:Unicompartmental Knee Arthroplasty, M:male, F:female.
Normal CRP value: 0-25.
Comparison of CRP values according to arthroplasty type.
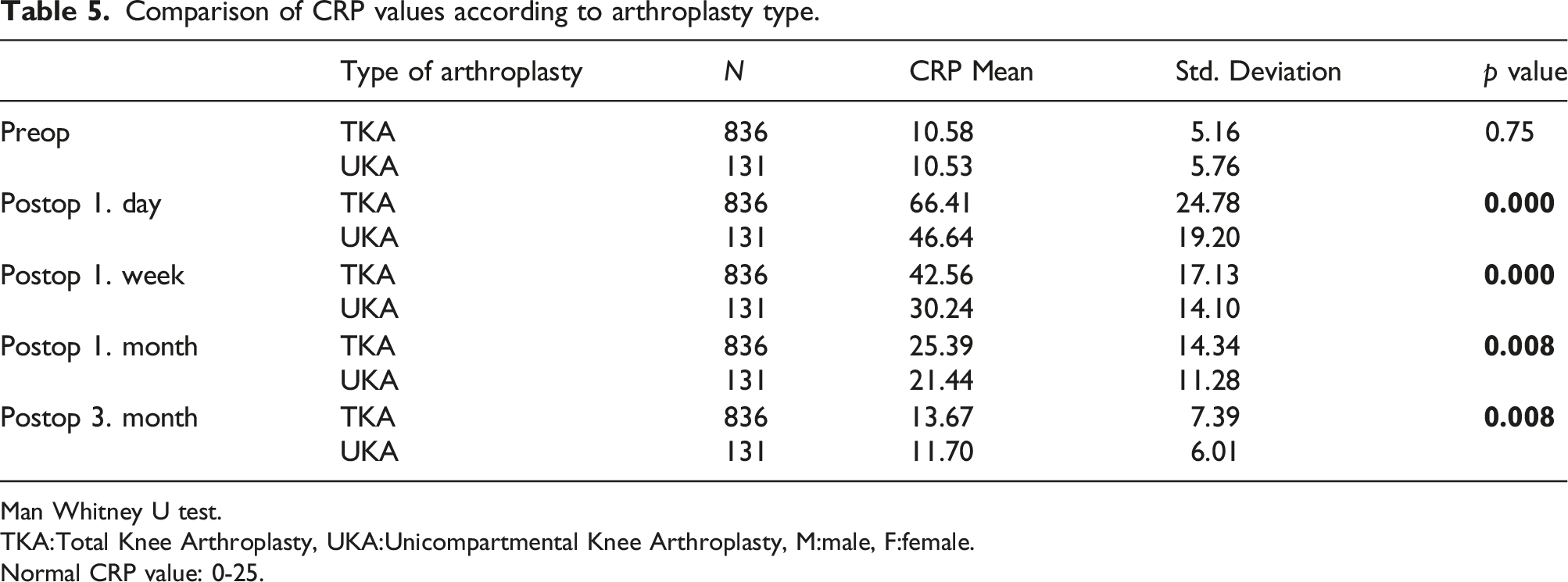
Man Whitney U test.
TKA:Total Knee Arthroplasty, UKA:Unicompartmental Knee Arthroplasty, M:male, F:female.
Normal CRP value: 0-25.
CRP values of patients who underwent TKA in the postoperative period.

TKA:Total Knee Arthroplasty.
CRP values of patients who underwent UKA in the postoperative period.

UKA:Unicompartmental Knee Arthroplasty.
Discussion
In summary, our study shows that CRP level after knee arthroplasty is associated with gender difference. In addition, postoperative CRP values of patients who underwent UKA were generally lower than those of patients who underwent TKA. In the 3rd postoperative month, CRP values decreased to normal limits in 96.3% of the patients who underwent TKA and 98.5% of the patients who underwent UKA.
Infection following joint arthroplasty is a primary concern for surgeons. Despite the availability of multiple modalities, the diagnosis of PJE remains a challenge. 18 The CRP value is often used to detect PJE. In addition, it is widely used to investigate the course of postoperative inflammation after TKA.9,14,19 Although there are many studies on CRP values after TKA, the potential effect of patient gender is not clear enough. 17 An anthropometric study demonstrated a gender-specific course of CRP independent of specific operations. 20 Larsson et al. 16 evaluated the postoperative course of CRP after UKA according to the gender of the patients and stated that CRP was independent of gender. In contrast, Windisch et al. 17 emphasized for the first time that the course of CRP in the first 10 days after TKA is gender specific. A higher course of CRP in males after total hip arthroplasty and spine surgery has been confirmed in other studies.21,22 Our study data support the literature. In addition, according to the literature review we conducted, we believe that our study data is the first study to examine the gender difference in the course of CRP up to the 3rd month after arthroplasty.
It is unclear how gender difference affects the CRP level after arthroplasty. Sex hormones may cause a variation in the inflammatory and hemostatic response. Angele et al. 23 stated that sex hormones have an effect on the post-traumatic immune response. It has also been reported in studies that the anti-inflammatory response elicited by higher testosterone levels in males is reduced.24,25 Siennicka et al. 26 In their study investigating serum levels of inflammatory and hemostatic markers in patients after acute coronary syndrome, they observed a variation in the inflammatory and hemostatic response between males and females after acute coronary syndrome and observed a higher CRP and IL-6 level in male patients than in females. In a multicenter study evaluating clinical outcomes in severely injured adults with blunt hemorrhagic shock, serum levels of IL-6, which increases CRP release, were statistically higher in males than females. 27 In addition, Sperry and Minei 25 reported a higher IL-6 level in males after traumatic injury and hemorrhagic shock. Bohl et al. 28 pointed out that the male gender is a risk factor for postoperative sepsis after total joint arthroplasty and supports the thesis that the inflammatory response after surgery is gender-dependent.
In addition, the severity of surgical trauma may also affect the CRP level. 29 Larson et al. 16 showed that the postoperative CRP increase depended on the type of tissue affected, such as fat, bone, and muscle. Watt et al. 15 showed that a higher level of CRP would be associated with increased surgical trauma. In conclusion, greater tissue damage during the surgical procedure in males may explain the higher CRP level. This can theoretically be explained by the larger male bones, the more stimulating cells (macrophages and platelets), and the greater release of proinflammatory mediators. 30 In our study, CRP values were significantly lower in patients treated with UKA than in patients treated with TKA. Our data support that tissue damage has an effect on the CRP value after surgery. Because less bone and soft tissue are traumatized in UKA, it causes a lower CRP rise compared to traditional TKA. Shen et al. 19 compared CRP levels after four different types of arthroplasty. He found that CRP levels after hip resurfacing and computer navigation-assisted TKA were lower than those after conventional primary total hip arthroplasty and TKA. It can be assumed that less or no trauma to the medullary space in UKA would explain the lower CRP level. Our study data shows the long-term course of CRP, including data at the 1st and 3rd months after surgery. We believe these results can guide the course of CRP after knee arthroplasty without complications in male and female patients. It can contribute to the interpretation of early and late postoperative CRP values.
In conclusion, our study findings suggest that CRP increase in both sexes is similar due to the trauma caused by surgery in the early postoperative period. However, after the decrease in the effect of trauma in the late postoperative period, CRP again shows a similar course as in the preoperative period due to gender differences. This indicates that gender plays a significant role in the long-term course of CRP after arthroplasty.
Limitations
The retrospective design of the study was a natural limitation. The unequal sample size of the male and female groups was another limitation of our study. The CRP value taken from the patients' blood shows the systemic inflammatory response. This response may be caused not only by surgery but also by inflammation from other parts of the body. The most important disadvantage of this study is that local inflammation was not examined from the synovial fluid in the knee, and a systemic inflammatory test was used instead. Inflammation in another part of the patient during the test will increase the CRP value. Another limitation is that the tobacco use of the patients is not questioned. This may affect CRP values. Other inflammatory markers were not measured in our study besides CRP to confirm its course.
Conclusions
Our study showed that the uncomplicated course of CRP after TKA and UKA is gender-specific, and higher CRP values are observed in males than in females. The UKA group exhibited significantly lower postoperative CRP levels than the TKA group.
Footnotes
Authors contributions
Study conception and design: HA, OB, Data collection: HA,YSK,OB, Drafting of the article: HA, OB,YSK, Data analysis and interpretation: HA, OB,YSK, Critical revision of the article: HA, YSK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical Principles of Research: Ethies committee approval with the registration number SÜKAEK-2022 12/19 was received from the Clinical Research Ethics Committee of Health Sciences University Samsun Training and Research Hospital.
Consent
Written informed consent from participants was not required because the study was retrospective and analyzed anonymized data with no risk to the patients.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to privacy concern of participants but are available from the corresponding author on reasonable request.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.