
Abstract
Background
Serotonin (5-HT) precursors regulate bone remodeling. This study aims to investigate the correlation of plasma 5-HT precursors and metabolite with bone mineral density (BMD) and bone turnover markers in postmenopausal osteoporosis (PMOP) patients.
Methods
The age, body mass index (BMI), and years since menopause (YSM) were documented for 348 postmenopausal women in normal/osteopenia/osteoporosis (OP) groups, with lumbar spine and femoral neck BMD measured. Serum bone turnover markers (PINP/β-CTX) and plasma 5-HT, 5-HT precursors (Trp/5-HTP) and metabolite (5-HIAA) were measured by ELISA. OP patients were allocated to high/low expression groups following ROC analysis of 5-HT/Trp/5-HTP/5-HIAA. The relationship of plasma 5-HT/Trp/5-HTP/5-HIAA, BMD, and bone turnover markers with PMOP was analyzed using logistic regression analysis. The correlation of plasma 5-HT/Trp/5-HTP/5-HIAA with BMD and bone turnover markers was analyzed using Pearson’s correlation analysis, followed by logistic regression analysis of the relationship between plasma 5-HT/Trp/5-HTP/5-HIAA and BMD, bone turnover markers and PMOP.
Results
BMI, YSM, BMD and PINP, and β-CTX levels differed among groups. Levels of plasma 5-HT precursors/metabolite were increased in OP patients. Individuals with high 5-HT precursors/metabolite levels had low BMD and high PINP/β-CTX levels. The 5-HT precursors/metabolite negatively-correlated with BMD and positively-correlated with PINP/β-CTX. BMI, YSM, BMD, and PINP/β-CTX/Trp/5-HTP/5-HT related to PMOP and were independent risk factors for OP.
Conclusion
Plasma 5-HT precursors and metabolite negatively-correlate with BMD and positively-correlate with PINP/β-CTX in PMOP patients. Peripheral 5-HT precursors and metabolite level may be a new direction of treatment of PMOP and bone metabolism-related disorders.
Keywords
Introduction
Osteoporosis (OP) is a skeletal disease characterized by excessive bone loss, clinically manifested with the worsening of bone mass and microarchitecture and impairment of bone strength, which brings about huge financial burdens and major reductions in the quality of life.1,2 Postmenopausal OP (PMOP) is the most frequent kind of OP. 3 The high prevalence of OP in postmenopausal women is attributed to the fluctuation of hormones, estrogen in particular, and the decrease in bone mineral content since menopause.4,5 PMOP patients face the risk of osteoporotic fractures as high as 30–40%, making it one of the most urgent clinical problems to be solved. 6
Bone mineral density (BMD) assessed by dual X-ray absorptiometry (DXA) and the incidence of osteoporotic fractures are the basis of the operational diagnosis of OP.7,8 PMOP is a high-bone turnover disease with increased bone resorption and bone formation. 6 The markers of bone turnover consist of a constellation of proteins or protein derivatives released by osteoblasts or osteoclasts in the process of bone remodeling. 9 Specifically, procollagen type I N-propeptide (PINP) is a marker for bone formation, and β-C-terminal telopeptide of type 1 collagen (β-CTX) is a bone resorption marker. 10 Although bone turnover markers might not assist in the diagnosis of OP, they help elucidate the pharmacodynamics and effectiveness of OP medications and can be used as an alternative to BMD in monitoring OP therapies. 11 Therefore, an understanding of the relationship of BMD and bone turnover markers with other bone-related parameters is necessary.
Serotonin (5-HT) is a signaling molecule with important implications for bone metabolism and the development and maintenance of mineralized tissues. 12 The 5-HT signaling can produce mixed effects in bone cells. 13 On the one hand, brain 5-HT stimulates bone formation and inhibits bone resorption as a neurotransmitter, and on the other hand, peripheral 5-HT suppresses bone formation and produces the opposite result of bone remodeling as a hormone. 14 In mouse osteoblasts, 5-HT represses cell proliferation through the 5-HT receptor 1B and the transcription factor cyclic adenosine monophosphate responsive element binding. 15 Tryptophan (Trp) generates 5-hydroxytryptophan (5-HTP) under the action of Trp hydroxylase and subsequently generates 5-HT under the catalysis of 5-HTP decarboxylase. 16 The 5-HTP is the precursor of 5-HT and has been extensively applied to elevate 5-HT levels as a dietary supplement. 17 The 5-hydroxyindole acetic acid (5-HIAA) is the catabolite of 5-HT.18,19 In rats with chronic kidney disease, 5-HT and its metabolite 5-HIAA are negatively related to the stiffness of the femur. 20 However, the correlation of 5-HT and its precursors and metabolite with BMD and bone turnover markers remains elusive. The present study was devised to measure the levels of plasma 5-HT and its precursors and metabolite in PMOP patients and to analyze their association with BMD and bone turnover markers.
Materials and methods
Ethics statement
The present clinical trial was reviewed and approved by the Ethics Committee of Beijing Jishuitan Hospital Guizhou Hospital. All participants were fully informed of the study objective and provided the informed consent form.
Study subjects
Altogether 348 postmenopausal women admitted to Beijing Jishuitan Hospital Guizhou Hospital from January 2021 to June 2022 were recruited as study subjects. Participants were allocated to the OP group (N = 143), osteopenia group (N = 120), and normal group (N = 85) according to the T scores: ≤−2.5, OP; −2.5∼−1.0, osteopenia; ≥−1.0, normal bone mass. 21
Inclusion criteria
The inclusion criteria were as follows: 1) aged between 40–80 years, with the duration of menopause >1 year; 2) no administration of drugs affecting bone metabolism, such as bisphosphonates, calcium-containing drugs, glucocorticoid, and vitamin D; 3) with complete general data, and the required information was accessible.
Exclusion criteria
The exclusion criteria were as follows: 1) with severe diseases of the liver, kidney, or hematopoietic system or malignant tumor; 2) severe systemic diseases or other diseases affecting bone metabolism; 3) recent administration of drugs affecting bone metabolism; 4) receiving relevant treatment affecting bone turnover within 3 months.
Sample and data collection
The fasting venous blood samples (6 mL) were collected from the elbow of each study subject and equally divided into two portions. One portion was stored in an anticoagulant-free collection tube and placed for 30 min at room temperature for spontaneous agglutination. Afterwards, the blood sample was centrifuged for 20 min at 2000 r/min, and the serum was collected and conserved at −80°C until use. Another portion was placed in a collection tube containing anticoagulant. The collection tube was repeatedly inverted to thoroughly mix the anticoagulant and blood sample. After the mixture stood for 1 h, it was centrifuged, and the supernatant (plasma) was collected and preserved at −80°C. The basic characteristics of all study subjects, including age, body mass index (BMI), and years since menopause (YSM) were recorded. The BMD of lumbar spine and neck of femur was measured using a DXA (Discovery W; Hologic Inc, Waltham, MA, USA). The T values were estimated according to the reference range of the instrument manufacturer.
Enzyme-linked immunosorbent assay
The levels of serum PINP and β-CTX were determined using human PINP (Qiongge Biotechnology, Wuhan, China) and β-CTX ELISA kit (Yipu Biotechnology, Wuhan, China) as per the instructions. The levels of plasma Trp, 5-HTP, 5-HT, and 5-HIAA were measured using human Trp (Jianglaibio, Shanghai, China), 5-HTP, 5-HT, and 5-HIAA ELISA kits (Camilo, Nanjing, China) following the specifications.
Statistical analysis
Statistical analysis and data plotting were carried out using SPSS 21.0 (IBM Corp, Armonk, NY, USA) and GraphPad Prism 8.01 (GraphPad Software, San Diego, CA, USA). Measurement data are described as mean ± standard deviation. The difference between groups was analyzed using t test, and the difference among groups was analyzed using one-way analysis of variance. The levels of plasma Trp, 5-HTP, 5-HT, and 5-HIAA in OP patients were analyzed using the receiver operating characteristic (ROC) curves. The correlation of plasma 5-HT precursors and product of metabolism in OP patients with BMD and bone turnover markers was analyzed using the Pearson correlation analysis. The relationship of plasma 5-HT precursors, product of metabolism, BMD, and bone turnover markers with PMOP was analyzed using multivariate logistic regression analysis.
Results
Clinical baseline characteristics of the population enrolled
Clinical baseline characteristics of the population enrolled.

Note: BMI: body mass index; BMD: bone mineral density; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen; OP: osteoporosis. Pa represents the comparison between the normal group and OP group. Pb represents the comparison between the osteopenia group and OP group. Data are described as mean ± standard deviation. The difference among groups was analyzed using one-way analysis of variance, followed by Tukey’s test.
Comparison of plasma 5-HT, 5-HT precursors (Trp, 5-HTP) and product of metabolism (5-HIAA)
The levels of plasma 5-HT, 5-HT precursors (Trp, 5-HTP) and product of metabolism (5-HIAA) in 348 postmenopausal women were measured using ELISA kits, and the OP group manifested with higher levels than the normal and osteopenia groups (all p < .001, Figure 1(a)–(d)). Comparison of plasma 5-HT, 5-HT precursors (Trp and 5-HTP) and product of metabolism (5-HIAA). (a–d) The levels of plasma Trp, 5-HTP, 5-HT and 5-HIAA were measured using ELISA kits. Data are described as mean ± standard deviation. The difference among groups was analyzed using one-way analysis of variance, followed by Tukey’s test. ***p < 0.001.
Comparison of bone mineral density and bone turnover markers among osteoporosis patients with different levels of plasma 5-HT precursors and metabolite
According to ROC analysis, in OP patients, the area under the curve (AUC) of plasma Trp was 0.7920 (sensitivity: 89.51%, specificity: 56.59%, cut-off value: 84.15) (Figure 2(a)); that of plasma 5-HTP was 0.7876 (sensitivity: 72.73%, specificity: 72.20%, cut-off value: 84.61) (Figure 2(b)); that of plasma 5-HT was 0.8025 (sensitivity: 58.04%, specificity: 84.39%, cut-off value: 83.58) (Figure 2(c)); and that of plasma 5-HIAA was 0.7749 (sensitivity: 81.12%, specificity: 60.49%, cut-off value: 17.75) (Figure 2(d)). Subsequently, OP patients were assigned to the low Trp level and high Trp level groups, low 5-HTP level and high 5-HTP level groups, low 5-HT level and high 5-HT level groups, and low 5-HIAA and high 5-HIAA level groups based on the ROC critical values of Trp, 5-HTP, 5-HT, and 5-HIAA. The BMD and levels of bone turnover markers were compared between groups. Relative to OP patients with low levels of Trp, 5-HT, and 5-HIAA, OP patients with high levels exhibited decreased BMD of lumbar spine and neck of femur (all p < .0001), and increased levels of PINP and β-CTX (all p < 0.0001) (Table 2, Table 3, Table 4); OP patients with high level of 5-HTP had decreased BMD of lumbar spine and femoral neck (p < .0001; p = .0002), and elevated levels of PINP and β-CTX (all p < .0001) compared to the OP patients with low levels of 5-HTP, respectively (Table 5). Comparison of BMD and bone turnover markers among OP patients with different levels of plasma 5-HT precursor and metabolite. The ROC curves of plasma Trp, (a) 5-HTP, (b) 5-HT, and (c) 5-HIAA, (d) in OP patients. Comparison of BMD and bone turnover markers between the low Trp level and high Trp level groups. Note: BMD: bone mineral density; Trp: tryptophan; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen. Comparison of BMD and bone turnover markers between the low 5-HT level and high 5-HT level groups. Note: BMD: bone mineral density; 5-HT: serotonin; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen. Comparison of BMD and bone turnover markers between the low 5-HIAA level and high 5-HIAA level groups. Note: BMD: bone mineral density; 5-HIAA: 5-hydroxyindoleacetic acid; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen. Comparison of BMD and bone turnover markers between the low 5-HTP level and high 5-HTP level groups. Note: BMD: bone mineral density; 5-HTP: 5-hydroxytryptophane; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen.




Correlation of plasma 5-HT precursors, product of metabolism, bone mineral density and bone turnover markers with osteoporosis
Correlation of plasma 5-HT precursors and product of metabolism with BMD and bone turnover markers in OP patients.
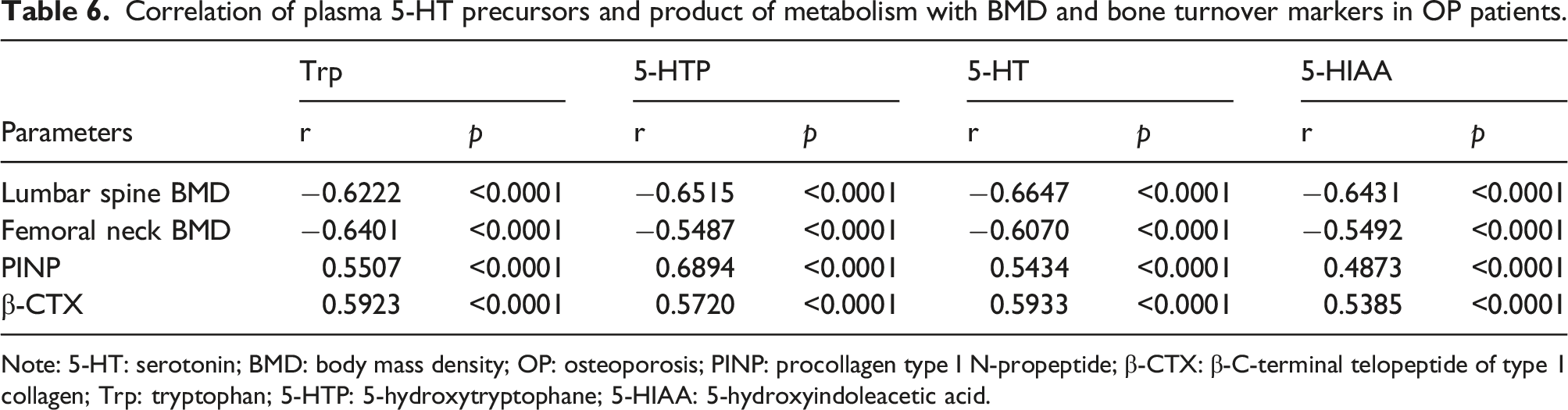
Note: 5-HT: serotonin; BMD: body mass density; OP: osteoporosis; PINP: procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen; Trp: tryptophan; 5-HTP: 5-hydroxytryptophane; 5-HIAA: 5-hydroxyindoleacetic acid.
Relationship of plasma 5-HT precursors and metabolite with bone mineral density and bone turnover markers in postmenopausal osteoporosis patients
Relationship of plasma 5-HT precursors, product of metabolism and BMD and bone turnover markers in PMOP patients.

Note: 5-HT: serotonin; BMD: body mass density; OP: osteoporosis; BMI: body mass index; PINP, procollagen type I N-propeptide; β-CTX: β-C-terminal telopeptide of type 1 collagen; Trp: tryptophan; 5-HTP: 5-hydroxytryptophane; 5-HIAA: 5-hydroxyindoleacetic acid; OR: odds ratio; CI: confidence interval.
Discussion
Postmenopausal osteoporosis, as the most prevalent type of low bone mass, seriously affects approximately 10% of women aged more than 60 years, contributing to increased morbidity and significant loss of independence in the long run. 22 The serum 5-HT level is a negative predictor of total and trabecular volumetric BMD and plays a physiological role in the regulation of bone mass. 23 The present study elicited that 5-HT precursors and metabolite are inversely associated with lumbar spine and femoral neck BMD and positively correlated with bone turnover markers PINP and β-CTX in PMOP women.
There is evidence that plasma 5-HT is an effective inhibitor of bone formation. 24 An increased level of circulating 5-HT has been documented in dextran sodium sulfate-inflamed mice with decreased trabecular and cortical bone parameters. 25 Patients with idiopathic OP manifest decreased Trp levels. 26 Patients with neuroendocrine tumors tend to have increased urinary 5-HIAA levels, as well as a lower BMD at the hip. 27 Our results suggested that PMOP patients had higher levels of plasma Trp, 5-HT, 5-HTP, and 5-HIAA than postmenopausal women with normal bone mass and osteopenia. In OP, BMD is the most extensively used parameter in assessing bone strength. 28 PINP and β-CTX, biochemical markers of bone turnover, are increased in OP patients with fracture. 29 Our results showed significantly lower lumbar spine BMD and femoral neck BMD and higher PINP and β-CTX levels in postmenopausal women with OP, than those with osteopenia and normal bone mass.
A previous study has documented that serum 5-HT level is inversely associated with BMD in rats. 30 In women, decreased BMD is correlated with serotonergic antidepressant use. 31 Patients suffering from neuroendocrine tumors have decreased hip BMD and increased urinary 5-HIAA. 27 Trp-linked metabolites are highly correlated with BMD. 32 A few Trp metabolites can even decrease BMD and increase fracture risks. 33 Likewise, our results illustrated decreased lumbar spine and femoral neck BMD in PMOP patients with relatively high levels of Trp, 5-HTP, 5-HT, and 5-HIAA. Furthermore, 5-HT precursors and metabolite are inversely associated with BMD in lumbar spine and neck of the femur in PMOP patients. The 5-HT is a regulator of bone turnover, whose increase can be induced by supplemental 5-HTP. 34 The use of selective 5-HT reuptake inhibitors is in association with changes in bone turnover markers in young men . 35 The plasma 5-HIAA is associated with osteocalcin, a marker of bone formation, in patients with carcinoid syndrome. 36 Walsh, J. S et al. 36 pointed out the positive correlations of whole-blood 5HT with osteocalcin, PINP, and CTX in healthy individuals. Bone turnover markers, which are internationally recognized as a relatively sensitive indicators of bone turnover, could only reflect the rapidity of bone loss and couldn’t be used in clinical diagnosis of OP. 9 To diagnose OP, a history of fragility fracture and BMD measured by dual-energy X-ray absorptiometry are still needed. 37 Meanwhile, there is no consensus on the standard reference interval for bone turnover markers, and thus determining the bone changes is difficult. 38 A previous study reported that 5-HT manipulates bone remodeling via two different pathways. 14 As a consequence, we continued to investigate the association of plasma 5-HT precursors and metabolite with BMD, Bone turnover markers in PMOP patients in this study. Consistent with the above findings, our results delineated that PMOP patients with high levels of 5-HT precursors and metabolite present elevated levels of bone turnover markers, and further evinced the adverse correlation of 5-HT, 5-HT precursors and metabolite with BMD and the positive associations of 5-HT, 5-HT precursors and metabolite with bone turnover markers PINP and β-CTX.
Patients with type 2 diabetes mellitus complicated with OP show lowered BMI. 39 YSM is associated with the occurrence of postmenopausal osteoporotic fractures. 40 The BMI and YSM varied among PMOP patients and postmenopausal women with normal bone mass and osteopenia. Furthermore, decreased BMI and increased YSM are risk factors for low bone mass in Singaporean women. 41 Low lumbar spine and total hip BMD is a risk factor for primary and recurrent fractures in PMOP patients. 42 Femoral neck or spine BMD is a risk factor for scanographic bone attenuation coefficient ≤145 Hounsfield Units, which represents the best compromise between sensitivity and specificity to screen patients at risk of vertebral fracture. 43 The levels of serum β-CTX and PINP are independent risk factors for OP in both males and females. 44 On the contrary, elevated serum Trp predicts a low risk of incident major osteoporotic fractures in elderly women. 45 The use of selective 5-HT reuptake inhibitors also acts as a risk factor for OP in postmenopausal women. 46 Our results further denoted that not only BMI, YSM, BMD at the lumbar spine and femoral neck, PINP, β-CTX, Trp, and 5-HT, but also 5-HTP are independent factors affecting OP advent in postmenopausal women.
To conclude, the present study found that 5-HT and its precursors and metabolite were negatively linked to BMD and positively correlated with bone turnover markers in patients with PMOP, and patients with high Trp, 5-HTP, 5-HT, and 5-HIAA showed low BMD and high PINP/β-CTX. The results provide a theoretical reference for the regulation of bone metabolism in clinical PMOP patients, which may be a new direction for the treatment of bone metabolism-related diseases such as PMOP. For instance, 5-HT precursors and their metabolite receptor blockers are expected to be a new effective drugs for the treatment of PMOP. Nevertheless, there were limitations in our study. HT performs completely different functions at different synthesis sites. For example, central 5-HT mediates bone reconstruction via a receptor 5-HT2CR for 5-HT in neurons of the ventral medial nucleus of the hypothalamus. 47 Osteoclast production is reduced by repressing RANKL in mice lacking peripheral 5-HT. 48 What’s more, increment in peripheral 5-HT is another possible pathway leading to declined bone mass. For example, 5-HT interferes with the entry of plasma fibronectin into the extracellular matrix of osteoblasts, and plasma fibronectin is the main enzyme substrate of FXIII-A in the extracellular matrix of osteoblasts, and FXIII-A plays an important role in the deposition and quality of the osteoblast matrix. 49 Additionally, the number of cases collected in this experiment is limited, and thereby the results are limited. Therefore, the sample size of the study needs to be expanded to further explore the specific mechanisms of plasma 5-HT precursors and metabolite in PMOP patients.
Footnotes
Authors’ contributions
QYF is the guarantor of integrity of the entire study and contributed to the study design, study concepts, definition of intellectual content, manuscript editing; QYF, XYS contributed to the literature research; LL contributed to the clinical studies; XZZ, ZHC contributed to the experimental studies; XYS, LL contributed to the data acquisition, manuscript review; XYS, XZZ and ZHC contributed to the data analysis; XYS contributed to the statistical analysis, manuscript preparation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Study on bone markers and osteoporosis in postmenopausal women in Guizhou Province (NO.gzwkj2022/179)
Ethics approval and consent to participate
The present clinical trial was reviewed and approved by the Ethics Committee of Beijing Jishuitan Hospital Guizhou Hospital.
Informed consent
All participants were fully informed of the study objective and provided the informed consent form. All procedures were strictly implemented according to the Declaration of Helsinki.