
Abstract
Background
Previous studies lacked adequate quantitative data on sustentaculum tali (ST), especially in Chinese population. The aims of this study are to explore the quantitative morphology of ST in dried bone specimens, and to discuss its implications related to ST screw fixation, talar articular facet variation, as well as subtalar coalitions.
Methods
A total of 965 dried intact calcanei from Chinese adult donors were evaluated. All linear parameters were measured by two observers with a digital sliding vernier caliper.
Results
Most parts of ST body can accommodate a commonly-used 4-mm-diameter screw, but the minimum height of anterior ST is only 4.02 mm. The shapes of the STs are slightly affected by left-right, subtalar facet, but the subtalar coalition may potentially increase the sizes of STs. The incidence of tarsal coalition is 14.09%. Among the osseous connection, there are 58.8% of type A articular surface and 76.5% of middle and posterior talar facet (MTF and PTF) involvement. ROC curve shows that subtalar coalition will be detected when ST length is greater than 16.815 mm.
Conclusions
Theoretically, all the STs can accommodate 4 mm diameter screw, but a 3.5 mm diameter screw is recommended to be placed in the middle or posterior of the small ST for safety. The shapes of the STs are greatly influenced by the subtalar coalition, while they are less affected by left-right, subtalar facet. The osseous connection is common in type A articular surface and always involved in the MTF and PTF. The cut-off value of the length of STs was confirmed as 16.815 mm for predicting subtalar coalition.
Introduction
ST is a special structure in the calcaneus supporting body weight and transmitting force.1–3 According to previous studies, the discussion of ST morphology was mainly concerned with three issues: sustentacular screw fixation in calcaneal fracture, subtalar joint surface, and subtalar coalition.4–6 First, ST is a common fixation site for calcaneal fracture. 4 To precisely place a screw into ST is always a challenge for surgeons, because ST is a small target on the medial side of the calcaneus, and is not always exposed during surgery. So, the screw may cause ST fracture, resulting in the damage of subtalar joints, adjacent tendons and neurovascular structures. 4 However, there is no literature discussing on whether small ST can safely accommodate 4 mm diameter screw. Second, there are three facets over upper side of the calcaneus that are well-established: Anterior Talar Facet (ATF), Middle Talar Facet (MTF) and Posterior Talar Facet (PTF). 5 In some cases, however, the MTF may be contiguous to the ATF for unknown reasons. 5 There is no quantitative analysis on how the contiguous talar facets will influence the size and shape of STs. Third, up to now, far too little attention has been paid to subtalar coalition. Actually, subtalar coalition is a main cause of painful and rigid flat-feet, recurrent ankle sprains and arthritis. 7 Talocalcaneal coalition is the second most common type of subtalar coalition, with an incidence of 1–13%, in which MTF is commonly involved.6,8,9 However, the anatomical structures of subtalar coalitions were not described in detail. Therefore, the aim of this study is to explore the quantitative morphology of STs in dried bone specimens, and to discuss their implications relative to ST screw fixation, talar articular facet variation, and subtalar coalition.
Materials and Methods
A total of 965 dried calcanei (480 left, 485 right), without prominent pathology, with unknown gender, were obtained from the department of anatomy, Southern Medical University. All calcanei samples were obtained with donors’ living wills and the formal consents of their family members. All experiments were regulated under the related law of People’s Republic of China. All linear parameters were measured by two observer with a digital sliding vernier caliper (sensitivity = 0.01 mm). The mean value of them was calculated as the measurement value.
Anatomical measurements
The following were seven quantitative parameters to describe ST morphology (Figure 1). Ⅰ. The heights of ST in anterior (L1), middle (L2), and posterior (L3) sections were measured. The medial surface of ST was equally divided into three sections. The heights of ST in each section were measured as the vertical distance between the upper facet of ST and the groove for flexor hallucis longus tendon (GFHLT). Ⅱ. The length (L4) and width (L5) of ST were measured by using the length and width of GFHLT under ST as replacements. Ⅲ. The maximum longitudinal and transverse diameter of the MTF were measured as the length (L6) and width (L7) of MTF. Schematic diagram of ST measurement: L1: The height of anterior ST; L2: The height of middle ST; L3: The height of posterior ST; L4: The length of ST; L5: The width of ST; L6: The length of MTF; L7: The width of MTF.

Classification of talar articular facets
Three types of calcanei (type A, B and C) with different talar articular facets were defined according to the report of Uygur et al.
5
Three types of calcaneus classified by morphology of talar articular facets. The above images show the upper view of the calcaneus, The below images correspond to the ST of the above image, viewed from inside-below view. Due to The fusion of the ATF and MTF in Type B specimens, the boundary of MTF could not be determined, and The width of MTF could not be measured. Due to the irregular shape of MTF in Type C specimens, it is difficult to measure the width of MTF. In this experiment, the length and width of the GFHLT were used as the length and width of the ST. The height of the ST was measured at the anterior, middle, and posterior parts of the ST. The length, width and heights of the ST, the width of MTF can be measured in all specimens.
Classification of subtalar coalitions
Subtalar coalitions, representing abnormal bridging between tarsal bones, can be osseous, fibrous, or cartilaginous.10,11 Osseous connection: Trabecular bone is found at the bridging. Fibrous connection: Only the cortical bone is found at the bridging, forming a rough bone surface. Cartilaginous connection: Only the cortical bone is found at the bridging, forming a smooth and flat bone surface (Figure 3). 1. Osseous connections; 2. Fibrous connections; 3. Cartilaginous connections; 4. MTF; 5. ATF; 6. PTF.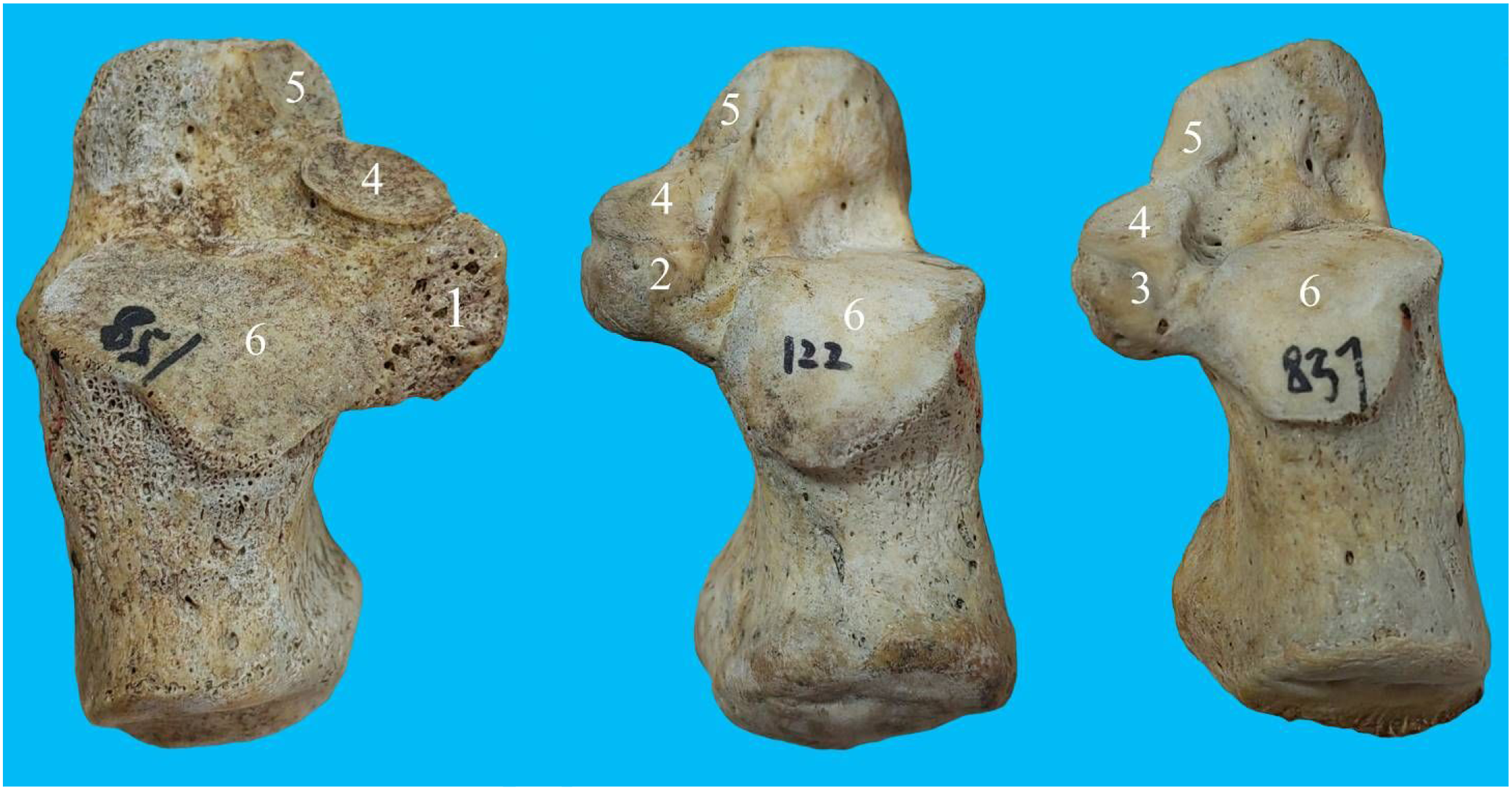
Classification of facet involvement in calcaneus with subtalar coalition
Classifications of facet involvement include:8,12–14 MTF only, MTF and PTF, and PTF only (Figure 4). Classification of facet involvement in subtalar coalitions: 1. Only MTF was involved; 2. Both MTF and PTF were involved; 3. Only PTF was involved.
Analysis of Data
The data were analyzed with SPSS 20.0 software (IBM SPSS Statistics for Windows, IBM Corp, Armonk, NY). The independent t test was used to compare the means of the grouped parameters for left and right, and for Type A and B, respectively. A one-way analysis of variance (ANOVA) helped to compare the means of heights among three ST sections for significant difference. If ANOVA reports significant differences, Bonferroni test or Tamhane’s T2 was performed for multiple comparisons. A one-sample t test was used to compare the means of heights and lengths of STs to a 4 mm diameter screw. Spearman correlation analysis was adopted to investigate the relation between the counting data. Chi-square test was used to analyze the relations among tarsal coalition classifications, facet involvement classifications, and talar articular facet classifications. Unordered multiple classification Logistic regression was used for the prediction of tarsal coalition. A p < 0.05 was considered statistically significant.
Results
Anatomical parameters of ST: Data and comparison with 4 mm diameter screw
Parameters of the size of ST with respect to screw placement (mm).

Differences of ST measurements for left-right groups, subtalar facet groups, subtalar coalition groups, and facet involvement groups
The measurements of ST (mm) Left-right groups Subtalar facet groups Subtalar coalition groups Subtalar facet involvement groups of coalitions.

Data are shown as Mean ± S.D. Independent t test and One-way ANOVA were used for statistical testing.
*Independent t test showed that the height of posterior ST and the width of ST have significant difference between left and right. The height of anterior ST, the length of ST and the length of MTF have significant difference between Type A and Type B subtalar facet groups. *p < 0.05, **p < 0.01.
#One-way ANOVA showed that the height of posterior ST, the length of ST and the width of ST have significant difference among subtalar coalition groups. The height of posterior ST, the length of ST and the width of ST have significant difference between coalition-involved subtalar facet groups. #P < 0.05, ##P < 0.01.
Differences between left-right groups: There are 480 left (49.74%) and 485 right (50.26%) calcanei in this study. Only two parameters are significantly different between left and right, which are the mean height of posterior STs and the mean width of STs. However, the differences of the mean values between these two parameters were both less than one mm, indicating the differences of ST morphology between left and right are inconspicuous.
Differences between subtalar facet groups (Figure 2): In this study, we only investigated the differences between type A and B, due to the lack of specimens in C type. Three parameters showed statistically significant difference of their mean values between A and B types, with all four in B type larger than that in A type, including the height of anterior ST, the length of the MTF and ST The differences of the mean values between these parameters are only around one mm, suggesting that the subtalar facet variations only slightly influence the morphology of ST
Differences between subtalar coalition groups (Figure 3): Three parameters show statistically significant differences of their mean values between subtalar coalition groups and normal group, including the lengths of STs, the widths of STs, and the posterior heights of STs. One-way ANOVA shows the means of the length, the width, and the posterior height of STs in normal group are all significantly smaller than those in the subtalar coalition groups (p < 0.001). However, no difference was found in the length, width, and posterior height of STs among three subtalar coalition groups. These results indicate that subtalar coalition may potentially increase the size of ST
One-way ANOVA shows that the major differences between the subtalar coalition groups and the normal group are the mean values of ST lengthss, ST widths, and posterior ST heights. Therefore, these three variables were used for logistic regression analysis (with unordered multiple classifications) to assess their relations to subtalar coalition. Results show that the logistic model was statistically significant (χ2 = 109.151, p < 0.001). Among these three variables, only ST length showed statistical significance.
Exp B (OR value): When ST length increases one mm, the risks of subtalar coalition for osseous, cartilage, and ligament connection increase by 2.106, 1.395, and 1.531 times, respectively.
ROC (Figure 5): An optimal cut-off value of ST length for diagnosis of subtalar coalitions is 16.815 mm (Sensitivity = 70.6%, Specificity = 69.5%, Area Under the Curve [AUC] = 0.758). Receiver operator characteristic curves (ROC) for the length of ST (Area Under the Curve [AUC] = 0.758).
Cross table of subtalar facet types, Subtalar facet involvement groups of coalitions, and Subtalar coalition groups.

Relations between subtalar facet types, subtalar facet involvement, and subtalar coalition groups
In this study, we investigated the relations between subtalar facets types, subtalar facet involvement of coalitions, and subtalar coalition groups (Table 3). A total of 136 specimens with subtalar coalition were investigated. There are 48 cases (35.29%) of A type subtalar facet, 86 cases (63.23%) of B type and 2 cases (1.47%) of C type (Figure 2). For subtalar coalition groups, there are 29 cases (21.32%) of Fibrous connection, 90 cases (66.18%) of Cartilaginous connection, and 17 cases (12.50%) of Osseous connection (Figure 3). For subtalar facet involvement of coalitions, there are 72 cases (52.94%) involved only MTF, 60 cases (44.12%) involved MTF and PTF, and 4 cases (2.94%) involved only PTF (Figure 4).
Spearman correlation analysis shows that the subtalar coalition groups are weakly correlated to subtalar facet types (r = 0.209, p = 0.017) and subtalar facet involvement groups of coalitions (r = −0.258, p = 0.003). No relation was found between subtalar facet involvement groups and subtalar facet types. Chi-square tests shows that more than half (58.8%) of the osseous subtalar coalitions are type A facet (χ2 = 14.212, p < 0.003). Another result shows that 76.5% osseous connection involved MTF and PTF, while 69% Fibrous connection involved MTF only (χ2 = 12.573, p < 0.008).
Discussion
ST is so important for calcaneal fracture fixation that even with the risks and challenges of techniques, surgeons still choose ST as a reliable fixation site.4,15 Many literature reported the serious consequences of ST screw breach, such as injuries in adjacent facets, tendons, and neurovascular structures.4,16 However, previous studies did not evaluate the safety of commonly-used screws (3.5 or 4 mm in diameter) in terms of ST anatomy.17,18 In this study, the measurements of ST showed that a 4-mm-diameter screw can be applied to most of patients, but some people with a small ST may bear the risk of screw breach if the fixation site is not appropriate. The height of ST is a key indicator to evaluate the screw diameter, as a small ST height can easily lead to screw breach. According to this study, the posterior section of ST is safer for screw fixation than the anterior section since the height of ST increases from anterior to posterior. In this study, the minimum height of ST is at the anterior section, which is 4.02 mm. For these small STs, if screw placement at ST is necessary, a 3.5-mm-diameter screw is recommended. According to Mahato’s study of the Indian population, the mean height of ST is 9.28 mm which is similar to our results, while the mean length of ST is 25.53 mm, which is larger than ours. 1 Different from Mahato’s, our study measured not only the middle section of ST, but also the anterior and posterior sections to determine the height of ST Mahato’s method will be difficult to measure the length of ST when ATF and MTF are contiguous or all three joint surfaces are fused together. This is a possible reason for the inconsistence of ST length.
The ST is the part of the medial bony protrusion above the calcaneus, with the MTF above and the GFHLT below. 19 The medial surface is adjacent to the flexor digitorum longus tendon, and the lateral surface is connected to the calcaneus. 19 The ST is a bony protrusion, and determining the boundary between it and the calcaneus can easily define the range of the ST If the boundary line between the calcaneus and ST is divided from above, it is easily affected by type B and C subtalar facets. When ATF and MTF are contiguous, it is difficult to determine the boundary between ATF and MTF, resulting in the inability to determine the front end of the ST and measure the length of the ST, or inaccurate measurement of the ST length.
The GFHLT is located below ST, and in all specimens, the anterior and posterior ends of the GFHLT are easily identified. Therefore, the length of the GFHLT was chosen as the length of ST in this experiment. The sagittal plane of the lateral edge of the GFHLT was used as the interface between the ST and the calcaneus. This can eliminate the influence of the subtalar facet variations deformation and subtalar coalition.
Previous research has shown that subtalar coalition changes the morphology of ST. 8 MTF may be contiguous with ATF in the anterior of ST, and the posterior of ST occasionally has tarsal coalitions.5,12 Our study found that these changes mostly occur in the anterior and posterior sections of ST In this study, the majority the calcaneus (78%) exhibit type B subtalar articular facets, which is in line with other studies in Turkey, USA, India, and Africa. 5 The rest of calcaneus (about 22%) mostly exhibits type A, while type C is rare. The relationship between the size and morphology of ST has rarely been discussed in the previous literature.5,20 In the study, the subtalar facet variations only slightly influence the morphology of ST
Subtalar coalition is one of the most common tarsal coalitions, received increasing attention by clinicians in recent years.6,21 Subtalar coalition can lead to pain and malfunction of foot and ankle, or even deformity. 22 In this study, the incidence of tarsal coalition is 14%, which is similar to other studies (1–13%).6,8,9 A main cause of tarsal coalition is the failure of mesenchymal separation, presenting fibrous, cartilaginous, or osseous bridging.10,11 The precise location of tarsal coalition is essential for surgical decisions. 13 Some studies suggested that subtalar coalitions mainly occur at MTF and PTF, while other studies showed that more than 1/4 of subtalar coalitions do not involve in MTF.8,12–14 Our study found that subtalar coalitions often take place at the MTF, followed by MTF and PTF. Only four cases do not involve in MTF (only PTF involvement). Surprisingly, we found that calcaneus with osseous subtalar coalition usually have type A articular facets and involve in MTF and PTF. The subtalar coalition may potentially increase the size of ST
In previous studies, the following measurements were commonly used to evaluate the morphological changes of ST: MTF length, the ratio of MTF length/ST length, the ratio of MTF length/posterior ST length, the percentage of the section posterior to the MTF.6,8 These measurement parameters all involve in the length of MTF. However, it was difficult to measure the length of MTF in type B and type C calcaneus. It is difficult to determine the boundary between ATF and MTF. Therefore, the length of MTF is not suitable for the assessment of ST length or the diagnosis of tarsal coalition. In this study, we used the length, width, and posterior height of ST in Logistic regression to establish an association with tarsal coalition. Our results showed that ST length is an important indicator of tarsal coalition. The ROC curve showed the optimal cut-off value of ST length was 16.815 mm for the prediction of tarsal coalition (AUC = 0.758).
Conclusions
The heights and lengths of ST are both greater than 4 mm, and the minimum measured value is 4.02 mm. The heights of ST increase gradually from anterior to posterior part. Therefore, theoretically, ST can accommodate a screw with a diameter of 4 mm. But some ST are very small, which are just a little bit bigger than 4 mm. So, it is recommended to use a 3.5 mm diameter screw and place the screw in the middle or posterior of the small ST for safety. Some interesting rules of tarsal coalitions were found in this experiment: The shape of the ST is slightly affected by left-right, subtalar facet, but the subtalar coalition may potentially increase the size of ST The ratio of tarsal coalition is 14.09%. The osseous connection is common in type A articular surface and often involved in MTF and PTF. The cut-off value of the length of ST for predicting subtalar coalition was confirmed as 16.815 mm.
Abbreviations
ST, Sustentaculum tali; ROC, Receiver operator characteristic curves; ATF, Anterior talar facet; MTF, Middle talar facet; PTF, Posterior talar facet; GFHLT, The groove for the flexor hallucis longus tendon; ANOVA, One-way repeated measure analysis of variance
Footnotes
Acknowledgements
We would like to thank the Department of Anatomy, Southern Medical University for their support in this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Sanming Project of Medicine in Shenzhen(No.SZZYSM202108013) and The Innovation Team and Talents Cultivation Program of National Administration of Traditional Chinese Medicine. (No:ZYYCXTD-C-202003).